
Abstract
Background:
We aim to investigate the possible causal association between Hashimoto's thyroiditis (HT) and rheumatoid arthritis (RA) using Mendelian randomization (MR) methods.
Methods:
A bidirectional MR analysis was conducted to evaluate the causal association between HT and RA. We obtained summary statistics data from two extensive genome-wide association studies (GWAS) comprising 15,654 cases of HT and 14,361 cases of RA. The primary effect estimate utilized in this study was the inverse-variance weighted (IVW) method. To ensure the reliability and stability of the results, we employed several additional methods for testing, including MR-Egger, weighted median, simple mode, weighted mode, and MR-PRESSO.
Results:
Our study revealed compelling evidence of bidirectional causality between HT and RA. When HT was considered as an exposure factor and RA was considered as an outcome factor, this study revealed a positive correlation between HT and RA (IVW: odds ratio [OR] = 2.4546, 95% confidence interval [CI], 1.1473-5.2512; p = 0.0207). Conversely, when we examined RA as the exposure factor and HT as the outcome factor, we still found a positive correlation between them (IVW: OR = 1.2113, 95% CI, 1.1248-1.3044; p = 3.9478 × 10−7).
Conclusions:
According to our research findings, there exists a bidirectional positive causal relationship between HT and RA among European populations. This implies that individuals with HT have an elevated risk of developing RA, and conversely, individuals with RA have an increased risk of developing HT.
Introduction
Rheumatoid arthritis (RA) is primarily characterized as a chronic systemic autoimmune disease that predominantly affects the joints (Smolen et al., 2016). The incidence rate of RA ranges from 0.5% to 1% (Alamanos et al., 2006; Silman and Pearson, 2002). RA exhibits pathological heterogeneity (Aletaha et al., 2015; Honda and Littman, 2012). Lymph node biopsies obtained during the early stages of RA indicate T cell activation occurring outside the synovium (de Hair et al., 2012). Owing to the significant involvement of autoimmunity in the development of RA, there may be a potential association between this condition and other autoimmunity.
Hashimoto's thyroiditis (HT) is a prevalent autoimmune disorder affecting the thyroid. It is characterized by progressive thyroid failure, goiter formation, and infiltration of T cells (Caturegli et al., 2014). Nevertheless, an increasing body of evidence indicates that thyroid autoimmunity may occur as a component of a broader autoimmune process in a substantial number of patients, often overlapping with other autoimmune diseases including RA (Biró et al., 2006; Boelaert et al., 2010; Lazúrová et al., 2014; Weetman, 2011).
The initial investigations on the relationship between RA and HT can be traced back to the 1960s (Buchanan et al., 1961; Gibberd, 1965; Hart, 1970). However, these early studies were primarily cross-sectional or observational and often lacked a suitable control group for comparison. As the research on the association between HT and RA continues to expand, several studies have emerged indicating a lack of a substantial correlation between the two diseases (Linos et al., 1980; Mulhem et al., 1966).
Recent studies exploring the relationship between HT and RA have demonstrated notable variations, likely attributed to factors such as racial disparities and environmental differences (El-Sherif et al., 2004; Li et al., 2019). To summarize, although an association between HT and RA has been acknowledged, it remains uncertain whether a causal relationship exists between the two and whether this association is unidirectional or bidirectional. Investigating the causal relationship between HT and RA can provide valuable insights into the potential etiology of both conditions and offer clinically relevant perspectives for screening, prevention, and patient management of HT and RA.
Mendelian randomization (MR) studies employ genetic variations, specifically single nucleotide polymorphisms (SNPs), as instrumental variables (IVs) to estimate the causal impacts of exposures on outcomes. By doing so, MR studies help overcome confounding factors typically found in observational studies and provide a level of evidence that is second only to randomized controlled trials (Davey Smith and Hemani, 2014; Gupta et al., 2017). In this study, we aim to examine the bidirectional causal relationship between HT and RA using the methodology of MR.
Materials and Methods
Data sources and selection of IVs
A genome-wide association studies (GWAS) conducted by Okada, which involved 14,361 RA cases and 43,923 controls of European ancestry (Okada et al., 2014), provided genetic association estimates of SNPs that were genome-wide significant (p < 5 × 10-8). Similarly, the summary-level data for SNPs linked to HT were acquired from a publicly available GWAS database that drew upon 395,640 individuals with European ancestry (15,654 cases and 379,986 controls) (Sakaue et al., 2021). The characteristics of the cohorts and subjects enrolled in the study are attached in Supplementary Table S3.
