
Abstract
Abstract
Introduction
The definition of endometrial ablation or resection procedures has evolved over time and is now divided into two categories: (1) Resectoscopic (hysteroscopic) ablation procedures, which have also been called first-generation procedures. These are the original procedures that require an operative hysteroscope or resectoscope to perform. A laser fiber, loop, or rollerball electrode is used with the scope to ablate or resect the endometrium. (2) Nonresectoscopic (nonhysteroscopic) ablation procedures are the newer techniques that do not require an operative hysteroscope or resectoscope to perform. These are designed to be technically easier and are referred to as global endometrial ablations (GEAs) or second-generation endometrial ablations. There are five nonresectoscopic or nonhysteroscopic ablations (GEAs) approved by the United States Food and Drug Administration (FDA). These include thermal balloon endometrial ablation (ThermaChoice, Ethicon Inc., Menlo Park, CA), hydrothermal endometrial ablation (HydroThermAblator, Boston Scientific, Natick, MA), radiofrequency endometrial ablation (NovaSure, Cytyc Surgical Products, Palo Alto, CA), cryoablation (Her Option, CryoGen Inc., San Diego, CA), and microwave endometrial ablation (Microsulis, Hampshire, England).
Although this article's main focus is on the newer GEAs, the review must include the resectoscopic procedures because the delayed complications were originally discovered following these older techniques.
Review
The etiology of all delayed or long-term complications following both resectoscopic and nonresectoscopic endometrial ablations is due to the intrauterine scarring and contracture that can occur following the procedure. The reason this scarring occurs is that the intent of a resection or ablation is to totally remove or destroy all the endometrium, which exposes intrauterine myometrium. After the distention media or ablation device is removed, these myometrial walls collapse upon each other, are in juxtaposition, and have a natural tendency to grow together, causing intrauterine scarring and contracture. The intrauterine scarring itself does not have clinical significance unless obstructed bleeding occurs from persistent or regenerating endometrium trapped behind the scar.
This intrauterine scarring and contracture has been well documented by multiple authors following the older resectoscopic ablations, 1 but a similar problem is being observed after GEAs. Roy et al. 2 found that any heat-based nonresectoscopic ablation procedure (GEAs) that causes thermal destruction of the endometrial lining produces significant scarring of the endometrial cavity. He found that when raw surfaces of the myometrium oppose each other and heal, the architecture of the endometrial cavity is altered and may even obliterate the cavity.
The first GEA approved by the FDA was the balloon ablation. Leung et al. 3 did diagnostic hysteroscopy 6 months following this procedure in 22 patients. Postablation intrauterine adhesions were found in 8 women (36.4%); 6 had focal adhesions in the fundal area and 2 had complete obliteration of the cavity.
Intrauterine scarring was also demonstrated on a hysterosalpingogram (HSG) study done 3 months following a third-generation balloon endometrial ablation and concomitant microinsert tubal sterilization. 4 This was a postapproval study required by the FDA to assure successful tubal closure. Of the 30 patients studied, 10 (33%) had intrauterine synechia. Five (5) had such significant scarring that the HSG was unable to confirm tubal occlusion, so the study was discontinued.
Hopkins et al. 5 studied 25 patients with menorrhagia who requested permanent sterilization at the time of their GEA. A radiofrequency global endometrial ablation was followed by hysteroscopic sterilization. Of the 21 patients who had a 3-month follow-up HSG, 9 patients (43%) had normal-appearing cavities, 5 (24%) had mild synechia, and 7 (33%) demonstrated intrauterine contracture. Tubal patency was noted in 2 patients, and a 6-month follow-up HSG revealed increasing synechiae. The one HSG done at 9 months revealed severe synechia. This is the first study to demonstrate that post GEA intrauterine scarring increases over time. This information is important to understand because it helps explain that many of the delayed complications after GEA take time to develop.
Cryoablation was developed in an attempt to prevent intrauterine scarring. Townsend et al. 6 performed hysteroscopy at 9, 12, or 15 months postcryoablation on 95 patients and found no intrauterine synechiae or adhesions. However, in 15 cases, the intrauterine cavity appeared narrowed and shortened, indicative of contracture. In 30 cases, only one tubal ostium could be visualized, which means that scarring is affecting the other cornu, suggesting that cryoablation is having similar intrauterine effects as heat-based GEAs.
Quinlan 7 assessed the endometrial cavity by hysteroscopy 6 months after cryoablation in 10 patients. In 4 cases, there were synechiae or marked narrowing limiting visualization of the entire cavity. Further studies will be necessary to clarify whether cryoablation is truly superior to heat ablation in decreasing intrauterine contracture and scarring.
Intrauterine scarring and contracture does not appear to cause symptoms unless obstructed bleeding occurs from persistent or regenerating endometrium behind the scar.
What percent of patients have endometrium remaining after an ablation? The most comprehensive study to focus on this issue was by Turnbull et al. 8 who performed magnetic resonance imaging (MRI) on 59 patients 5–65 months after endometrial resection including rollerball ablation of the cornual areas. Endometrial tissue was detected in 56 patients (95%) and was most commonly found in the upper uterine fundus close to the tubal ostia. Eleven (11) patients (18%) had hematometra situated in a uterine cornu. Two had marked dilatation of a fallopian tube and free intraperitoneal fluid was present in 32 patients (54%). The MRI indicated that this fluid was mainly blood, suggesting retrograde menstruation, and the radiologist indicated that the finding was unexpected.
Persistent or regenerating endometrium is also found after GEAs. Olson et al. 9 studied 15 patients with MRI 4 months after microwave endometrial ablation. A significant amount of endometrial tissue was found in 11 patients (73%). Taskin et al. 10 did random endometrial biopsies on 26 patients approximately 2.5 years after thermal balloon ablation and found endometrial glands in most specimens. They state that endometrial regrowth is an expected development following balloon ablation and should not be considered a failure.
Endometrium is also present in the intramural oviduct that is not destroyed by any of the ablation procedures. Lisa et al. 11 serially sectioned the intramural oviduct in 300 uteri and found that 25% of cases had endometrium in this portion of the tube.
Endometrial cells can persist after an endometrial ablation if deep adenomyosis is present. We 12 found that that approximately 20% of patients with menorrhagia have deep adenomyosis, which is a major cause of persistent bleeding problems following an ablation.
If there is bleeding from postablation endometrial tissue obstructed behind intrauterine scarring, central hematometra, CH, PATSS, and/or retrograde bleeding can occur.
