
Abstract
Introduction:
Human adenovirus (HAdV) is a common pathogen that can cause acute respiratory infections (ARIs) in children. Adenovirus pneumonia is the most severe respiratory disease associated with HAdV.
Objective:
We aimed to investigate the clinical characteristics of children hospitalized with adenovirus pneumonia in Quanzhou, China, in 2019. We also sought to determine the viral genotype in these cases and explore cases associated with severe adenovirus pneumonia.
Methods:
We collected oropharyngeal swabs from 99 children who were hospitalized with pneumonia in Quanzhou Women and Children's Hospital, these samples were tested for the presence of HAdV. Genotyping of the viruses was performed by real-time polymerase chain reaction. Logistic regression analysis was employed to analyze risk factors related to severe adenovirus pneumonia. The epidemiological data were examined using the Statistical Package for Social Sciences software (SPSS).
Results:
Among the 99 patients in our study, the median age was 21 months. We observed a 4% mortality rate among those diagnosed with adenovirus pneumonia. Adenovirus pneumonia often presents as a coinfection. Lactate dehydrogenase and neutrophil percentages of WBC's were significantly increased in patients with severe adenovirus pneumonia compared with mild HAdV disease. The predominant viral genotypes identified were type 3 and type 7.
Conclusions:
In the Quanzhou area of southeast China, the incidence of adenovirus pneumonia was found to be high among children younger than two years old. Type 7 HAdV was identified as the primary pathogen. A long duration of fever, dyspnea and digestive system complications were risk factors for severe adenovirus pneumonia after HAdV infection.
Clinical Trial Registration number:
ChiCTR2200062358
Introduction
Human adenovirus (HAdV) is a double-stranded DNA virus that lacks an envelope. Currently, 103 genotypes have been reported. With advancements in detection technology, HAdVs can now be categorized into seven species, namely species A-G (ICTV, 2011; Radke and Cook, 2018; Luan et al., 2022). Species B of HAdV, which includes genotypes HAdV-3,7,11,14,16,21,50,55, species C (genotypes 1,2,5,6,57, and species E (genotype 4) are mainly associated with respiratory tract infections in humans (Chehadeh et al., 2018; James et al., 2017; Kendall et al., 2016; Lynch and Kajon, 2016).
HAdV pneumonia is a common and severe community-acquired pneumonia in children (Lynch, et al., 2021; Nagao et al., 2018; Shieh et al., 2022). The typical clinical signs of respiratory tract infections caused by HAdV include fever and respiratory system symptoms. Other accompanying symptoms may include catarrhal conjunctivitis, red rash, and macular papules (Lynch et al., 2016; Takeshi et al., 2010).
HAdV infections are ubiquitous. Indeed, most people show that serological evidence of adenovirus infection before 10 years old and usually experience several adenovirus infections in early childhood (Galiano et al., 2004). Approximately 50% of adenovirus infections result in subclinical disease, meaning there are no apparent symptoms or signs of illness. However, when symptoms do occur, they are usually mild and self-healing, meaning they resolve on their own without requiring specific medical treatment (Lynch et al., 2021).
As a result, most adenovirus infections are not documented, therefore, epidemiological data have been derived from surveillance data and investigations of sporadic outbreaks. In recent years, sporadic outbreaks in children in the United States, the United Kingdom, South Korea, Taiwan, Paraguay, Kenya, and other places have mainly been concentrated in daycare centers, summer camps, and public swimming pools (Binder et al., 2017; Emilio et al., 2012; Faden et al., 2005; Frabasile et al., 2005; James et al., 2017; Kajon et al., 2010; Lin et al., 2019; Lin et al., 2017; Lynch et al., 2016; Magwalivha et al., 2010; Mennechet et al., 2019; Schachor et al., 2019; Takeshi et al., 2010).
Although HAdV can be transmitted by droplets, it is important to note that transmission through the gastrointestinal tract via the fecal-oral route can also occur (Lynch et al., 2021). HAdV 1-7 are the most common worldwide, causing the majority of adenovirus-related diseases. According to data from the national adenovirus reporting system of the United States, types 1, 2, 3, 4, 7, and 14 were the most commonly reported HAdV types in the United States from 2003 to 2016; these types accounted for 85.5% of all types reported (n = 1283) (Binder et al., 2017).
