
Abstract
Abstract
Introduction
There are a variety of surgical procedures that may alleviate MBO. Surgical findings and performance status will ultimately dictate the most appropriate intervention. This may be a simple division of an adhesive band, bypass of an obstructed segment of bowel, or a more-extensive procedure involving bowel resection with or without reanastomosis.
Another common cause of bowel obstruction is late-radiation bowel toxicity, which may be responsible for intestinal obstruction requiring surgical intervention in up to 7% of cases postradiotherapy. 3 In addition, other coexisting situations, such as poor nutritional status or concomitant chemotherapy, are recognized factors that may compromise the intestinal epithelium further in intra-abdominal cancer patients.
This article presents a surgical technique for reestablishing intestinal continuity in patients presenting with proximal obstruction secondary to recurrent intra-abdominal disease. This novel technique serves two purposes: (1) maintenance of continuity between the afferent and efferent limbs of the bowel and (2) protection of the integrity of the newly created anastomosis by external venting.
The most common surgical practice is to protect an anastomosis in the unprepared bowel by a proximal stool diversion, although there is increasing literature that suggest that bowel preparation is not necessarily required for bowel resection and reanastomosis. 4
Typically, a resection involving the ileum and ascending colon requires a proximal loop ileostomy. 5 Carrying out this procedure involves surgery at two different sites and requires that the anastomotic site remains internal. What the authors propose is a simplified procedure to externalize the anastomotic site by venting it to the skin yet performing a sufficiently long anastomosis to permit reinstitution of bowel function within the abdominal cavity.
Case
A 51-year-old patient presented with recurrent carcinoma with signs and symptoms suggestive of severe MBO. Her abdominal and pelvic computed tomography can findings were consistent with this diagnosis, showing a dilated small bowel along with a decompressed colon. In addition, a transition point was evident (Fig. 1). The patient underwent surgical exploration with findings described hereafter.
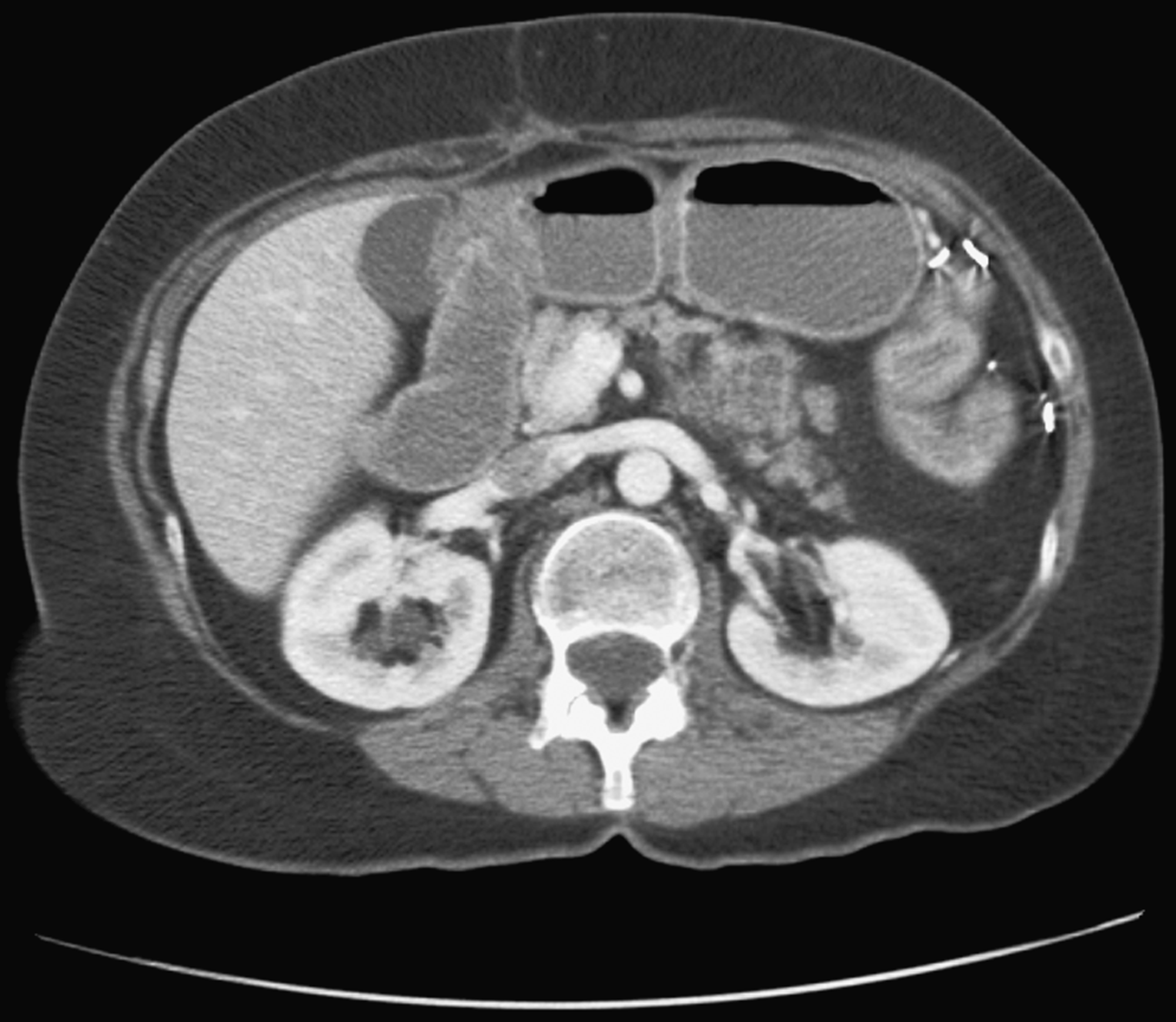
Preoperative computed tomography scan showing signs consistent with small-bowel obstruction.
Surgical procedure
A right paramedian incision was made, and the peritoneal cavity was entered by careful sharp dissection. Multiple bowel adhesions were seen but no carcinomatosis was noted.