To ensure the independence among genetic variants, all SNPs were subjected to clumping using a 5000-kB window and a threshold of r2 < 0.001. In addition, to ensure a strong correlation between SNPs as IVs and exposure, SNPs with F values <10 were excluded (Pierce et al., 2011).
The research utilized SNPs as the independent IVs and adhered to three criteria for conducting MR analysis. First, SNPs with a strong association with the exposure variable were carefully selected, while weak IVs were eliminated using the F-statistic. Second, the selected SNPs were required to be independent of any confounding factors, which was confirmed through the pleiotropy test. Lastly, the impact of SNPs on the outcome variable had to be attributed solely to the exposure variable and not through any direct associations. This condition was evaluated using various MR methods.
Statistical analysis
The primary MR analysis method employed in this study was the inverse variance weighted (IVW) method, which is widely acknowledged as the classical statistical MR approach (Bowden et al., 2017). This method assumes the absence of horizontal pleiotropic effects of the genetic instruments on the outcome variable. To avoid potential pleiotropic effects, four additional MR methods (MR-Egger, weight median [WM], simple mode, and weighted mode) were employed as supplements to assess the bidirectional causal effects between HT and RA.
IVW simulates the randomization procedure for grouping individuals by employing SNPs that induce mutations in gene expression or function. This randomization process aids in mitigating collinearity issues between genetic variations and other potential confounding factors, thereby enhancing the strength of causal inference. Owing to its higher statistical power, the results of the IVW method are typically used as the benchmark to evaluate the causal effect between HT and RA (Burgess et al., 2021). Other MR methods can provide supplementation when heterogeneity or pleiotropy exists.
To obtain stable and reliable results, we conducted the Cochran's Q test to evaluate heterogeneity (Burgess et al., 2018), and used MR-Egger and MR-PRESSO methods to assess horizontal pleiotropy and overall pleiotropy, respectively (Burgess and Thompson, 2017; Verbanck et al., 2018). We also conducted a leave-one-out analysis to determine whether the causality was influenced or biased by any SNP.
In this MR study, all analyses were conducted by the packages two-sample MR (version 0.5.7) in R (version 4.3.1). The presence of significant differences was determined by a p-value <0.05, which we considered as statistically significant.
Ethical considerations
This study employed publicly available deidentified data from participant studies that had previously obtained approval from an ethics committee, eliminating the requirement for additional ethical authorization or participant consent for this research.
Results
Genetic instruments
When HT was regarded as the exposure factor and RA as the outcome factor, the number of IVs was 9, and the F statistics was 82. When RA was the exposure factor and HT was the outcome factor, the number of IVs was 42, and the F statistics was 104. Detailed information about the SNPs are given in Supplementary Tables S1 and S2.
MR analyses
The MR results are summarized in Figures 1 and 2 and Tables 1 and 2. When considering HT as exposure factor, we observed a positive association between the likelihood of developing HT and the RA (IVW: odds ratio [OR] = 2.4546, 95% confidence interval [CI] 1.1473-5.2512, p = 0.0207; MR-Egger: OR = 17.0362, 95% CI 3.1357-92.5557, p = 0.0134; WM: OR = 1.4358, 95% CI 1.2393-1.6633, p = 1.4446 × 10-6; simple mode: OR = 1.6029, 95% CI 1.2144-2.1157, p = 0.0104; weighted mode: OR = 1.2626, 95% CI 1.1899-1.5645, p = 0.0021).