Studies of U.S. military personnel have shown that genotypes 3, 4, and 21 are the most common among them. Group B adenoviruses, which include types 3, 7, 14, and 21, have been associated with outbreaks of adenovirus pneumonia (Binder et al., 2017; Kajon et al., 2019; Metzgar et al., 2007). Infants and children are generally susceptible to HAdV. Data from respiratory adenovirus detection between 1997 and 2015 show that among the reported outbreaks, types 3 and 7 accounted for 24.97% (240/961) and 62.33% (599/961) of cases, respectively (Zhao et al., 2020).
Many severe pediatric adenovirus pneumonia cases were reported in China in 2019. Therefore, the Chinese mainland issued an expert consensus on diagnosing and treating adenovirus (National Health Commission and National Administration of Traditional Chinese Medicine, 2019).
At present, the classification, main manifestations, and prognosis of HAdV infections are not precise, and there is a relative scarcity of relevant data on past and recent HAdV infections in different regions of China. Based on these findings, clinical data for children with adenovirus pneumonia in our hospital in Quanzhou, which is situated in southeast China, were collected in 2019. The data collected include information on sex, age, and clinical characteristics of children diagnosed with severe adenovirus pneumonia. We determined the viral genotype associated with infection to provide a reference for early clinical identification, treatment, and prevention of adenovirus pneumonia in children as well as for vaccine development.
Methods
Research subjects
The research subjects in this study consisted of those who were suspected of having acute respiratory tract infections and were subsequently diagnosed with pneumonia through chest radiography. Moreover, these patients were predicted to have adenovirus pneumonia using polymerase chain reaction (PCR) and were hospitalized at Quanzhou Children's Hospital from January 1, 2019 to December 31, 2019. Ethical consent was obtained for this study.
However, it should be noted that the study subjects were not selected continuously due to the limited experimental conditions. The inclusion criteria for this study were as follows: (1) aged over 28 days and <14 years; (2) clinical symptoms, epidemiology, contact history, and detection results of adenovirus nucleic acid and meeting the diagnostic criteria of HAdV pneumonia (National Health Commission and National Administration of Traditional Chinese Medicine, 2019); and (3) availability of complete clinical data for analysis. The exclusion criteria were as follows: (1) presence of mental illness or cognitive impairment; (2) inadequate records with essential data, preventing a complete statistical analysis.
Classification criteria for pneumonia
In total, 99 children were diagnosed with adenovirus pneumonia according to the Guidelines for the Diagnosis and Treatment of Adenovirus Pneumonia in children (2019 edition) published by the National Health Commission and National Administration of Traditional Chinese Medicine (2019); we divided mild adenovirus pneumonia into severe adenovirus groups (Bradley et al., 2011).
Investigation and methods
Survey content
General demographic information, laboratory tests, clinical manifestations, laboratory examinations, adenovirus genotypes, and treatments were collected for the purpose of retrospective analysis.
Laboratory diagnosis
HAdV identification
Pathogen nucleic acids were extracted directly from clinical specimens using a nucleic acid extraction kit (Biogerm) along with nucleic acid extraction instruments (Biogerm). A multiplex reverse transcription-PCR was performed to screen for 15 different respiratory pathogens (respiratory syncytial virus, influenza virus A and B, parainfluenza virus 1-3, HAdV, human rhinovirus, human coronavirus, Streptococcus pneumoniae, Mycoplasma pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Acinetobacter bambini, and Bordetella pertussis) simultaneously by using a commercial kit (Biogerm: 1. Limit of detection: 500 copies/mL. 2. Positive/Negative compliance rate: 100%. 3. Linear detection range: 2 × 103-1 × 108 copies/mL. 4. Specificity: all samples of the target can be detected, and there is no crossover with other types). Adenovirus-positive specimens were further analyzed.
HAdV molecular typing
For typing of HAdV, hexon gene sequences were obtained for all adenovirus-positive specimens; PCR was performed with Platinum PCR SuperMix (Invitrogen) following the manufacturer's instructions. A partial hexon gene was amplified using the primer pair HAdV-Forward (5′-TGTAAAACGACGGCCAGTTTCCCCA-3′) and ADV-Reverse (5′-CAGGAAACAGCTATGACCCCCTGGT-3′). PCRs were conducted in a total volume of 50 μL containing Platinum PCR SuperMix (45 μL), primer F (10 μM, 0.5 μL), primer R (10 μM, 0.5 μL), and DNA template (4 μL).