Extensive lysis of adhesions was performed to free the distal third of the small bowel, the cecum, and the ascending colon. A significant radiation-induced inflammatory reaction was present around the terminal ileum and distal third of the small bowel. As a result, the terminal ileum and distal third of the small bowel were resected. At this point, a segment of proximal ileum, which was minimally affected by radiation, was identified. Having marked out this point, transection of the distal ileum was followed by gradual resection of all of the adherent loops from the pelvis up and away from the intact sigmoid colon. A solitary mass with central necrosis was found at this location and was completely resected. A decision was then made to carry out a double-barreled ileocolostomy.
Results
The postoperative patient's course was uneventful; the patient tolerated a solid diet on postoperative day 5. On postoperative day 7, she was discharged to go home in a stable condition. At the first-follow up visit, the expected gradual decrease in the ostomy output and a corresponding increase in rectal output were confirmed. Four (4) weeks later, the patient was taken to the operating room for definitive ileocolostomy closure. The techniques for both double-barreled ileocolostomy and definitive closure are described below.
Description of Surgical Techniques
Double-barreled ileocolostomy technique
In this case, the double-barreled end ileocolostomy was created first by performing a careful mobilization of the ascending colon and ileum from their mesentery as described above. Subsequently, the cecum was excised using a ILA-50 stapler (3M Company, St. Paul, MN) across the terminal ileum and an ILA-100 across the ascending colon (Fig. 2). Using interrupted 3-0 silk stitches; the colonic and terminal ileum ends were tacked together through the antimesenteric border for orientation. A 10-cm, side-to-side linear anastomosis was created by passing an ILA-100 stapler along the antimesenteric borders of the proximal ascending colon and the distal terminal ileum (Fig. 3). The distal end of the anastomosis was then temporarily closed transversely with a TA-60 (U.S. Surgical Corp., Norwalk, CT). In the right lower quadrant of the anterior abdominal wall, a temporary ostomy site was created by making a circumferential incision, which was dissected from the skin to the peritoneum, and the closed double-barreled ileocolostomy was exteriorized.

Limits of initial resection comprising the iliocecal valve.
