
Abstract
Abstract
Introduction
When clinicians encounter patients with this kind of granulomatous reaction, they are faced with a diagnostic dilemma, namely, to determine the cause of the granuloma.
Diagnostic challenges arise when simultaneous noninflammatory diseases are present in the patient.
In the present article, the authors report a case of unusual association of inflammatory and neoplastic diseases of the female genital organs, with emphasis on the identification of the origin of the necrotizing granulomatous lesion.
Case
In January 2007, a 49-year-old woman was admitted to the surgery division of our hospital for a laparoscopic colecystectomy for cholelithiasis.
The histological diagnosis was invasive mucinous adenocarcinoma (pT3 N1) and the patient underwent hepatic segment resection and regional lymph nodes dissection (Fig. 1).
Adenocarcinoma of the gallbladder invading the muscle layer (hematoxylin and eosin, ×50).
In June 2008, the patient was admitted for laparocele, and during surgery a right ovarian mass was incidentally found and removed (Fig. 2).

Ovarian metastasis of mucinous adenocarcinoma of the gallbladder (hematoxylin and eosin, ×100).
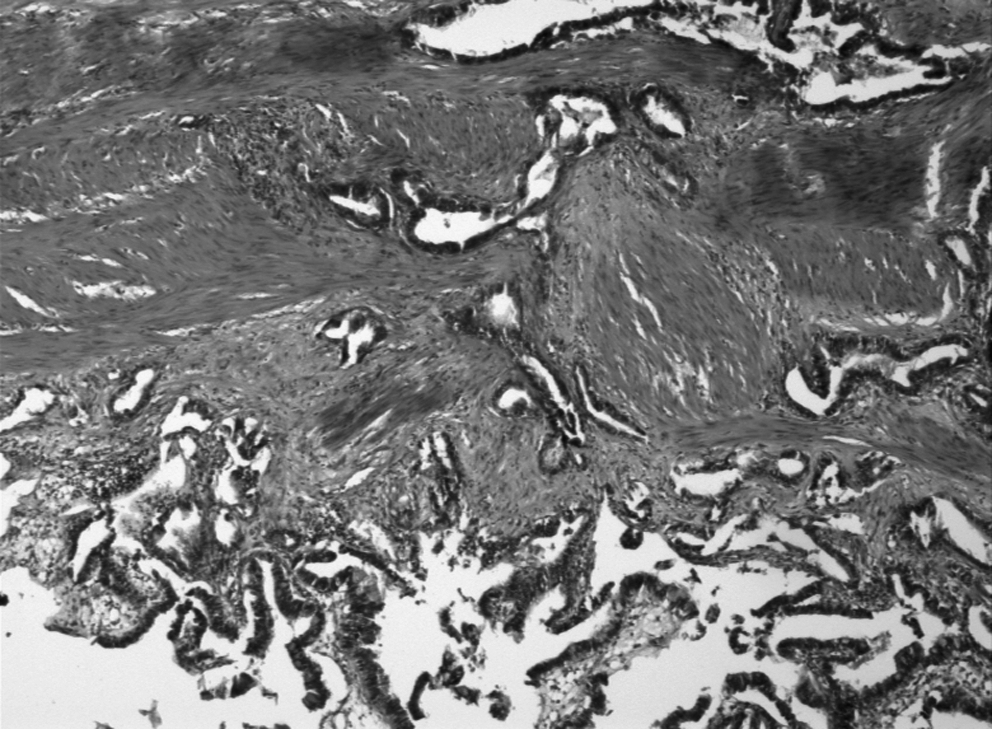
In September 2008, the patient underwent total hysterectomy with left annessiectomy and regional lymph nodes dissection. The histological slides of the surgical specimen were sent in consultation to Professor Christopher D.M. Fletcher, and after his revision the following diagnosis was made: mucinous adenocarcinoma of the gallbladder with bilateral ovarian metastases, associated with borderline serous tumor of left paratubal cyst (Fig. 3) and necrotizing granulomatous inflammation of unknown origin adjacent to the right tube (Fig. 4).

Borderline serous tumor of left paratubal cyst composed by floating papillary aggregates with cellular stratification (hematoxylin and eosin, ×200).
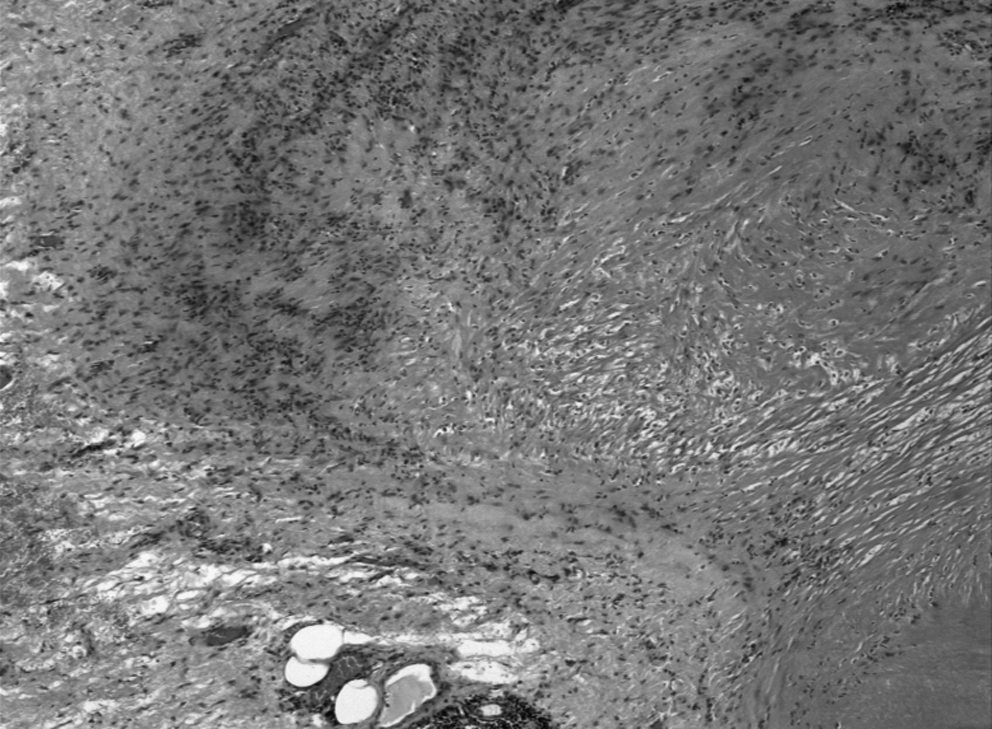
Palisading necrotizing granuloma in the paratubal soft tissue (hematoxylin and eosin, ×200).