Amplification was performed with the following thermal profile: 94°C for 10 min; 34 cycles of 94°C for 30 s, 52°C for 30 s, and 72°C for 30 s; and a final extension at 72°C for 10 min. The PCR products were purified and sequenced using the Sanger sequencing method and an ABI3730xl DNA Analyzer. The assembled DNA contigs were characterized by The Basic Local Alignment Search Tool (BLAST) survey of the National Center for Biotechnology Information (NCBI) GenBank database. The molecular type of each clinical specimen was determined in accordance with the highest sequence identity.
Statistical analysis
Statistical Package for Social Sciences (SPSS, version 26.0) software was used for statistical data analysis. Counting data are expressed as percentages (%), and nonnormally distributed data are described as the median and interquartile interval [M (P25, P75)]. Data conforming to a normal distribution are expressed as the mean ± standard deviation (±).
The chi-square test was employed to analyze categorical variables and the t test to analyze continuous data. Multivariate logistic regression analysis included the p-value of univariate logistic regression analysis at <0.05. Variables were assessed as risk factors associated with severe pneumonia. Independent variables were selected from logistic regression analysis positive: likelihood ratio (LR). p-Value <0.05 was considered statistically significant.
Results
Basic information
A total of 99 children were included in the study; the demographic characteristics and clinical features of hospitalized children with severe and mild adenovirus pneumonia are shown in Table 1. Among the 99 patients, the youngest was 1 month old, the oldest was 9 years old, and the median age was 21 months. Epidemiological investigation showed that most children with HAdV pneumonia were <5 years old, and 50% of children with severe HAdV pneumonia were <2 years old, so 2 years was chosen as the dividing line (Wang et al., 2021; Yu et al., 2021).
Basic Characteristics of Children with Severe and Mild Adenovirus Pneumonia
Represents the chi-square value for the chi-square test.
Represents the t value for the t-test.
The incidence HAdV pneumonia was highest in patients under 2 years of age. Among the affected individuals, there were 58 males and 41 females. There was no significant correlation between severe or mild adenovirus pneumonia and age or sex. The majority of cases of adenovirus pneumonia occurred in spring and summer (71.7%), with the highest number of cases observed in May. However, there was no significant difference in the number of children affected by adenovirus pneumonia in different seasons (p > 0.05).
For adenovirus pneumonia, the average length of hospital stay was 14 days. Among these cases, the average number of hospital days for mild and severe adenoviral pneumonia was 11 and 15 days, respectively. The average cost of hospitalization was ¥ 20,000, that for severe adenovirus pneumonia was ¥ 25,000, and that for mild adenovirus pneumonia was ¥ 10,000. Compared with mild adenovirus pneumonia, the length of hospital stay and cost of hospitalization increased significantly in the severe group (p < 0.05). The mortality rate of adenovirus pneumonia was 4%, However, there was no significant correlation between the mortality rate and the presence of underlying disease (p > 0.05).
Clinical features
Common symptoms included fever (92.9%), and the main fever pattern was retention fever (∼75%) in addition to respiratory symptoms such as cough (96%), expectoration (96%), and dyspnea (57%). Some children may present with gastrointestinal symptoms (∼17%). When comparing severe pneumonia with mild pneumonia, there is a higher likehood of dyspnea being accompanied by severe pneumonia, with rates of 54% and 3%, respectively. This difference is statistically significant with a p-value of <0.05 (Table 2).
Clinical Features of Severe and Mild Adenovirus Pneumonia
(1) “*” indicates that the total sample size of the fever type was 92; the remaining 7 had no fever symptoms. (2) “a” indicates chi-square test value and “b” indicates t-test value. (3) “-” means that the statistical test did not meet the chi-square test conditions. Fisher's exact test was used, and there was no chi-square value.
Laboratory examination
First blood sampling refers to the initial blood collection from children with disease; typically, it is usually conducted ∼1-3 days after onset of the disease. The majority of patients have already been administered drugs by this time, which may potentially compromise the validity of the results.
