
Abstract
Abstract
Introduction
Case
A 30-year-old gravida 3 para 2 who confirmed her pregnancy by a urine gravindex test at 40 days of amenorrhea underwent an MTP (medical termination of pregnancy) with laparoscopic sterilization at a private nursing home in her hometown. She had minimal painless bleeding for 2 days following the procedure, but later, she developed fever and vomiting, for which she was hospitalized in a district hospital and was treated with antibiotics and intravenous fluids. She was investigated for PUO (pyrexia of unknown origin), as she had recurrent episodes of vomiting and fever for the following 3 months. She was diagnosed as having enteric fever after performing a serum Widal test, which was positive (1 in 80 dilution), and she was treated accordingly. Subsequently, as she felt fetal movements, she consulted a gyneclogist, who diagnosed an intrauterine pregnancy of 32 weeks' gestational age, with the fetus being in breech presentation with oligohydramnios.
When she presented to us, she was afebrile, normotensive, and had mild palor. On per abdominal examination, the uterus was 32 weeks in size and fetal parts were felt easily and the fetus was in the breech presentation. Suspicion of secondary abdominal pregnancy due to perforation of the uterus at the time of MTP was considered, and ultrasonography (USG) was performed. TAS (transabdominal sonography) revealed an empty, enlarged uterus with the placenta on its superior surface and a live fetus in breech presentation with a biometry corresponding to 33 weeks' gestation. Liquor (i.e., amniotic fluid) appeared scanty, and there were no congenital anomalies. A diagnosis of secondary abdominal pregnancy was made, and she was hospitalized and managed conservatively with oral hydration, with the intention of delivering her abdominally electively after the completion of 34 weeks. But, after 4 days of admission, she suddenly complained of abdominal pain, and, on examination, she had tachycardia of 120/min and tenderness of the abdomen. Hence, an emergency laparotomy was undertaken under spinal anesthesia. Figure 1 shows the findings on opening the abdomen: The uterus was enlarged to 12 weeks' size, and the fetal surface of the placenta (i.e., the shiny part) was seen superior to the uterus. The fetus was lying freely and transversely in the upper part of the peritoneal cavity in the right dorsosuperior position smeared with thick scanty meconium and was extracted as a breech with an Apgar of 8/10 at 1min′. The ruptured amniotic cavity is shown in Figure 2. The placenta was gently lifted up by pulling on the cord, and the maternal surface of the placenta was found to be attached to the lateral part of the left outer half of the tube and the infundibulopelvic ligament (Fig. 3A). There were flimsy omental adhesions to the membranes. The lateral half of the left fallopian tube proximal to the fallope ring was clamped and cut, and the left infundibulopelvic ligament was clamped and cut and ligated with black silk sutures and the placenta was removed. The left ovary was normal and free from adhesions. The right ovary and fallopian tube were normal. The right fallopian tube had a fallope ring at the ampullary region. The surface of the uterus did not show any evidence of perforation. There was no postpartum hemorrhage, and blood loss was only around 250 mL. She was transfused 1 unit of compatible blood, as her preoperative hemoglobin level was 8 g/dL.
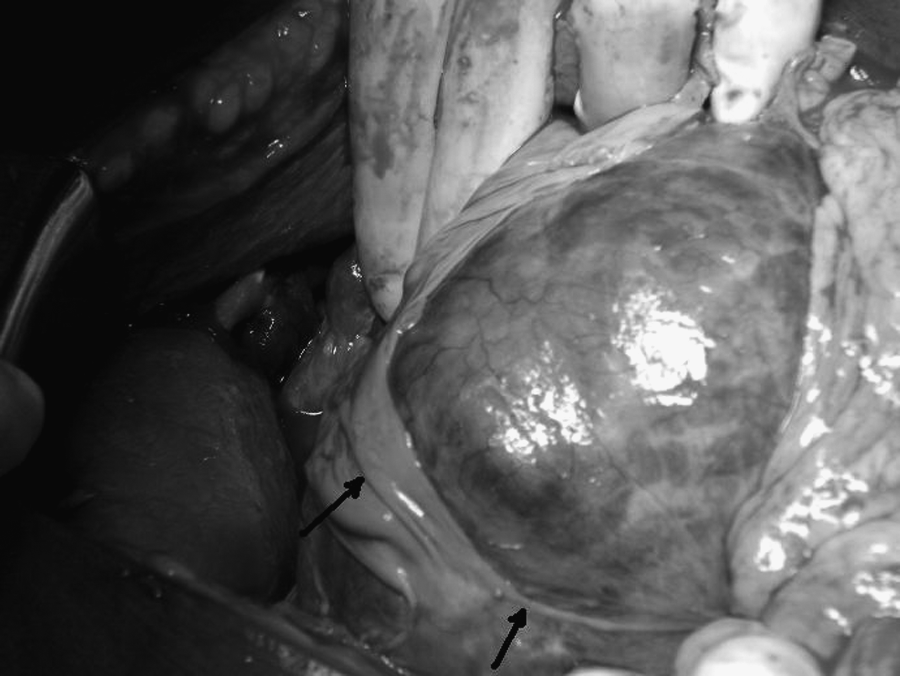
Findings on opening the parietal peritoneum before extracting the fetus. A 12-week-sized uterus is seen toward the right of the picture. The fetal surface of the placenta is seen toward the left and in the center. The arrow points to the ruptured amniotic membrane, which got folded.