The necrotizing granulomatous inflammation prompted a search for foreign bodies, rheumatoid diathesis, and fungal or mycobacterial infection. None of these was found. Follow-up revealed no evidence of a systemic granulomatous or neoplastic disease.
Discussion
Granulomatous lesions of female genital organs may be non-necrotizing or necrotizing. Non-necrotizing granulomatous inflammation of the uterus is a relatively uncommon finding that previously has been attributed to a variety of conditions, including infections, sarcoidosis, foreign-body reactions, and surgical procedures.1–4
Kelly and McCluggage described 8 cases where granulomas not associated with previous procedures were identified as an incidental finding in the myometrium or in the cervical stroma. 5 Because a review of the clinical records did not reveal obvious causes for the granulomatous inflammation, the authors proposed the term “idiopathic uterine granulomas” and speculated that these granulomas and idiopathic ovarian cortical granulomas may have a similar pathogenesis. 6 Kelly and McCluggage wrote that these granulomas are of no significance and merely represent a pathological curiosity.
Necrotizing granulomas of the uterine corpus have been reported associated with biopsy, surgery, and transcervical laser ablation of the endometrium.7–9 Necrotizing granulomas of unknown origin of female organs have not been reported up to now.
In the present case, the lesion consisted of areas of coagulative necrosis with a prominent border of palisaded histiocytes and it was localized in an unusual site as the right paratubal soft tissue.
Non-necrotizing or necrotizing granulomatous lesions of female genital organs have been reported to be associated with neoplastic lesions of uterus. In the study of idiopathic uterine granulomas by Kelly and McCluggage, endometrioid adenocarcinoma of the uterus was found in 2 cases, leiomyomata in 4 cases, and adenomyosis and an endometrial polyp in a single case each. In the report of 11 cases of granulomatous non-necrotizing inflammation of the uterus by Hoff and Prayson, endometrial adenocarcinoma was found in 2 cases, atypical polypoid adenomyoma in 1 case, and leiomyomata in 2 cases. 4
To our knowledge, a case of granulomatous lesions of female genital organs associated with a broad ligament cystadenoma of borderline malignancy has never been described. The paratubal cysts are commonly seen as small round cysts attached by a pedicle to the fimbriated end of the tube. 10 These lesions are of müllerian, mesonephric, and mesothelial origin and are classified as tumor-like lesions of the broad ligament (adenexal lesions). They are usually of müllerian origin, thin-walled, with clear content lined by a single layer of tubal-type ciliated epithelium. 10
Some authors believe that these cysts arise from an invagination or herniation of fallopian tube epithelium, creating an accessory tube lined by epithelium that can develop into a cyst or cystic neoplasm. 11 Other investigators suggest an origin from a müllerian duct remnant or a focus of endosalpingiosis.12–18
In the autoptic study of 468 adnexa from 234 women, Dørum et al. found paraovarian cysts in 11 women (4.7%). All cysts were benign, except for 1 case with bilateral serous cystadenoma of borderline type. 19 The risk of malignancies in this kind of cyst is <1%.20,21
Regarding the borderline tumors of the broad ligament, more than 30 cases, mostly serous cystic tumors, have been reported. One mucinous tumor has been reported.13,22–28
The present case is a rare example of borderline serous tumor arising from the müllerian cyst wall of the broad ligament. In the diagnosis of this lesion, all the criteria for primary tumors of the broad ligament proposed by Gardner et al. were considered: a primary location within, or on the surface of the broad ligament and a complete separation of the tumor from both the uterus and the ipsilateral ovary. 12
Regarding the second neoplasm of the patient, we reviewed the literature about mucinous carcinoma of the gallbladder. It represents 4% of all gallbladder malignancies 29 and more than 50% of the tumor must contain extracellular mucin to be defined as mucinous. 30
Six percent (6%) of the patients had ovarian metastasis, most of which with peritoneal involvement. 29 Clinically and pathologically, ovarian metastasis of gallbladder mucinous carcinoma may simulate a simultaneous primary mucinous cystoadenocarcinoma of the ovary. No immunostain would reliably make this distinction, as CDX-2 can be positive also in this kind of ovarian neoplasm. In the present case, the diagnosis of ovarian metastasis was supported by a negative finding of the ovaries in the computed tomography scan performed prior to colecystectomy.
Conclusions
In conclusion, the possibility of a systemic granulomatous or vasculitic disease should be stated in the pathology report and excluded clinically, even if this lesion could be originated from a previous surgical procedure or from a reaction to a neoplastic disease. To our knowledge, the association of these diseases is a unique case in the literature.
Footnotes
Acknowledgments
We would like to thank Prof. C.D.M. Fletcher and collaborators of the Department of Pathology of Brigham and Women's Hospital in Boston who revised our slides and gave us their valuable opinions about the case.
Disclosure Statement
No competing financial interests exist.