The chi-square test revealed significant differences in the percentage of neutrophils, percentage of lymphocytes, and lactate dehydrogenase (LDH) levels when comparing children with mild and severe pneumonia (p < 0.05). In contrast, there were no significant differences in platelet (PLT), procalcitonin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), glutamic oxalate aminotransferase (GGT), creatine kinase (CK), or creatine kinase-isoenzyme MB (CK-MB) (p > 0.05) (Table 3).
Laboratory Examination of Severe and Mild Adenovirus Pneumonia
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CK-MB, creatine kinase-isoenzyme MB; CRP, C-reactive protein; GGT, glutamic oxalate aminotransferase; LDH, lactate dehydrogenase; PCT, procalcitonin; PLT, platelets; WBC, white blood cell.
Coinfections
Among the 99 adenovirus pneumonia cases, according to clinical manifestations and lung computed tomography, adenovirus was the main pathogen, and the remainder were mixed infections. Table 4 shows coinfections with other respiratory pathogens in the study population. The most prevalent coinfections were with S. pneumoniae (49.5%), H. influenzae (26.3%), and M. pneumoniae (28.3%). Other respiratory pathogens detected included Parainfluenza virus (11.1%), Influenza A virus (3.0%), Respiratory syncytial virus (6%), M. catarrhalis (7.1%), B. pertussis (9.1%), Rhinovirus (7.1%), Bocavirus (1.0%), Acinetobacter baumannii (6.1%), and Staphylococcus aureus (1.0%).
Coinfections Pathogens in Severe and Mild Adenoviral Pneumonia
“−” means that the statistical test did not meet the square test conditions. Fisher's exact test was used, and there was no square value.
As shown in Table 4, S. pneumoniae was the most prevalent coinfecting organism in cases of adenovirus pneumonia, followed by M. pneumoniae and H. influenzae. However, there were no significant differences in the prevalence of these pathogens in cases of severe and mild adenovirus pneumonia, as well as mixed infection (p > 0.05).
Complications and outcomes
Both mild and severe adenovirus pneumonia patients exhibited fever with mean peak temperatures of 38.6 ± 2.6 and 38.6 ± 1.7, respectively. The duration of fever ranged from 1 to 32 days, with an average duration of 9 days. Compared with mild pneumonia, the time of fever associated with severe pneumonia was significantly longer [(7.15) vs. (2.8) days] (p < 0.05).
Among the 99 children with adenovirus pneumonia, severe cases were significantly more likely to be accompanied by hematological and digestive system diseases compared with mild cases in the later stage (p < 0.05). The outcomes of the children with adenovirus pneumonia were as follows: 3% were cured, 86% showed improvement, 4% unfortunately died, 4% were discharged automatically, and 2% were referred to a superior hospital. In this region, the outcomes of severe cases were relatively poor; however, there was no significant difference in outcome between severe and mild adenovirus pneumonia as indicated in Table 5.
Complications and Prognosis of Severe and Mild Adenovirus Pneumonia
“−” means that the statistical test did not meet the chi-square test conditions. Fisher's exact test was used, and there was no chi-square value.
Analysis of genotype
Infection-type information was available for 81 out of the 99 cases that were examined. Among these cases, the detected prevalence of adenovirus types 1, 2, 3, 4, and 7 was 1 (1.23%), 4 (4.94%), 20 (24.69%), 2 (2.47%), and 54 (67.5%), respectively, as shown in Figures 1 and 2. Genotype 7 was the predominant type in May-July, with most infections occurring in May. Genotype 3 was more commonly detected in the months of January, May to October, and December. Genotype 2 was primarily detected between September and November.

Number and monthly distribution of adenovirus serotypes from January to December 2019. HAdV, human adenovirus.