Central Hematometra
Central hematometra (Fig. 1) results from residual or regenerating endometrium bleeding behind a cervical or lower uterine segment stenosis. This stenosis is caused from damage to the upper endocervical canal and/or lower uterine segment at the time of an endometrial ablation and/or resection. It has occurred after both resectoscopic and nonresectoscopic ablations in 1%–3% of cases. 1
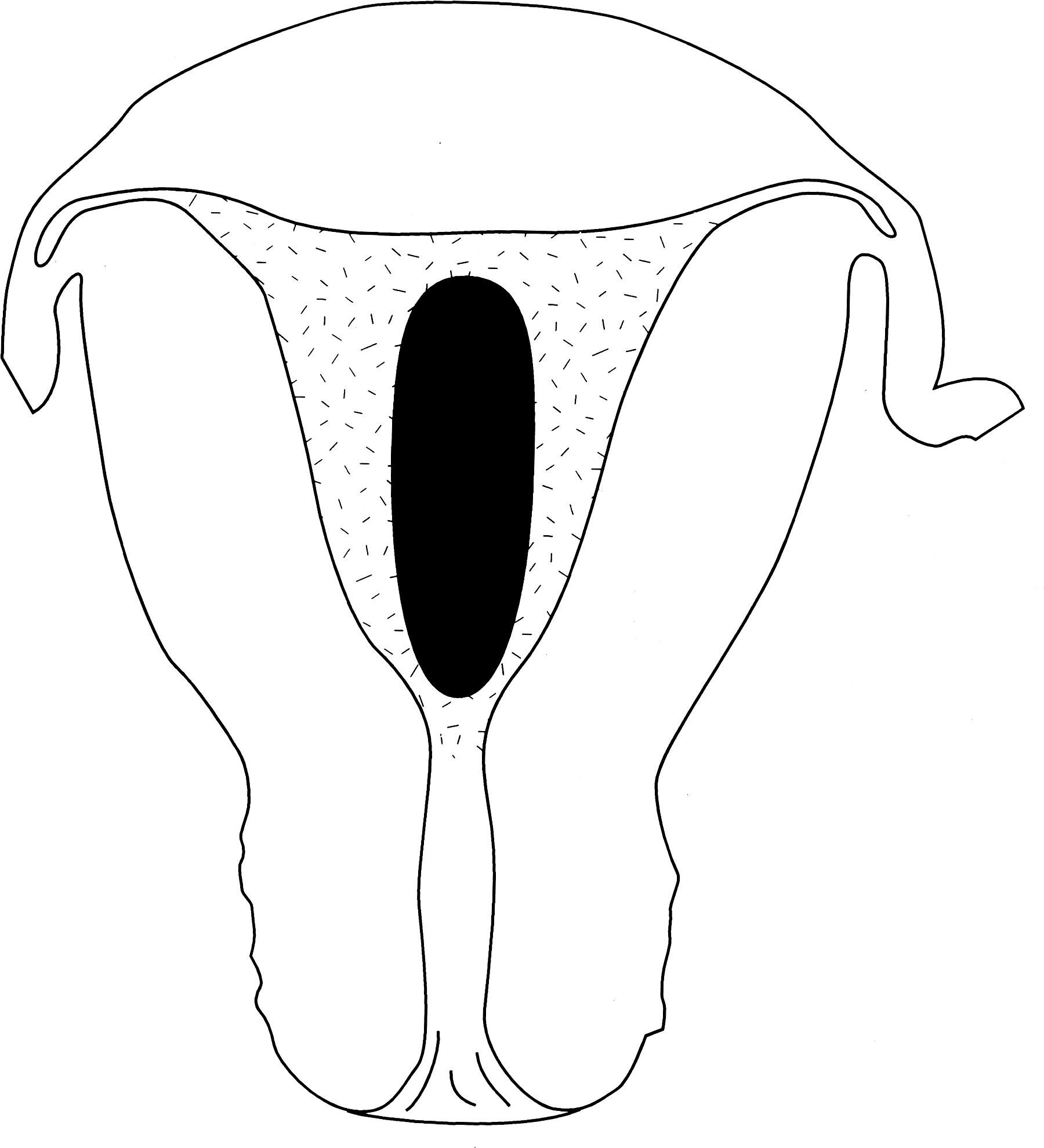
Drawing shows postablation intrauterine contracture (stippled area) with a central hematometra (black area).
The key symptom of central hematometra is cyclic lower abdominal/pelvic pain during the menstrual phase of the cycle. Patients are usually amenorrheic and the pain typically begins weeks to months after the surgery. An ultrasound study when the patient has symptoms is usually diagnostic.
Central hematometra can usually be treated by simply performing a cervical dilatation under ultrasound guidance. The placement of a stent is sometimes necessary.
Cornual Hematometra (CH)
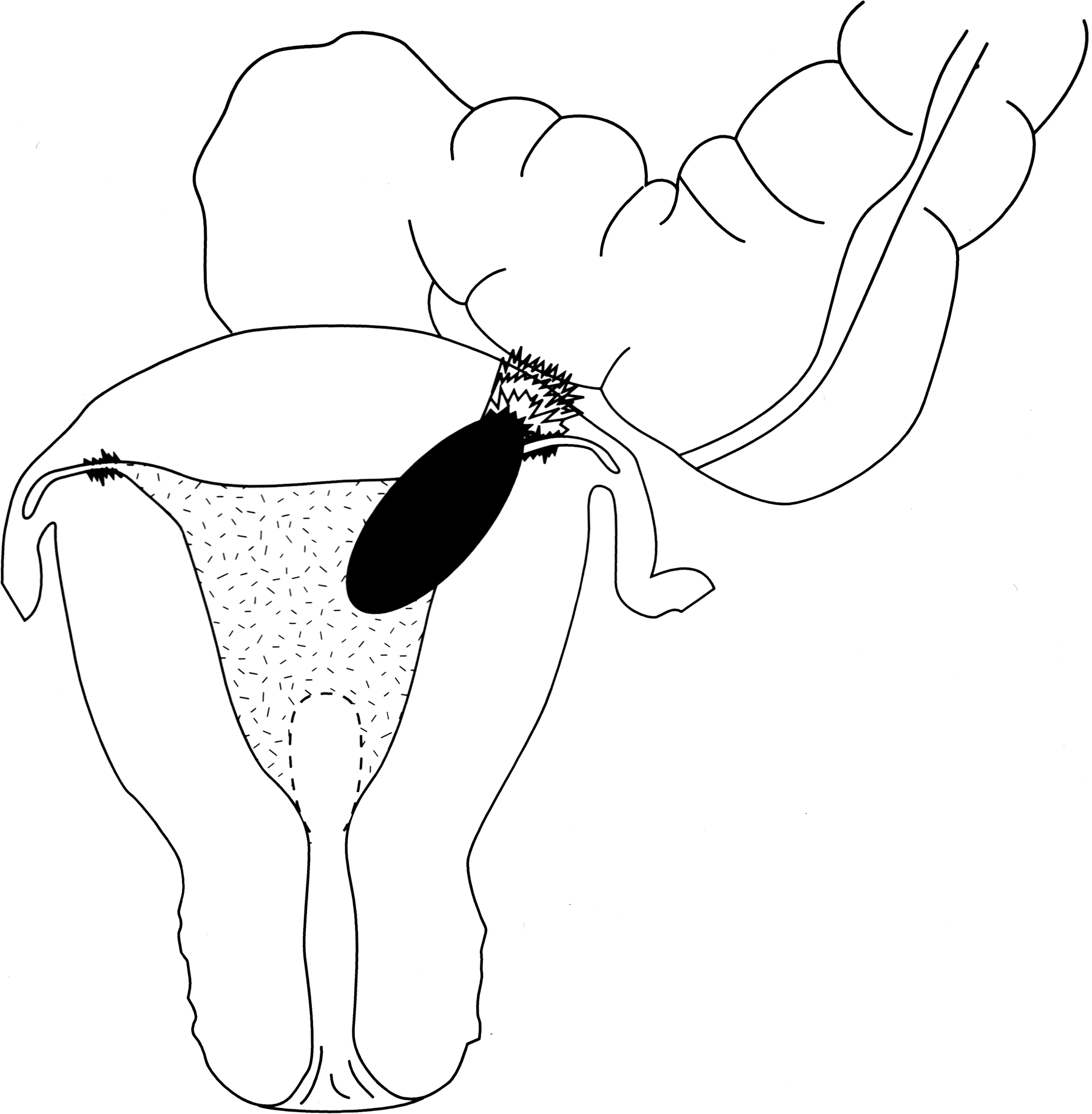
Cornual hematometra (Fig. 2) occurs when persistent or regenerating endometrium bleeds in the cornual area when there is both a proximal and distal cornual obstruction. The distal scarring prevents decompression of the hematometra by blocking retrograde bleeding through the oviduct.