Ruptured amniotic sac along with placenta which is lifted up.

(
On examination of the placenta (Fig. 3B), the fimbrial end of the fallopian tube could not be visualized, and it was incorporated into the maternal surface of the placenta. The fetus was female, weighed 2.8 kg, showed minimal cranial asymmetry on the right temporal region, and had no congenital malformations (Fig. 4). The patient recovered well and was discharged along with the baby on postoperative day 8.

The neonate. Minimal right facial asymmetry is seen.
Discussion
The development of ectopic pregnancy depends on complex interactions between many factors, although identifiable risk factors are often absent. 1 In the present case, the woman was multiparous and had no identifiable risk factors. In a large series, which assessed the symptoms with relation to the site of ectopic, abdominal pain was the most common symptom and its localization did not appear to have any relationship with the site of ectopic pregnancy. 2 This woman was asymptomatic in the initial 40 days, at which time she opted for MTP with sterilization.
In the present era, with the availability of β-HCG (beta-human chorionic gonadotropin) and imaging studies, the diagnosis of ectopic pregnancy is usually made early. The preoperative diagnosis of fimbrial pregnancy is very rarely made by USG. One (1) such case at early gestation was reported by Dahiya et al. 5 The present case, however, did not have USG before undergoing MTP with laparoscopic sterilization. The diagnosis was missed while performing laparoscopic sterilization, most probably because of ignoring or omitting to trace the fallopian tube in its entire length up to the fimbrial end prior to the application of the fallope ring.
Tubal pregnancy advancing to the third trimester is a very rare entity. The preoperative diagnosis is usually made as abdominal pregnancy on USG, as happened in the present case. The preoperative diagnosis can be missed, even in experienced hands, in 50% of the cases, and laparotomy is essential for a final diagnosis. 6 An unruptured fimbrial pregnancy, which had progressed to term and resulted in intrauterine death of the fetus, was reported by van der Bijil and Mabesa. The placenta, in this case, had derived its blood supply from the fallopian tube. 1 In the present case, the placenta was implanted on the fimbrial end of the tube and derived its blood supply from the vessels in the infundibulopelvic ligament. In the case described by Kocak et al., in which a 30-weeks-dead fetus was in the unruptured proximal falopian tube, the placenta derived its blood supply from the uterotubal angle. 6 In the case described by Lindgren, the right fallopian tube and the ovary were attached to the fetal sac, and, on histopathologic examination, the fimbria were thickened and were attached to the placenta by fibrous tissue. He established the diagnosis of fimbrial pregnancy, as the case did not fit in with the criteria of primary or secondary abdominal pregnancy, and there was no evidence of tubal rupture and no smooth muscle was found in the wall of the sac. However, the placenta, in this case, was implanted on the posterior wall of the pelvis, the right side of the cervix, and on the broad ligament, and the patient had severe hemorrhagic shock after removal of the placenta. In the present case, the placenta was quite free, as it could be lifted up easily, as shown in Figure 2, and, surprisingly, the only attachment it had was the fimbrial end of the fallopian tube and infundibulopelvic ligament.
Conclusions
Advanced fimbrial pregnancy resulting in live birth is a very rare entity. This case illustrates that if one is not careful in tracing the fallopian tube in its entire length, ectopic pregnancy can be missed, which may be fatal. It is also essential to perform a transvaginal USG prior to MTP in cases of early pregnancy to avoid this happening.
The blood supply at the fimbrial end is good enough for the fetus to grow in to the advanced stage. Onset of pain abdomen and tachycardia denote the rupture of the amniotic sac in cases of abdominal pregnancy on conservative treatment, and one should act up on it and do a laparotomy to save the fetus and mother from hemorrhage, as the separation of the placenta also can take place after a rupture of the amniotic sac, in some cases.
Footnotes
Disclosure Statement
No competing financial interests exist.