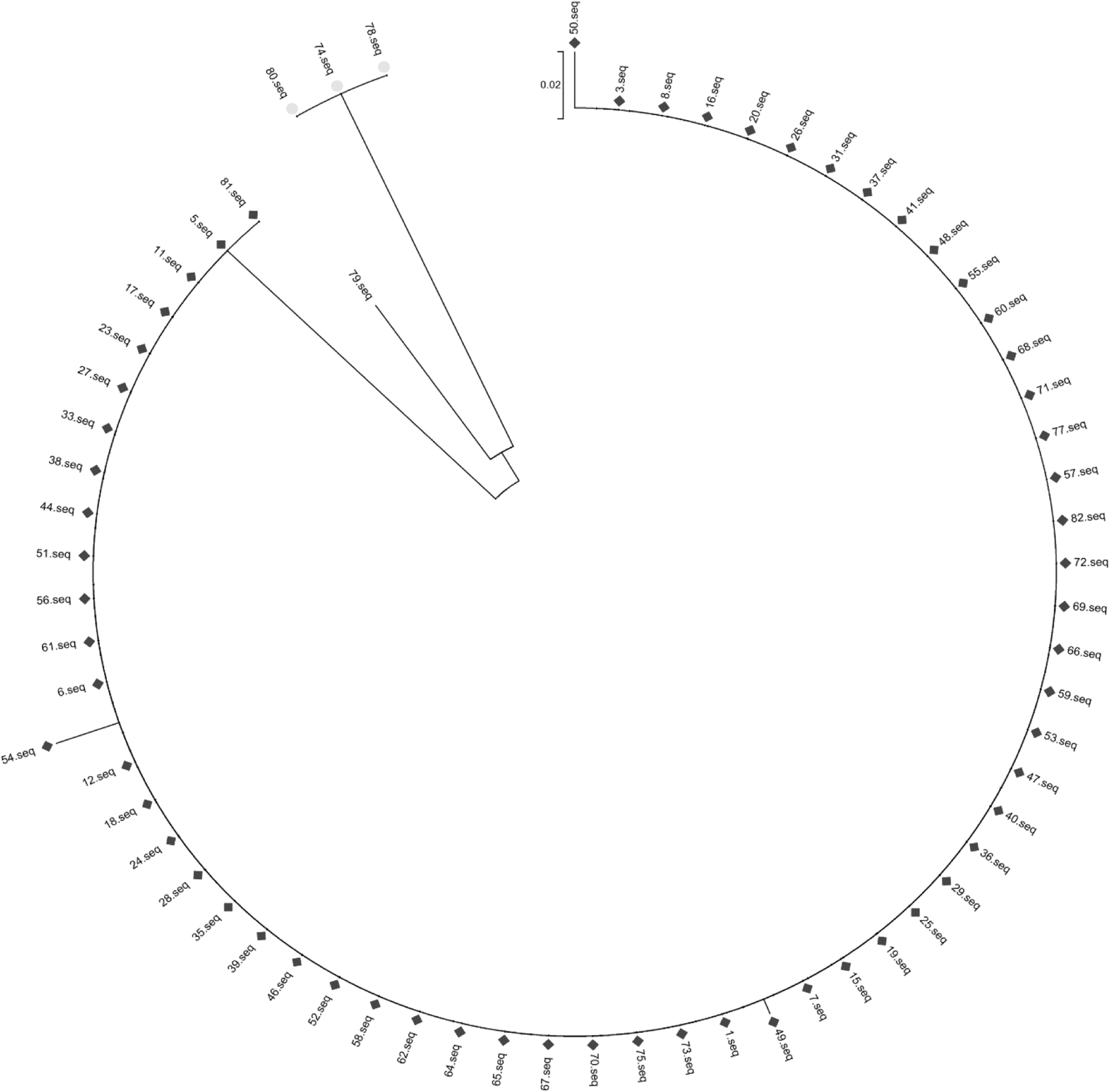
Evolutionary tree of adenovirus serotypes from January to December 2019.
In both severe and mild cases of adenovirus pneumonia, genotype 7 was the most common type, accounting for 72.2% of severe cases and 55.6% of mild cases. In this study, three patients treated with extracorporeal membrane oxygenation (ECMO) were infected with adenovirus 7. Nevertheless, there was no significant difference in the distribution of adenovirus genotypes between severe and mild adenovirus pneumonia, as indicated in Table 6.
Serotyping Results of Severe and Mild Adenovirus
The data distribution did not meet the condition of the square test, and Fisher's exact test was used instead.
Risk factors for severe pneumonia caused by adenovirus infection
Variables with a p-value <0.05 from univariate logistic regression analysis were included in multivariate logistic regression analysis to evaluate the risk factors associated with severe pneumonia. The independent variables were selected by the forward LR. p-Value <0.05 was considered statistically significant.