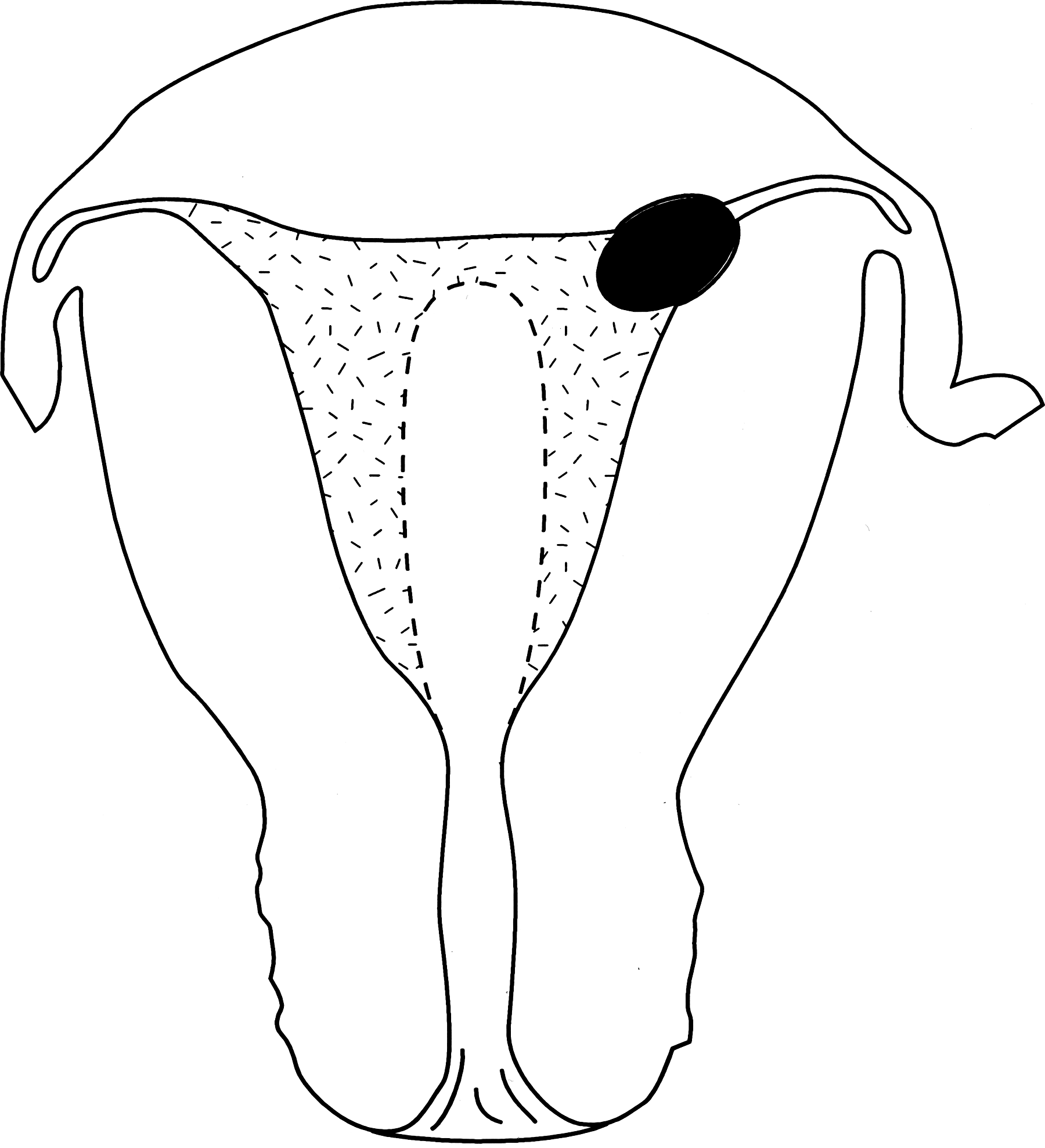
Drawing shows postablation intrauterine contracture (stippled area) with a left cornual hematometra (black area). (Used with permission from Elsevier.)
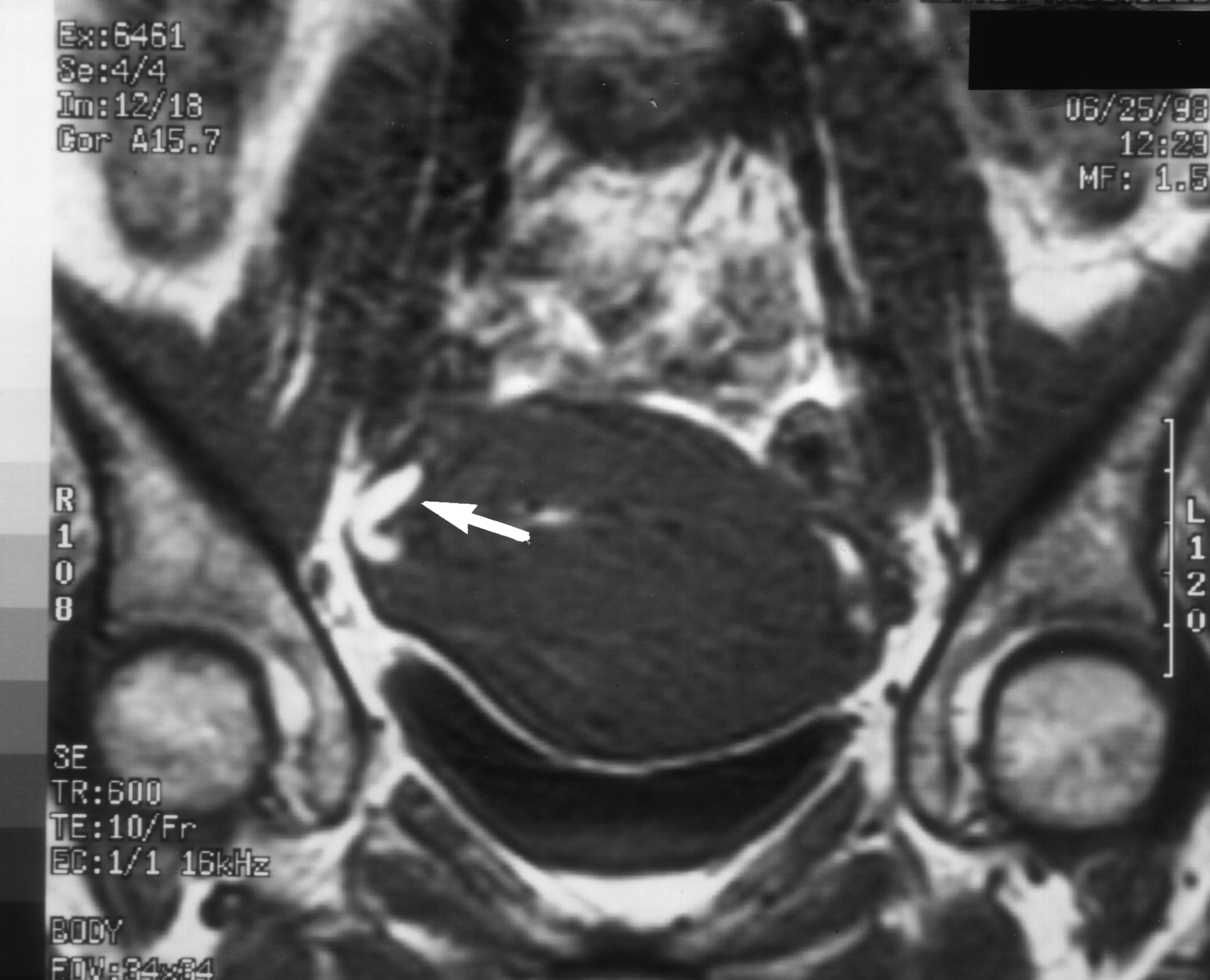
The symptoms of CH are usually cyclic lower abdominal pain during the menstrual phase of the cycle. Often, the pain is unilateral on the same side as the CH. The diagnosis can only be made if the imaging study is performed while the patient is symptomatic. The cornual hematometra can absorb during the remainder of the month and the diagnosis can be missed during this time. If the CH is large, it may be visualized on ultrasound but often it is small, requiring an MRI study to make the diagnosis (Fig. 3).