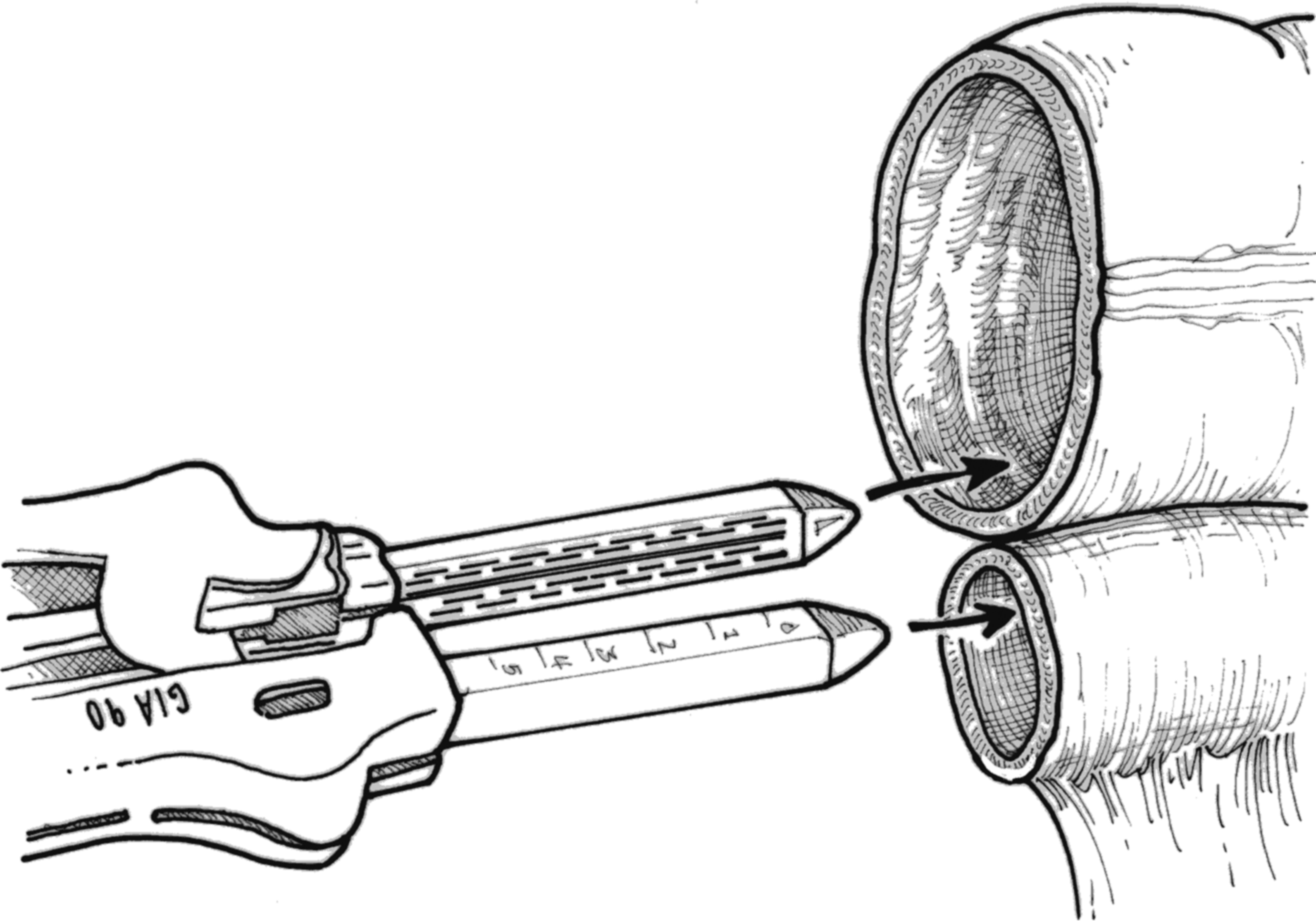
Mechanical suture is applied to approximate both intestinal lumen side-to-side.
This sequence of steps allowed construction of the anastomosis with easy access and a gentle exteriorization through the newly created ostomy site. Following completion of this step, a drain was placed in the pelvis close to the anastomosis. The abdominal incision was then closed in a standard fashion. The TA-60 staple line was then excised and the ileocolostomy was matured by suturing it to the anterior abdominal wall with interrupted 3-0 Vicryl sutures (Figs. 4 and 5).