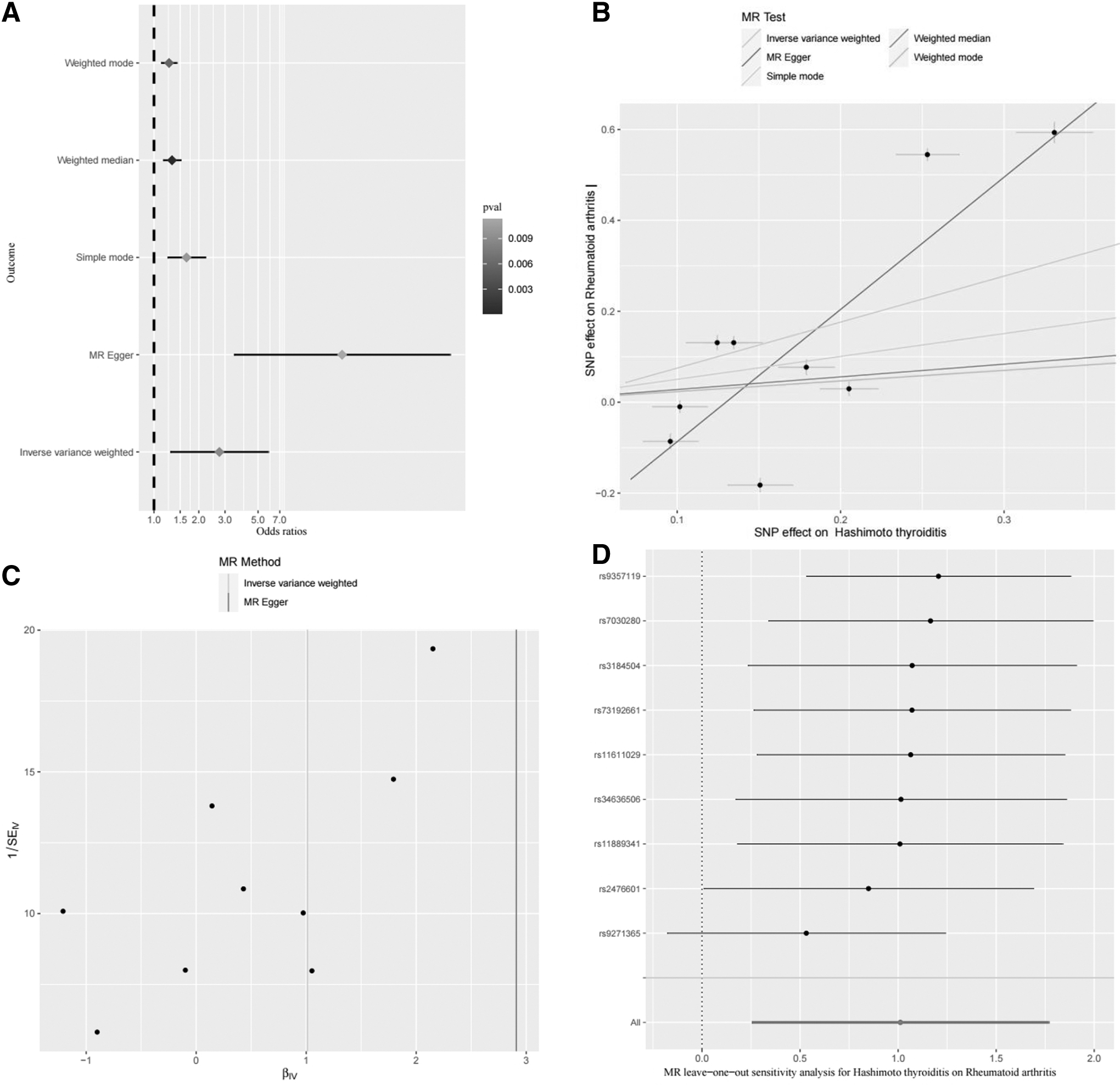
The causal effect of HT on RA.
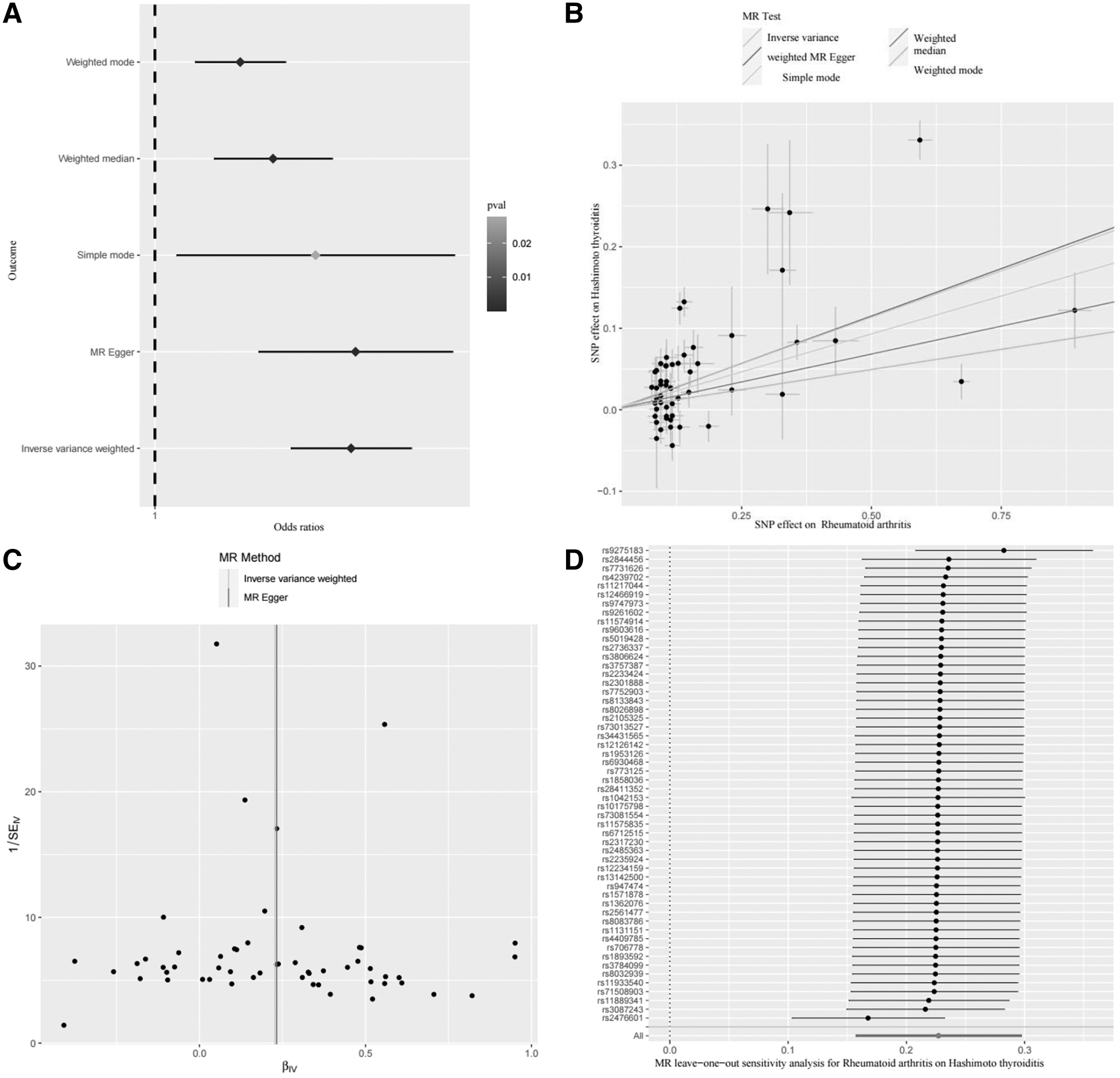
The causal effect of RA on HT.
Causal Effect of Hashimoto Thyroiditis on Rheumatoid Arthritis
IVW, inverse-variance weighted; MR, Mendelian randomization; LCI, lower confidence interval; UCI, upper confidence interval; OR, odds ratio; RA, rheumatoid arthritis; WM, weight median.
Causal Effect of Rheumatoid Arthritis on Hashimoto's Thyroiditis
When RA was considered as exposure factor, there is still a positive correlation between them (IVW: OR = 1.2113, 95% CI 1.1248-1.3044, p = 3.9478 × 10-7; MR-Egger: OR = 1.1910, 95% CI 1.0595-1.3387, p = 0.0056; WM: OR = 1.0883, 95% CI 1.0316-1.1481, p = 0.0020; weighted mode: OR = 1.0721, 95% CI 1.0206-1.1261, p = 0.0083). According to the results of five MR analysis methods, Figures 1A and 2A show evidence of a bidirectional causal relationship between HT and RA.
Sensitivity analyses
According to the sensitivity analyses of the MR analysis results of the causal effect of HT on RA (Fig. 1B, C and Tables 3 and 4), we observed heterogeneity and pleiotropy (Cochran's Q test: p-value = 2.4779 × 10-233; MR-Egger estimates: p-value = 0.0474, MR-PRESSO: global test: p-value <0.001). The leave-one-out analysis indicated that there were no SNPs that could potentially drive the causal link (Fig. 1D). However, the existence of heterogeneity and pleiotropy does not impact our conclusion that HT has a positive causal effect on RA.
Heterogeneity Test of the Mendelian Randomization Results on the Causal Relationship Between Hashimoto Thyroiditis and Rheumatoid Arthritis
Pleiotropy Test of the Mendelian randomization Results on the Causal Relationship Between Hashimoto's Thyroiditis and Rheumatoid Arthritis
SE, standard error.
In our study, we applied IVW analysis under a multiplicative random effects model and obtained consistent results (Table 3, multiplicative random effects model: OR: 1.8634, 95% CI 1.0999-3.1568, p-value = 0.0207). Furthermore, we utilized the “MR-PRESSO outlier test” to identify and remove any abnormal SNPs (outliers) to obtain correct results that account for horizontal pleiotropy (Table 4). Upon removing the outliers, the MR results exhibited increased significance (MR-PRESSO outlier-corrected: p-value = 0.0066).