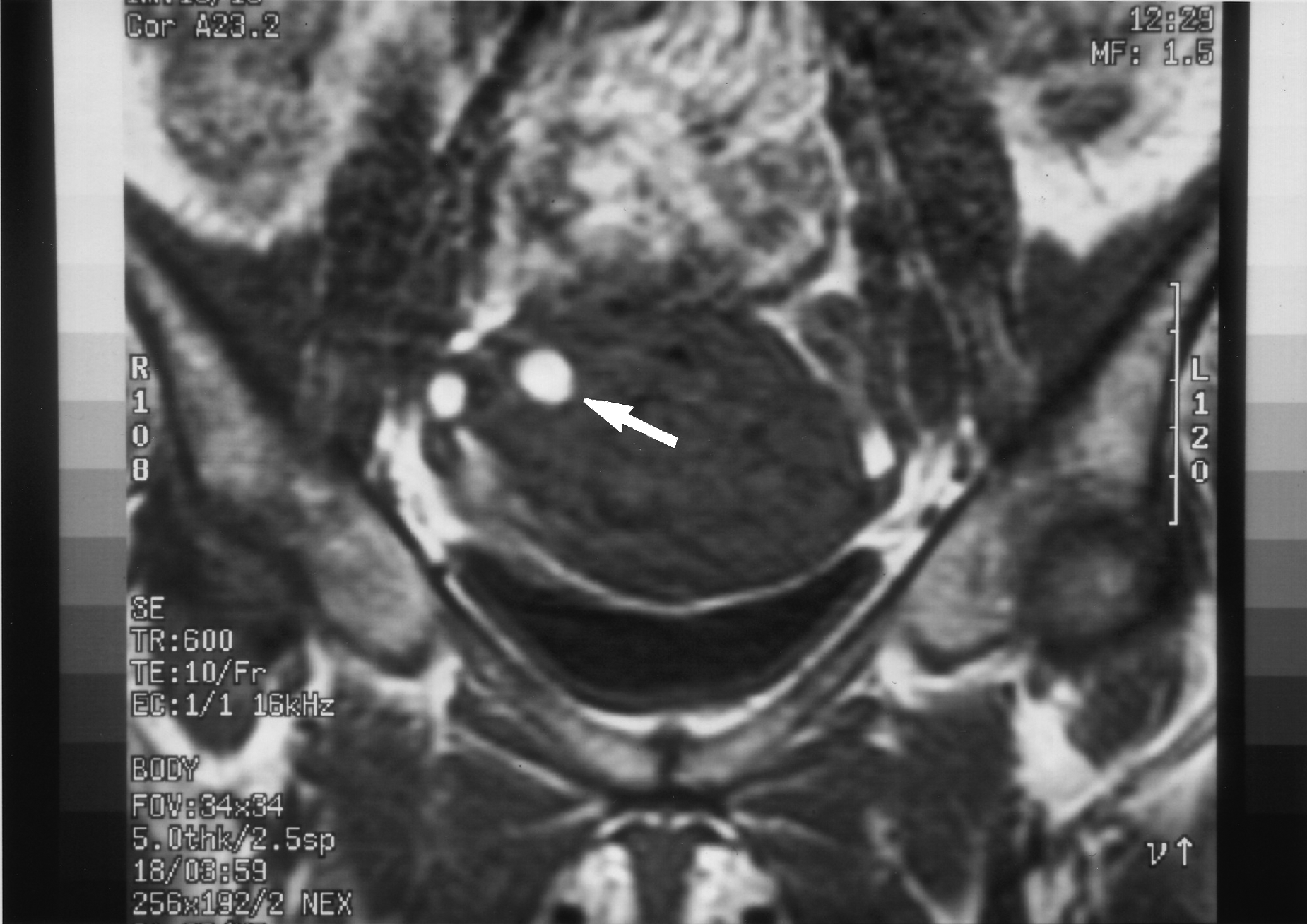
Magnetic resonance imaging scan in the coronal plane (T2-weighted spin echo image) shows a right cornual hematometra (white arrow). (Used with permission from Elsevier.)
Treatment of CH is difficult because the intrauterine scarring may be dense. The hematometra can be difficult to locate and drain without perforating the uterus. The best approach is to use an operative hysteroscope under ultrasound guidance to drain the CH and then resect or ablate the endometrium that has caused the bleeding. The surgeon must be cognizant that cornual myometrium is thin and easily perforated. Unfortunately, even if the CH is successfully drained and the area ablated, the hematometra often recurs and necessitates a hysterectomy.
Postablation Tubal Sterilization Syndrome (PATSS)
PATSS (Fig. 4) can occur in sterilized patients who have had an endometrial ablation. If postablation scarring obstructs cornual bleeding, the blood can create retrograde pressure and distend the occluded fallopian tube, thus causing significant pain. PATSS was originally described by Townsend et al. 13 They presented 6 patients with a history of a tubal ligation, in whom severe unilateral or bilateral lower abdominal pain occurred 6–10 months after a total rollerball endometrial ablation. All of the patients were evaluated by laparoscope and hysteroscope and were found to have a contracted scarred endometrial cavity, CH, and a hematosalpinx of the proximal tubal stump. The term PATSS was coined to describe this complication.