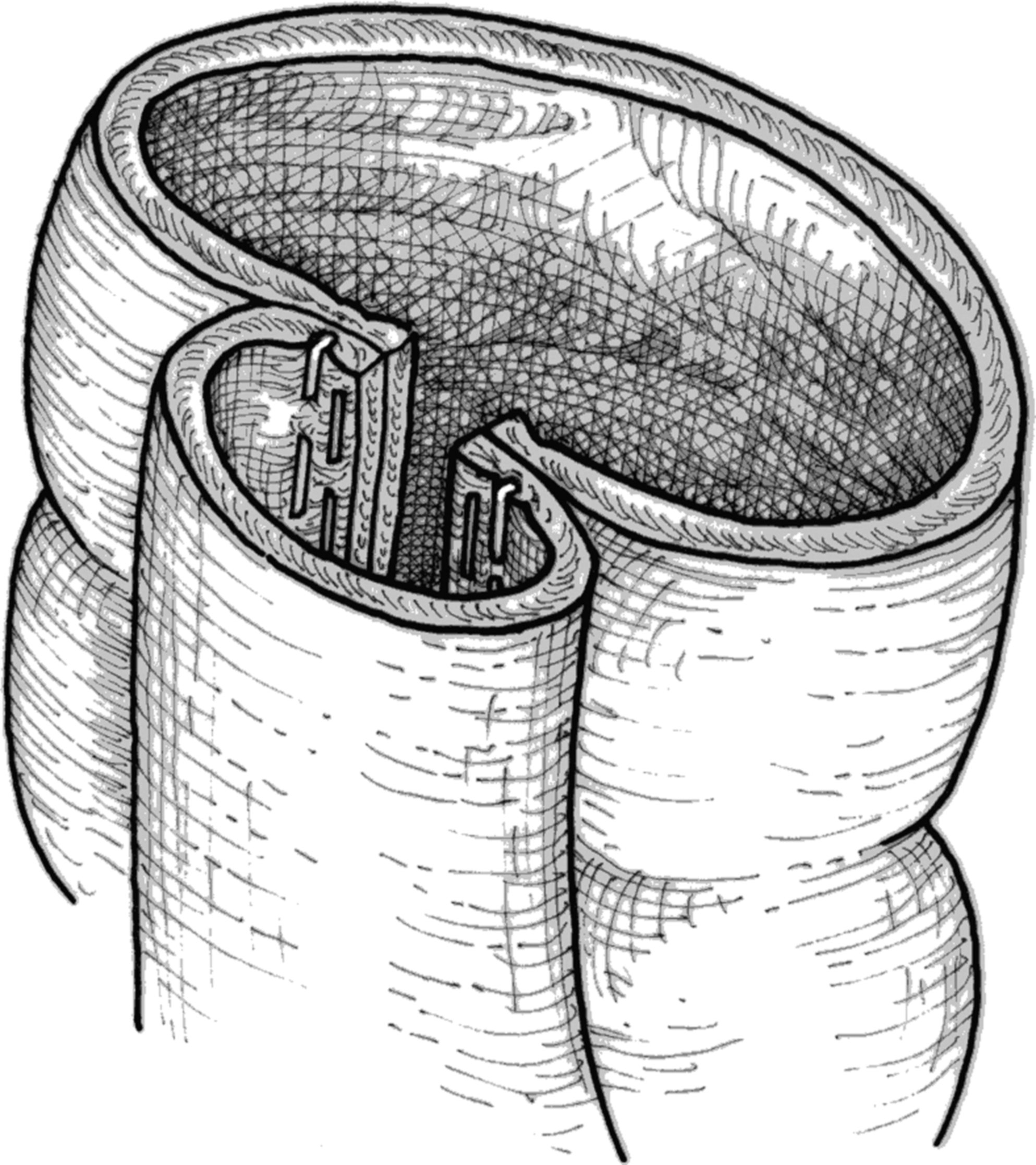
Double-barreled anastomosis is performed.