The results, as shown in Table 7, indicate that a long duration of fever, dyspnea, and digestive system complications were found to be significant risk factors for severe pneumonia after HAdV infection. This suggests that patients with a prolonged fever, experiencing difficulty in breathing (dyspnea), and encountering complications related to the digestive system are more likely to develop severe pneumonia after HAdV infection.
Analysis of Viral Load (Cycle Threshold Value) in Patients With Severe and Mild Pneumonia
Discussion
Infants under 2 years old not only have an immature respiratory tract but also experience unbalanced autoimmune system development, resulting in low nonspecific and specific immune responses. The respiratory and immune systems of older children mature gradually. Moreover, older children have built-up protective antibodies due to previous natural infection.
This may be why the highest rate of HAdV infection is observed in children under 5 years old, especially those aged 0-2 years. Among the 99 patients in our study, the age range spanned from 1 month old to 9 years old; children under 2 years old accounted for 56.6% of cases. The median age was 21 months, which is roughly consistent with previous literature (Binder et al., 2017; Lin et al., 2017).
Serological studies have shown that HAdV-specific IgG antibodies are transmitted from the mother in the first few months after birth, are deficient in infants until 2 years old, and increase gradually after the age of 2 years. Children younger than 6 months benefit from specific immunity due to the protection of their mother's antibodies and are less affected by HAdV (Cheng et al., 2015). However, 15% of the children infected with HAdV in this study were under 6 months, suggesting that the protective effect of maternal antibody for infants aged 0-6 months was limited.
In general, HAdV infection in hospitalized children under 6 months with pneumonia should not be ignored. However, there was no significant correlation between severe and mild HAdV pneumonia cases in terms of age, sex, or complications with primary disease.
The average hospitalization time for adenovirus pneumonia was 14 days, and the average hospitalization cost was ∼¥ 20,000, which was much longer and higher than that for common pneumonia (Harris et al., 2011; Heindl et al., 2019). The longest hospitalization duration was 55 days, with the highest cost reaching¥ 319,187.76. In addition, the proportion of severe adenovirus pneumonia was 67.7%, with all severe adenovirus pneumonia cases treated in the intensive care unit, confirming the severity of adenovirus pneumonia.
The results of routine blood examinations showed that the percentage of neutrophils in the early stage after HAdV infection was significantly increased, which is roughly consistent with the literature and possibly indicates early stage viral infection. The percentage of lymphocytes in severe adenovirus pneumonia was substantially lower, which suggests that mixed bacterial infection may not be ruled out in the early stage. Further laboratory studies are needed to elucidate the specific mechanism.
Due to the shared actions of hypoxia, inflammation, and toxins in lung tissue, local tissue damage occurs, leading to the loss of the cell membrane structure integrity, and the release of enzymes. Significant increase in LDH levels can reflect the degree of lung inflammation and tissue damage to some extent.
When comparing the proportion of increased LDH levels in severe and mild adenovirus pneumonia, it was found that the former was significantly higher than the latter (p < 0.05). Therefore, early evaluation of LDH can be helpful for assessing the severity of the disease in its early stages, which is consistent with current domestic research.
In this study, there was no significant difference in white blood cell (WBC), C-reactive protein, PLT, ALT, AST, GGT, CK, or CK-MB between cases of severe and mild adenovirus pneumonia (p > 0.05). One possible reason for the findings is that early adenovirus infection had not extended to multisystem disease.
Previous reports have confirmed a high incidence of coinfections in children with respiratory tract infections. HAdV has a similar susceptible population and epidemic season as other respiratory pathogens, which may lead to mixed infections. Notably, nonspecific changes in the airway during HAdV infection and the specific reaction between bacteria and the host mediated by the virus are significant factors for coinfection (Li et al., 2021; Rajkumar et al., 2015).
Coinfection of HAdV and M. pneumoniae has been reported as the most common in Beijing, China (Gao et al., 2020). In our study, the most common mixed infection in cases of adenovirus pneumonia was S. pneumoniae (49.5%), followed by M. pneumoniae (28.3%) and H. influenzae (26.3%). In addition to common pathogens in pneumonia such as S. pneumoniae and H. influenzae, it is important to pay attention to coinfection with M. pneumoniae as it occupies the second position in terms of prevalence.