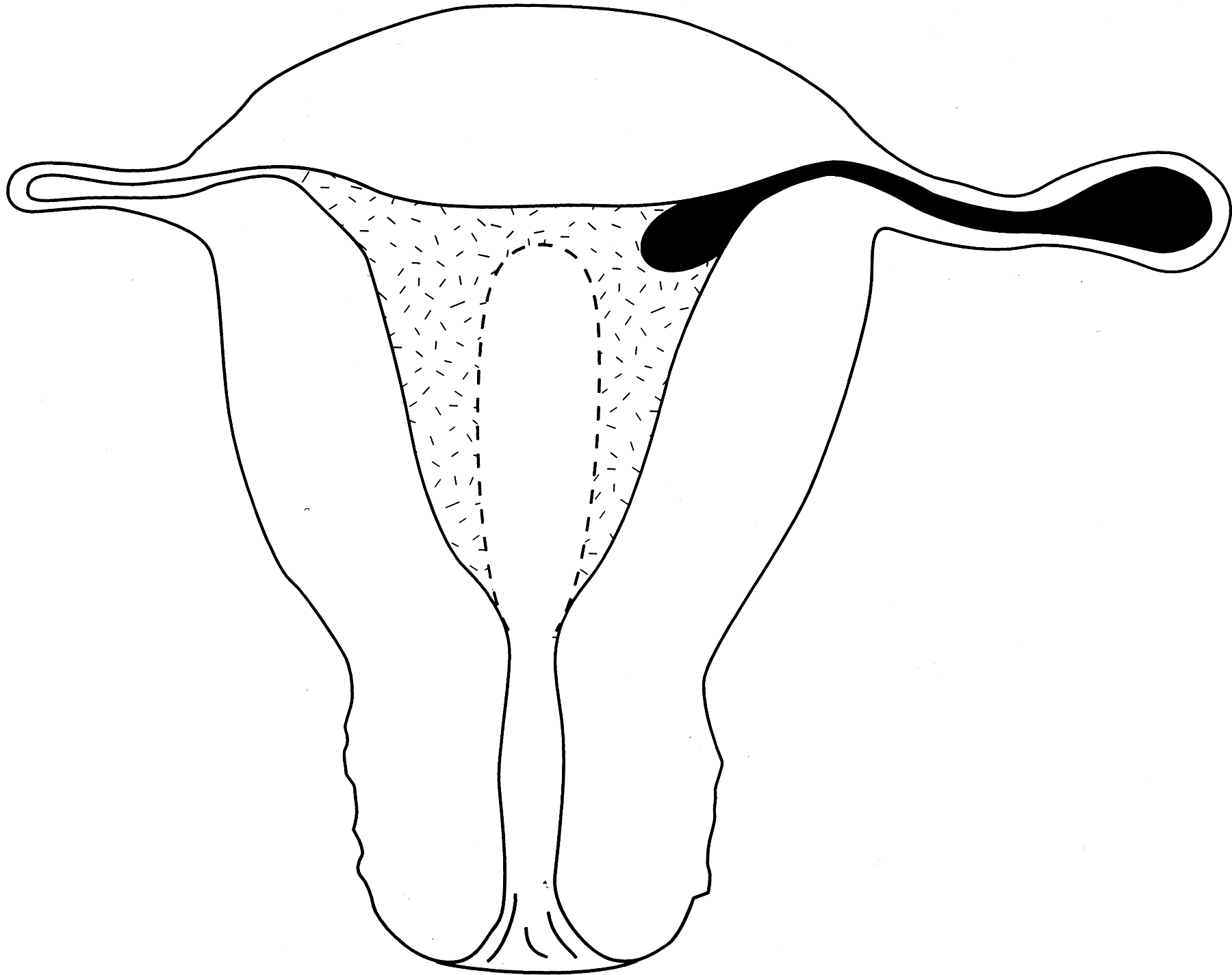
Drawing showing postablation tubal sterilization syndrome with an intrauterine contracture (stippled area), left cornual blood, and left hematosalpinx (black area). (Used with permission from Elsevier.)
PATSS should be suspected when a patient with a past history of a tubal ligation presents with cyclic unilateral or bilateral lower abdominal pain months to years following an endometrial ablation. The pain only occurs during the menstrual phase of the cycle even though the patient may be amenorrheic.
PATSS is a difficult diagnosis to make because there is often insufficient blood in the cornual region and proximal tubal segment to be easily visualized by an ultrasound or computed tomography scan. An MRI scan (Fig. 5) is usually necessary to detect the hematosalpinx. Radiologists must be educated about PATSS since most are not aware of this condition, although The Year Book of Diagnostic Radiology, 2003 edition 14 thoroughly covered this subject. MRI studies must be performed when a patient is symptomatic during the menstrual phase of her cycle, whether or not she is amenorrheic. This cannot be overemphasized, since hematosalpinx and cornual blood can absorb during the nonmenstrual phase of the month and the diagnosis will therefore be missed.
Magnetic resonance imaging scan in the coronal plane (T2-weighted spin echo image) shows a right proximal hematosalpinx (white arrow) that confirms a postablation tubal sterilization syndrome. (Used with permission from Elsevier.)
It has been questioned whether this small hematosalpinx can cause the great amount of pain that patients experience with PATSS. The authors believe that it can for three reasons: First, the pain is always on the same side as the hematosalpinx. Second, when the hematosalpinx is surgically removed, the pain immediately goes away. Third, one of the senior author's patients who had PATSS was an MRI technician and scanned herself throughout the month. When she was experiencing the pain, the hematosalpinx could be seen but when the pain abated, the blood was absorbed and the hematosalpinx could not be visualized. This clearly again emphasizes the importance of scheduling the MRI at the appropriate time of the menstrual cycle.
The initial treatment of PATSS is surgical removal of the hematosalpinx and drainage of the cornual blood. As discussed in the CH section of this review, such treatment is technically difficult, the CH often recurs, and a hysterectomy is required.
CH and PATSS have been described after both resectoscopic and nonresectoscopic (GEA) ablations. After resectoscopic ablations, the incidence of CH has been quoted as being between 10% and 18% and PATSS between 8% and 33% in patients who have had a tubal ligation. 1 The longer studies demonstrate the highest incidence of CH and PATSS. We 15 followed 50 consecutive patients who had a total rollerball endometrial ablation for at least 10 years. Symptomatic CH and/or PATSS were diagnosed in 5 of 50 patients (10%) by ultrasound scanning and/or MRI and confirmed at surgery. Since MRIs and/or ultrasounds were only performed on the 5 symptomatic patients and not on the other 45, the 10% incidence may be underestimating this problem. Two (2) patients had CH and 3 had PATSS, 4–90 months after the ablation. Of the 50 patients, 9 had a previous tubal ligation and 3 (33%) ended up with PATSS.
Although CH and PATSS have been reported after nonresectoscopic ablations, the actual incidence is not known because the follow-up time of these newer procedures is shorter. The incidence of these obstructive problems is most likely understated because of the difficulty in making the diagnosis as discussed above. If a hysterectomy is performed on a patient for postablation pain, the surgeon must specifically tell the pathologist to serially section the cornu and proximal oviduct to see if blood is trapped in these areas. Uterine sections in these regions are not routinely taken by pathologists. One must also realize that if the uterus is not removed during the menstrual phase of a patient's cycle, trapped blood may not be detected since it has been absorbed during the remainder of the menstrual cycle. Timing of imaging and surgery is therefore critical. Until gynecologists, radiologists, and pathologists are educated about these obstructive problems, diagnoses of CH and PATSS will continue to be missed.
The short-term success rates following both resectoscopic and nonresectoscopic endometrial ablations are excellent. Over time, however, this success drops and the hysterectomy rate increases. The main indications for these hysterectomies are for pain and/or bleeding.
The ACOG Practice Bulletin, May 2007 edition 16 states that hysterectomy rates within 4 years following both resectoscopic and nonresectoscopic endometrial ablations are at least 24%. Furst et al. 17 published an article on the long-term follow-up after resectoscopic endometrial ablations. They followed 120 patients for at least 10 years and found that there was a 43% hysterectomy rate in women younger than 40 years old at the time of their ablation. Longinotti et al. 18 performed a large study on 3681 women who had either a resectoscopic or nonresectoscopic endometrial ablation. The later procedures included thermal balloon ablation, hydrothermablation, radiofrequency ablation, and cryoablation. If patients were 40 years old or younger at the time of their ablation, 40% ended up having a hysterectomy and rather than plateauing, this rate continued to increase throughout the 8-year follow-up. The results were similar for all types of endometrial ablation procedures and independent of leiomyomata. The main indications for the hysterectomies were bleeding (51.6%), pain (22%), and bleeding with pain (20.3%). Therefore, 42.3% of patients had a component symptom of pain.
Dickerson et al. 19 published a randomized controlled trial comparing hysterectomy with endometrial ablation for the treatment of persistent uterine bleeding and called it the STOP-DUB study. The ablation techniques studied were resectoscopic ablation using electrodessication/coagulation and nonresectoscopic ablation using thermal balloon. They found that almost one third of the women they studied had a reoperation (mainly hysterectomy) within 5 years. Pain and/or bleeding were the main indications for reoperation but pain was the most prevalent. The outcome was the same for all the ablation techniques.