According to the sensitivity analyses of the MR analysis results of the causal effect of RA on HT (Fig. 2B, C and Tables 5 and 6), heterogeneity and horizontal pleiotropy were detected in our study (Cochran's Q test: p-value = 1.0069 × 10-35; MR-PRESSO global test; p-value <0.001). The leave-one-out test demonstrated that removing any SNP would not fundamentally alter the results (Fig. 2D). To address the presence of heterogeneity and horizontal pleiotropy, we performed IVW under a multiplicative random effects model (Table 5) and utilized the “MR-PRESSO outlier test” analysis to account for and balance these factors.
Pleiotropy Test of the Mendelian Randomization Results on the Causal Relationship Between Rheumatoid Arthritis and Hashimoto's Thyroiditis
Heterogeneity Test of the Mendelian Randomization Results on the Causal Relationship Between Rheumatoid Arthritis and Hashimoto's Thyroiditis
The analysis results provide support for the presence of a positive causal effect of RA on HT (multiplicative random effects [IVW]: OR: 1.1421, 95% CI 1.0849-1.2022; p-value = 3.9478 × 10-10−7; MR-PRESSO outlier corrected: p-value = 3.3985 × 10-6).
Discussion
To our knowledge, this study appears to be the first to investigate the causal relationship between HT and RA using a bidirectional MR approach. The findings of this study offer some evidence supporting a bidirectional positive causal relationship between HT and RA.
HT and RA are two prevalent autoimmune disorders, and immune factors play a vital role in their etiology and progression, suggesting a potential association between them (Jabrocka-Hybel et al., 2018; Yamada et al., 2014). Genetic findings suggest that HT and RA exhibit shared genetic susceptibility factors, including HLA and CTLA4 (AlFadhli and Nizam, 2014; Mikosch et al., 2021; Prahalad et al., 2009). In Karim Benhatchi's research, the frequency of the GG genotype for the CTLA4 A49G gene polymorphism was found to be significantly higher in patients with concurrent HT and RA (Benhatchi et al., 2011). However, literature results suggest that the role of CTLA1 exon 49 A4G polymorphism in RA susceptibility differs between two distinct racial populations (Han et al., 2005).
Moreover, sex steroids may play a crucial role in the development of both HT and RA. Epidemiological investigations reveal a higher incidence rate of HT and RA in women than in men (Kvien et al., 2006; Paknys et al., 2009). As a result of the actions of estrogen and progesterone, both HT and RA tend to ameliorate during pregnancy, whereas postpartum disease activity is more prevalent (Amino et al., 1999; Nelson and Ostensen, 1997). In addition, other environmental factors, including smoking and vitamin D levels, have a certain impact on the occurrence and progression of both RA and HT (Adams and Hewison, 2008; Silman et al., 1996; Wiersinga, 2013).
Although multiple pieces of evidence point to a correlation between HT and RA, the precise direct causal relationship between them has remained unclear until now. However, the findings of this study suggest that in addition to genetic factors, steroid factors, and environmental factors, HT and RA do indeed have a direct causal association with each other. This finding may have implications for the clinical management of HT and RA as it suggests that there could be shared therapeutic targets between the two diseases. Such shared targets may offer potential avenues for drug development and treatment strategies.
Nevertheless, it is crucial to acknowledge a few limitations. First, it should be noted that the GWAS data utilized in our study solely consisted of individuals of European ethnicities, which limits the generalizability of the MR outcomes to other ethnic populations. Second, we regretfully lack subgroup data to examine the causal effects between HT and RA in relation to gender or age groups.
Conclusion
In summary, our research indicates a bidirectional causal relationship between HT and RA, which can provide some assistance for clinical disease management. HT patients should undergo RA screening, and vice versa. For individuals with HT, it is crucial to undergo RA screening. Effective management of HT can help reduce the risk of developing RA, and vice versa.
Footnotes
Acknowledgments
We sincerely thank S. Sakaue and Y. Okada for sharing the GWAS summary data.
Authors' Contributions
J.L. contributed to conceptualization, methodology, and writing—original draft. Y.C. was involved in data curation and conceptualization. Z.J. carried out data collection and data curation. L.L. took charge of data collection and formal analysis. G.Z. took charge of methodology and visualization. K.N. carried out data collection and writing—review and editing. X.D. took charge of writing—review and editing and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.