Therefore, we should pay attention to coinfection with this pathogen. Notably, nine cases presented coinfection with B. pertussis, accounting for 9.1% of the cases. Importantly, it was observed that not all of the nine children had been vaccinated with the Diphtheria, Pertussis, and Tetanus (DPT) vaccine; this indirectly indicates that infants who have not been immunized with the DPT vaccine are generally susceptible to B. pertussis. Although the DPT vaccine provides strong protection in infants, it is not 100% effective. Further studies are necessary to gain a deeper understanding of this observation.
China is a vast territory with significant differences in climate, culture, and customs across the different regions. There are also differences in epidemic seasons, genotypes, and outcomes of HAdV infections. In northern China, HAdV infection is common throughout the year and prevalent in winter. However, it is more prevalent during the spring and summer in the southern region, with the highest incidence rate occurring in summer.
Further, in recent years, the major types of HAdV infection in northern China have been found be types 3 and 7. In contrast, those in the southern region had mainly been typed 3 and type 2 (Chen et al., 2016; Duan et al., 2019; Yao et al., 2019). HAdV infection was found to be more common in September and December. Further, the survey indicated that the susceptible population was 1- to 4-year-old children according to a survey from 2001 to 2002 in the Taiwan area, which is close to the Quanzhou area (Chen et al., 2004).
This study demonstrated a seasonal pattern of HAdV infection with the majority of cases (70.7%) occurring in spring and summer, especially during the latter (37.0%), and it was also observed that most infections were reported in May. Further, the analysis revealed the presence of five types of HAdV. Notably, HAdV-7 was detected consistently throughout the year, spanning from January to October 2019. HAdV-3 exhibited a higher prevalence in January, as well as during the months of May to October and December 2019.
The presence of HAdV-2 was noted specifically between September and November 2019. On the other hand, sporadic occurrences of HAdV-1 and HAdV-4 were observed. It is worth mentioning that adenovirus types 3 and 7 are the main types associated with lower respiratory tract infections in children under 5 years of age worldwide (Chehadeh et al., 2018; Selvaraju et al., 2011; Wang et al., 2015).
Antibodies against different species (A-F) of HAdV have been identified in this study, Interestingly, the results revealed that species B exhibited the lowest titer, with only 18% positivity. These findings indicate that the immunity of people to subgroup B is generally low (Nagao et al., 2018). This may be one of the critical reasons for the high infection rates of types 3 and 7 (both subgroup B).
Our study revealed that HAdV pneumonia was mainly caused by species B (accounting for 91.4%), as dominated by types 7 and 3. Adenovirus type 7 accounted for the highest proportion (66.7%), followed by type 3 (24.7%), consistent with relevant literature (Selvaraju et al., 2011). In addition, adenovirus C (types 1, 2) and species E (type 4) infections were found. HAdV involves different clinical manifestations based on genotype, with species B being associated with gastroenteritis, respiratory tract infection, and keratoconjunctivitis (Lee et al., 2012).
Notably, HAdV-b7 is associated with severe respiratory disease (Liu et al., 2015; Scott et al., 2016). Species C and E primarily cause respiratory tract diseases, whereas species D is associated with keratoconjunctivitis. On the other hand, species F is often associated with gastroenteritis (Lion, 2014). Adenovirus types 1, 2, and 4 have been reported sporadically, without outbreaks.
However, our study found no significant difference in genotype between severe and mild adenovirus pneumonia. Possible reasons for this are as follows. First, the sample size of cases included in this study was small; the HAdV cases described in this study do not represent a population-based sample. Second, given that the diversity of genomic types in adenovirus serotypes is a worldwide phenomenon, it is unclear whether genomic type diversity is the primary cause of clinical manifestations. HAdV3a50 and HAdV3a51 are newly described variants that became more prevalent in 2006 and 2007 and have been associated with at least one epidemic (Lebeck et al., 2009).
Most of the genomic types among genotypes are closely related, which suggests that these variants may be caused by genetic drift of epidemic genomic types, and minor changes in genome sequence may be sufficient to exert survival advantages over previous circulating genome types. Therefore, whenever possible, full-genome sequencing should be performed when possible.
Several studies have revealed that HAdV is an important pathogen of viral myocarditis and viral diarrhea (Treacy et al., 2010). Our study, which included 99 cases of HAdV pneumonia, showed a statistically significant association (p < 0.05) between severe and mild adenovirus pneumonia and accompanying hematological and digestive system diseases.