Vilos et al. 20 studied indications for hysterectomy after endometrial ablation. Of 163 hysterectomies, the indications were for bleeding in 20 (12.3%), pain in 105 (64.4%), and both in 38 (23.3%). Therefore, 87% had a component of pain.
These long-term studies are confirming that pain is a major indication for hysterectomies following both resectoscopic and nonresectoscopic ablations. What is actually causing this postablation pain?
Adenomyosis is often found in hysterectomy specimens from patients who are experiencing postablation pain. However, it is controversial whether adenomyosis alone is the cause of the pain.
We12,21 have studied adenomyosis extensively and found that it is a major reason for endometrial ablation failure since it can cause persistent abnormal uterine bleeding. However, we found that the dysmenorrhea often associated with preexisting adenomyosis stayed the same or improved after an ablation. Patients with adenomyosis who experienced increasing postablation pain were found to have an obstructive problem such as CH and/or PATSS.
The actual incidence of CH and PATSS will not be known until gynecologists, radiologists, and pathologists become aware of these painful obstructive problems and how best to make the diagnosis.
Postablation Cornual Endosalpingoblastosis (PACE)
PACE occurs when the tubal epithelium of the intramural oviduct next to the tubal ostia is injured during an endometrial ablation. This injury can activate the tubal epithelium, which has the potential of growing into the cornual myometrium.
It has been shown that injury to the tubal epithelium in the intramural and/or proximal oviduct can activate this tubal tissue. Sampson 22 originally described this tubal activation seen after cornual resection and coined the term “endosalpingiosis.” He did not understand the clinical significance of endosalpingiosis but realized that it could be a painful lesion. During laparoscopic sterilization, Rock et al. 23 found that cautery injury of the fallopian tube within 4 cm of the uterine cornu may predispose to development of “endometriosis” and subsequent fistula formation at the proximal tip of the ligated tube or cornual area. We 24 discovered a similar pathologic problem when the proximal oviduct adjacent to the uterus was coagulated during laparoscopic tubal fulguration and coined the term “endosalpingoblastosis.” This series showed that the activated tissue can cause uteroperitoneal fistulas, which are associated with a high rate of ectopic pregnancies after laparoscopic tubal coagulation failure. In contrast, injury to the middle or distal oviduct causes a normal fibrotic reaction without tubal activation. Maker et al. 25 studied 25 patients who had undergone tubal sterilization and eventually had a hysterectomy. They found that patients who had tubal electrocoagulation close to the cornu developed endosalpingoblastosis associated with tubal or uteroperitoneal fistulas.
The term endosalpingoblastosis is more appropriate than endosalpingiosis or endometriosis because pathologic studies reveal that both tubal and endometrial epithelium usually invade the cornual myometrium 24 (Fig. 6).
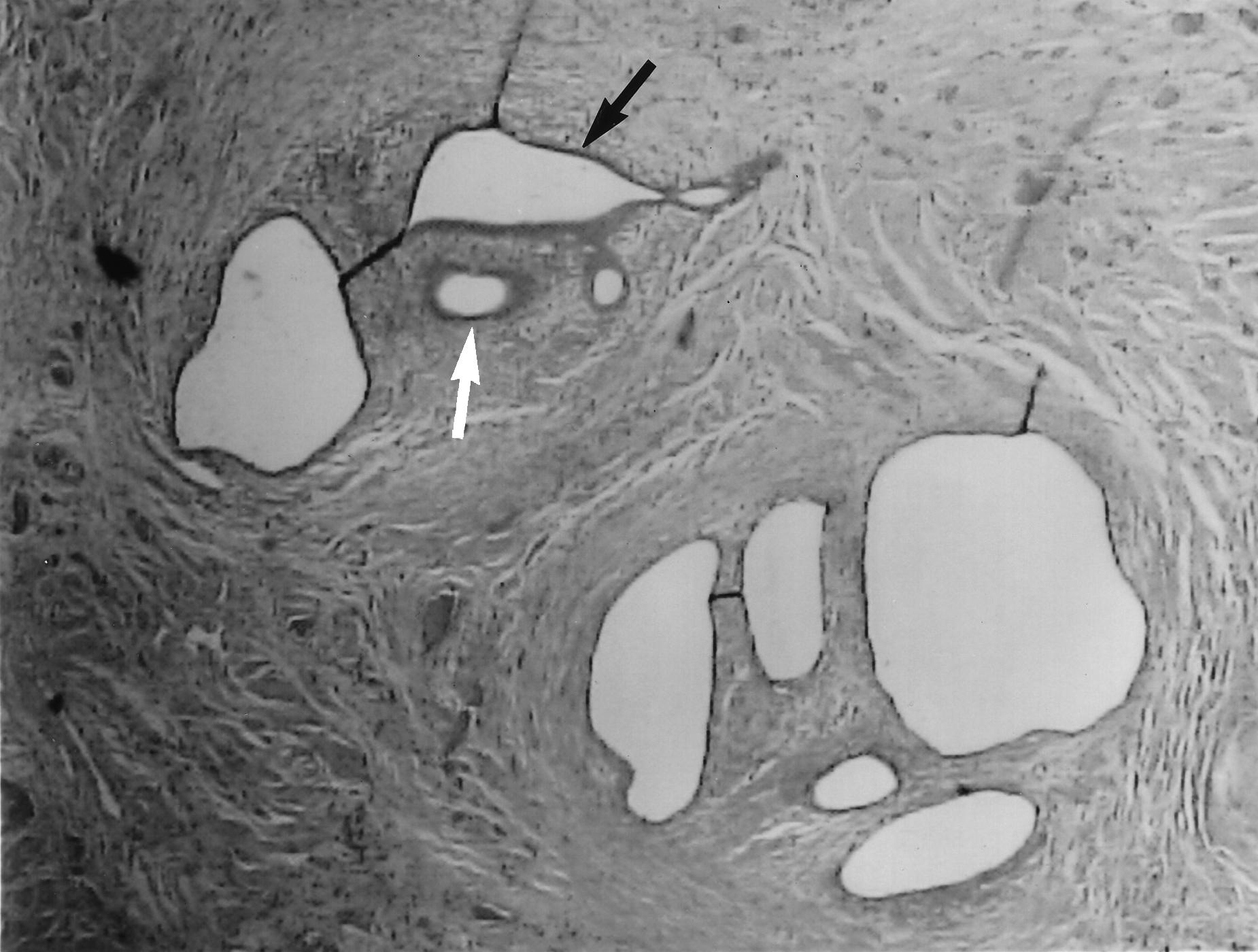
Photomicrograph showing both tubal (black arrow) and endometrial (white arrow) epithelium invading the cornual myometrium (postablation cornual endosalpingoblastosis).
When the cornual areas are specifically studied in postablation hysterectomy specimens, endosalpingoblastosis has been found there. The term postablation cornual endosalpingoblastosis (PACE) was coined to describe this process. 15 In 1 patient having a hysterectomy for persistent painful CH, activated tissue was found to grow through the cornual serosa and into the sigmoid colon (Fig. 7). Sampson 22 described a similar case of cornual endosalpingiosis growing into the colon after a cornual resection.
Drawing shows intrauterine contracture (stippled area) with a left corneal hematometra and postablation cornual endosalpingoblastosis invading left cornual myometrium and colon.
It usually requires 3–5 years for endosalpingoblastosis (PACE) to develop following injury to tubal ostia epithelium and/or the intramural oviduct. It will therefore require a long-term histopathologic study of postablation and/or resection hysterectomy specimens, where the intramural oviducts and cornual areas are serially sectioned, to determine the true incidence and clinical significance of PACE.