Regarding the outcome, according to the consensus of experts, the results of our study showed that 3% of the children were cured, 86% improved, 4% died, 4% were discharged against medical advice, and 2% were transferred to a superior hospital. According to reports from relevant research, the fatality rate of adenovirus pneumonia can reach 10% (Shieh et al., 2022).
Due to rescue measures such as ECMO, plasma exchange, and blood purification, two children were successfully rescued. However, one child, who was 3 months old, unfortunately died in our hospital. It is worth noting that this child had been transferred to our hospital after receiving 1 month of treatment at another hospital. Initially, the patient was diagnosed with severe pertussis and toxic encephalopathy.
However, as the disease progressed, complications such as liver failure, myocardial damage, serous effusion, and gastrointestinal bleeding occurred. Therefore, we conducted a multidimensional evaluation of the comorbidities of adenovirus pneumonia, including: the complication of the nervous system: toxic encephalopathy encephalitis, convulsions, coma; the complication of kidney diseases: acute nephritis, renal failure; the complication of blood system: dysfunction pancytopenia, anemia, neutrophil, deficiency, thrombocytopenia; the complication of gastrointestinal infection: diarrhea, vomiting, toxic intestinal paralysis, and gastric intestinal failure, gastrointestinal bleeding; the complication of cardiovascular system: myocarditis, myocardial enzyme abnormality; the complication of immune system: immunocompromised.
In addition, the patient developed secondary sepsis involving Staphylococcus hominis subsp. Despite the high number of severe adenovirus pneumonia cases in our hospital, the fatality rate was lower than the national average. Among patients with lower airway infection, the survival rate ranged from 14% to 60%.
In addition, these patients had different degrees of pulmonary complications (Cheng et al., 2015), such as bronchiolitis obliterans, hyaline membrane, and bronchiectasis. The pathological basis of lower airway infection is small airway lesions (Shieh et al., 2022). Adenovirus pneumonia can easily cause the sequelae cited earlier, which needs further study.
The study has several advantages. First, it focused on hospitalized children, whereas most previous studies have primarily focused on screening adenovirus genes in children with respiratory diseases in outpatient clinics. Second, unlike previous studies that mainly analyzed genotypes, this study also explored clinical manifestations, laboratory examinations, and other pathogenic bacteria.
Third, there is limited literature on the disease burden and length of hospital stay in children hospitalized with adenovirus pneumonia, and this study provides a detailed elaboration on this group. Overall, the study was comprehensive, allowing for multidimensional and multilevel analyses of adenovirus pneumonia, which have substantial clinical implications and reference value in vaccine development.
The study mentioned has several limitations. First, the study duration was short, only spanning 1 year. As a result, a comprehensive analysis of changes in adenovirus genotyping in the area could not be performed due to the lack of comparison between years before and after. In addition, the number of cases included in the trial was small, and it should be noted that the HAdV cases described in the study were not representative of a population-based sample.
As this was a clinical study, the specific reasons for the observed problems can only be speculated. Further discussion and verification in animal model experiments and molecular biology studies are required to determine the underlying causes.
In conclusion, conducting surveillance on the types of HAdV-type surveillance is a crucial tool for monitoring the relative prevalence of different genotypes (Wu et al., 2022). In Quanzhou, Genotypes 7 and 3 are commonly associated with pneumonia with type 7 being particularly prevalent. Therefore, when adenovirus infection is identified, it is important to determine the genotype as soon as possible, and closely monitor the disease progression.
Footnotes
Acknowledgments
The authors would like to thank the patients and their parents for participating in this study and the staff at Quanzhou Women and Children's Hospital for their assistance.
Authors' Contributions
J.Z.: Conceptualization, methodology. D.P.: Data curation, writing
Ethics Approval and Consent to Participate
The study was conducted in line with the Declaration of Helsinki (as revised in 2013). This study was approved by the ethics committee of Quanzhou Women and Children's Hospital (No. 2020-33), and informed consent was obtained from all the participants.
Availability of Data and Materials
Data and materials can be obtained by contacting the corresponding author.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was also supported by Shanghai Biogerm Clinical Laboratory and the Technology Project of Quanzhou, Fujian Province (2018E158).