Postablation Endometriosis
Endometriosis, as well as central hematometra, CH, PATSS, and adenomyosis are some of the pathologic conditions found in patients who eventually develop cyclic pain following an endometrial ablation and/or resection.26,27 If endometriosis is found, it is usually not known if it was present before or occurred after the procedure.
The etiology of endometriosis is still debated, but significant retrograde bleeding from congenital or iatrogenic cervical or intrauterine obstruction is considered one of the causes.
Olive et al. 28 studied women with retrograde menstruation secondary to congenital müllerian outlet obstruction. Seventy-seven percent (77%) of these patients developed significant endometriosis.
Turnbull et al. 8 in their postresection/ablation MRI study, detected free intraperitoneal fluid in 32 of 59 patients (54%) studied. Eleven (11) were amenorrheic and no additional extrauterine pelvic pathology was apparent. As radiologists, they state that this was an unexpected finding and probably due to retrograde bleeding since T2-weighted MRIs are able to determine if peritoneal fluid is mainly blood. This is in contrast to women who have not had an ablation. Although retrograde bleeding can occur normally, it is not common in eumenorrheic women. Koninckx et al. 29 studied the volume and characteristics of peritoneal fluid by laparoscopic aspiration throughout normal menstrual cycles in 303 patients. They found that peritoneal fluid fluctuates throughout the month up to a volume of 20 mL but is usually an exudate and only bloody in 4.2% of patients.
Sorensen et al. 30 published an article entitled “Endometriosis by implantation: a complication of endometrial ablation.” They presented a case of a 44-year-old woman who had an endometrial resection for menorrhagia. She had no past history of pelvic pain or dysmenorrhea. Postoperatively, she was amenorrheic, but developed increasing dysmenorrhea every 4 weeks over the next 8 months. A sonogram revealed a cystic mass lateral and posterior to the uterine body. At hysteroscopy, the uterine cavity was observed to be shrunken with fibrotic walls. Laparoscopic evaluation demonstrated that the pelvis was partially filled with old organized blood clots. The distal two thirds of both fallopian tubes were distended with edema and blood. Blood clots were protruding through both tubal ostia. The uterus and ovaries appeared normal. A bilateral salpingectomy was performed, and pathologic examination demonstrated typical endometriosis in the mucosa of both tubes. Bae et al. 31 have also found histopathologic endometriosis in the tubal mucosa of patients with PATSS.
Future long-term studies will be necessary to determine whether postablation retrograde bleeding increases the incidence of endometriosis.
Pregnancy Following Endometrial Ablation
Pregnancy after an endometrial ablation and/or resection may be considered a long-term complication resulting from postablation intrauterine scarring. Cook et al. 32 reported on 43 pregnancies that occurred after endometrial ablation. These pregnancies were complicated by a high risk of abnormal placentation, spontaneous abortion, preterm delivery, and cesarean hysterectomy.
Xia et al. 33 further emphasized that pregnancy-related complications are often synechiae related. They report a 12% ectopic rate (usually cornual or cervical), high miscarriage rate, as well as preterm premature rupture of membranes.
Mukul and Lim 34 describe postablation synechia-related fetal limb malformations. Also confirmed are a high accreta/percreta and uterine rupture risk with subsequent cesarean hysterectomy.
Patients must understand that endometrial ablation is not a sterilization procedure, and major complications can occur if they become pregnant after the procedure.
Therefore, consideration must be given to contraception when counseling patients for endometrial ablation.
Endometrial Cancer Following Ablation
Many physicians are concerned that postablation intrauterine scarring may obstruct postmenopausal bleeding from an endometrial cancer and delay the diagnosis.
It has been shown that cervical or lower uterine segment obstruction can influence prognosis. Schneider et al. 35 studied 7 patients who had a lower uterine stenosis from a previous cervical amputation and who developed endometrial cancer. In 6 of these patients, the cervical stenosis prevented early uterine bleeding. Four (4) of these patients when diagnosed were in an advanced surgical stage of the disease (stage II and III) and all died thereafter. The authors recommend periodic ultrasound of the endometrium in patients at risk of having a lower uterine segment obstruction or cervical stenosis to rule out obstructed endometrium.
Margolis et al. 36 reported the first case of asymptomatic endometrial cancer after endometrial ablation. The patient underwent a total rollerball ablation for abnormal bleeding. A large benign polyp was resected at the time of the ablation. The patient was amenorrheic after the procedure but developed urinary stress incontinence. She underwent a total abdominal hysterectomy, bilateral salpingo-oophorectomy, and a Marshall-Marchetti-Krantz retropubic suspension procedure approximately 2.5 years after the ablation. The pathology revealed grade 1–2 adenocarcinoma of the endometrium that had invaded >50% of the myometrium (International Federation of Gynecology and Obstetrics stage IC).
Valle and Baggish 37 reviewed the world literature and found 8 patients with endometrial cancer after endometrial ablation. Most of the patients had high risk factors for this type of cancer. The authors recommended that patients with high risk factors, particularly an endometrial biopsy demonstrating hyperplasia, who are not responsive to progestin therapy, are not good candidates for endometrial ablation.
Bradley 38 states that if an endometrial ablation is performed in high-risk women for endometrial cancer, the procedure can prevent the egress of blood, foster development of synechiae, render endometrial biopsy difficult to impossible, and potentially bury endometrial cells deeper within the myometrium, all of which contribute to a delay and “upstaged” diagnosis of endometrial cancer.
Most women who develop endometrial cancer at younger ages have high risk factors such as obesity, diabetes, hypertension, and/or polycystic ovarian syndrome. Endometrial cancer, however, has a higher prevalence in postmenopausal women and many of them do not have these risk factors. MacMahon 39 found that approximately 50% of patients in whom endometrial cancer developed have no identifiable risk factors. Therefore, it is difficult to select out all patients who may eventually develop endometrial cancer.
Cooper and Brady 40 states that the newer ablation techniques that are easier to perform have enticed more gynecologists to try using GEAs. Although they empower the physician to offer more advanced minimally invasive options to patients, these tools simultaneously can tempt the surgeon to forgo meticulous preoperative evaluation. Most GEAs do not require visualization of the endometrium and thus bypass an important diagnostic tool that can demonstrate intrauterine pathology.
Some physicians believe that the incidence of endometrial cancer will be reduced after an ablation procedure because the endometrium has been resected or destroyed. However, as stated earlier in this review, endometrial tissue either persists or regenerates in up to 95% of patients.
Neuwirth et al. 41 studied the incidence of endometrial cancer following an ablation in patients who had normal preoperative endometrial histology. Their data analysis shows no increased or decreased risk of endometrial cancer in this group of patients.
Another concern is retrograde bleeding following an endometrial ablation. As stated earlier, Turnbull et al. 8 in their postresection/ablation MRI study, found that 32 of 59 patients (54%) studied had evidence of retrograde bleeding. This brings up an important theoretical question. In patients who develop endometrial cancer following a total ablation and/or resection, will retrograde bleeding caused by a postablation intrauterine obstruction force significantly more malignant cells into the peritoneal cavity than is found in patients without an intrauterine obstruction? Will the incidence of metastatic disease and the prognosis be affected?
Studies have shown that during fluid hysteroscopy, endometrial cancer cells can be pushed through the oviducts into the peritoneal cavity, but this brief exposure does not appear to affect prognosis. However, will prognosis be compromised in postablation patients who experience prolonged retrograde bleeding from an obstructed endometrial cancer? Does prolonged peritoneal exposure to malignant cells in retrograde bleeding lead to metastatic disease? At this time, we do not know the answer to these questions; however, Havrilesky et al. 42 have shown that positive peritoneal cytology is an independent predictor of prognosis among patients with stage I-IIIA endometrial cancer. They found among patients with stage IIIA endometrial cancer, metastasis to the adnexa or serosa does not appear to confer a worse prognosis than positive cytology alone.
Horowitz et al. 43 published the first case of a metastatic lesion following an ablation in a patient with endometrial cancer. The patient was an obese, diabetic 64 year old who had an endometrial ablation for persistent postmenopausal bleeding. A dilation and curettage at the time of ablation demonstrated an endometrial polyp together with glandular hyperplasia and cellular atypia. Definitive surgery was not done at that time because the patient had a high surgical risk. Fourteen (14) months after the ablation, a metastatic periumbilical nodule was found and definitive surgery was performed. The hysterectomy specimen revealed a poorly differentiated adenocarcinoma and the patient died 4 months later.
Baggish et al. 44 in their authoritative text on hysteroscopy, state that endometrial ablations should not be performed as a means of eliminating postmenopausal bleeding since the risk of masking and delaying the diagnosis of endometrial malignancy far outweigh any benefit accrued by the cessation of bleeding.
Most of the patients who have had an endometrial ablation procedure are not yet in the age group at risk of developing endometrial cancer. The mean age for patients having an endometrial ablation is 40.5 and the mean age of a woman developing endometrial cancer is 64.4, almost a 24-year differential. Since ablations became popular in the mid 1990s, it will take another 10 years of follow-up before we know the full extent of this problem.
Until this issue is resolved, McLucas 45 recommends periodic pelvic ultrasound scans to evaluate the endometrial echo complex (EEC) in high-risk and postmenopausal women to rule out any obstructed endometrial growth.
Postablation Intrauterine Evaluation Is Problematic
Postablation pelvic ultrasound examination to evaluate the EEC is employed not only for periodic screening but also to evaluate patients who return with abnormal uterine bleeding or postmenopausal bleeding following their ablation. If an abnormal EEC is found, it is difficult to evaluate for two reasons. First, it has not been determined what an abnormal EEC is after a patient has had an ablation. It is not known if an endometrial thickness (stripe) measuring less than 4–5 mm is also considered normal in patients who have had an ablation. Second, if an abnormal EEC is discovered, postablation scarring makes it difficult to evaluate the intrauterine cavity thoroughly. Endometrial biopsies, which are a simple office diagnostic procedure, are unreliable after an ablation. An ultrasound-guided operative hysteroscopy is often necessary but dense intrauterine scarring can distort the intrauterine cavity making it difficult to access all endometrial tissue. Even if endometrial tissue is obtained, it is difficult to ascertain whether the sample is complete. Often, a hysterectomy is necessary just to resolve this problem.
Of all the obstructive phenomena discussed in this review, the inability to accurately evaluate the intrauterine cavity after an ablation is evolving into a major practical problem. It is concerning that ablations make future endometrial biopsies have little to no diagnostic value. Taking away our ability to perform this simple in-office procedure to evaluate patients who return with postablation abnormal uterine bleeding, postmenopausal bleeding, or an abnormal EEC is problematic.
The FDA physician advisory committee expressed concern about these long-term problems when asked for help in developing a clinical trial to determine if “cosmetic ablations” were safe. “Cosmetic ablations” are defined as an endometrial ablation for women seeking elective cessation of menses. After the committee was educated about these postablation long-term complications, they strongly resisted approving any studies on “cosmetic ablations.” The main reason for disapproval was that the long-term risk of postablation obstructive complications is too high merely to warrant eliminating normal menstrual periods. 46
Horowitz et al. 43 state that only with long-term follow-up will the true safety and efficacy of endometrial ablation be defined.
Prevention of Postablation Obstructive Problems
As with any new technology, modifications are sometimes necessary to prevent delayed or long-term complications. A partial endometrial ablation (PEA) was developed to treat menorrhagia without causing intrauterine scarring, thus avoiding the obstructive problems cited above. A PEA only ablates or resects the anterior or posterior endometrial wall and avoids injury to the cornual areas. When only one wall is injured, it heals in juxtaposition to a normal, uninjured endometrial surface on the opposite wall. The injured and uninjured surfaces do not grow together. Intrauterine contracture and adhesions are therefore prevented, leaving the cavity open.
In a partial ablation, the cornual areas are not ablated for two reasons. The first reason is to avoid scarring in the area so that any future bleeding from cornual endometrium is not obstructed. The second reason is to avoid injury of the tubal ostia to prevent activation of this tissue (PACE).
After a partial ablation, the intrauterine cavity stays open, thus preventing obstructive problems and allowing for easy access if future evaluation becomes necessary. Endometrial biopsies and diagnostic hysteroscopy can be successfully performed. Hypomenorrhea or eumenorrhea, not amenorrhea, is the goal.
An initial study of partial ablation was performed on 50 patients with ovulatory menorrhagia. 47 All had failed medical treatment and had a normal-appearing cavity without gross polyps or submucous myomas by hysteroscopy. The menorrhagia was corrected in most patients. After a 3-year follow-up, 76% were satisfied, 10% were partially satisfied, and 14% were not satisfied with the results. Five (5) hysterectomies were performed for recurrent menorrhagia and all specimens had deep adenomyosis. Inspection of the intrauterine cavity was performed 4–26 months after the partial ablation. None of the patients were found to have intrauterine adhesion or contracture after partial ablation. The entire cavity, including both cornual areas, was open and both tubal ostia could be visualized. The authors have now preformed over 1000 partial ablations with similar results. No obstructive problems have occurred after a PEA.
Another alternative to treat menorrhagia without causing obstructive problems is to insert a levonorgestrel-releasing intrauterine system (LNG IUS), which has been shown to be successful in reducing uterine bleeding. Lethaby et al. 48 in their Cochrane review, found that although the LNG IUS treatment results in a smaller reduction in menstrual blood loss than does endometrial ablation and women encounter more short-term side-effects, there were no differences in the women's rates of satisfaction or quality of life.
Conclusions
Although the operative and short-term complications of endometrial ablation are well documented, the delayed or long-term complications and their significance are just now being understood. The main reason these delayed complications are occurring is that both resectoscopic and nonresectoscopic ablations remove the endometrium and expose intrauterine myometrium. At the end of the total ablation procedure, when the distention media or instrument is removed, these exposed myometrial walls collapse upon each other and have a natural tendency to grow together, causing intrauterine contracture and scarring. These changes may not only obstruct bleeding, from persistent or regenerating endometrium trapped behind the scar, but also make future evaluation of the intrauterine cavity difficult.
It is becoming evident that there is a higher failure rate when ablations are performed on younger individuals. Older patients have a higher success rate since many experience menopause before developing recurrent bleeding problems or delayed obstructive complications, which can take up to 7 years to develop. However, postmenopausal women who have had an ablation may still have intrauterine scarring that could obstruct future endometrial growth and compromise the ability to thoroughly evaluate the endometrial cavity.
Until gynecologists, radiologists, and pathologists are aware of these obstructive problems and how to diagnose them, being particularly cognizant that timing of the diagnostic study is critical, the true incidence of these delayed or long-term complications will not be known. Education of these physicians is also important so that the ablation techniques that cause the fewest long-term complications can be identified.
Footnotes
Acknowledgments
We thank Fernando Herrera, senior artist at the University of California at Davis Medical Illustration Department, and Dr. Richard Wertz for their invaluable help.
Disclosure Statement
The authors do not have any commercial, proprietary, or financial interest in the products or companies described in this review paper.