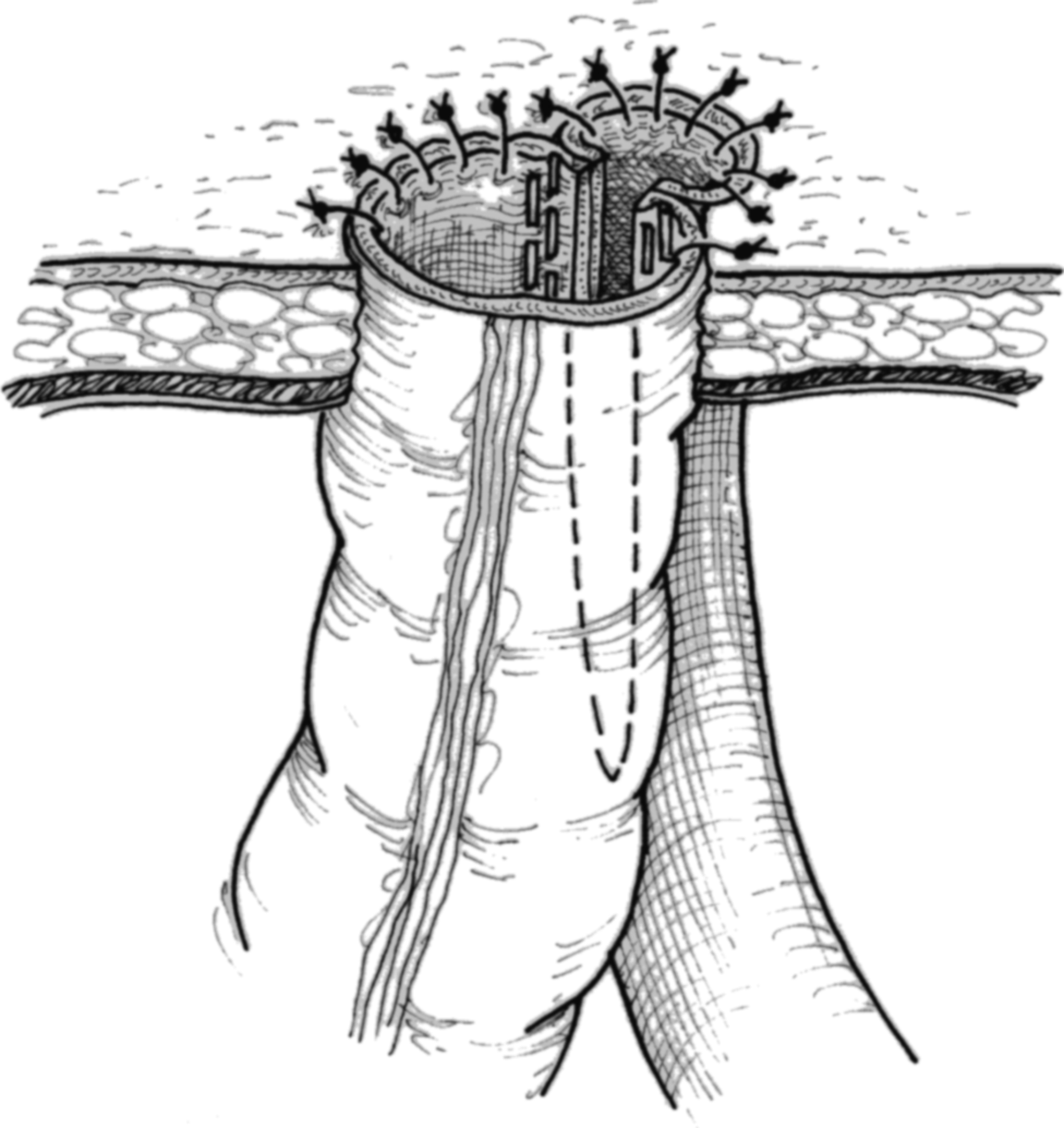
Venting of the double barreled anastomosis through skin using usual ostomy technique with interrupted suture.
Secondary anastomosis and ileocolostomy internalization
A circumferential incision encompassing the involved skin and the stoma itself was performed. Progressive dissection around the stoma was performed until the peritoneum was entered and the stoma was free. Then, closure of the patent lumen was carried out using an ILA-50, and the redundant mucosal tissue was excised (Fig. 6).

The mechanical suture is applied transversally to complete the anastomosis.
Once closed, the bowel was dropped into the peritoneal cavity and the peritoneum, muscle and fascia were reapproximated with Number 1 PDS sutures, using a standard Smead-Jones method. The skin and subcutaneous tissue were then loosely reapproximated with 3-0 nylon (Fig. 7).
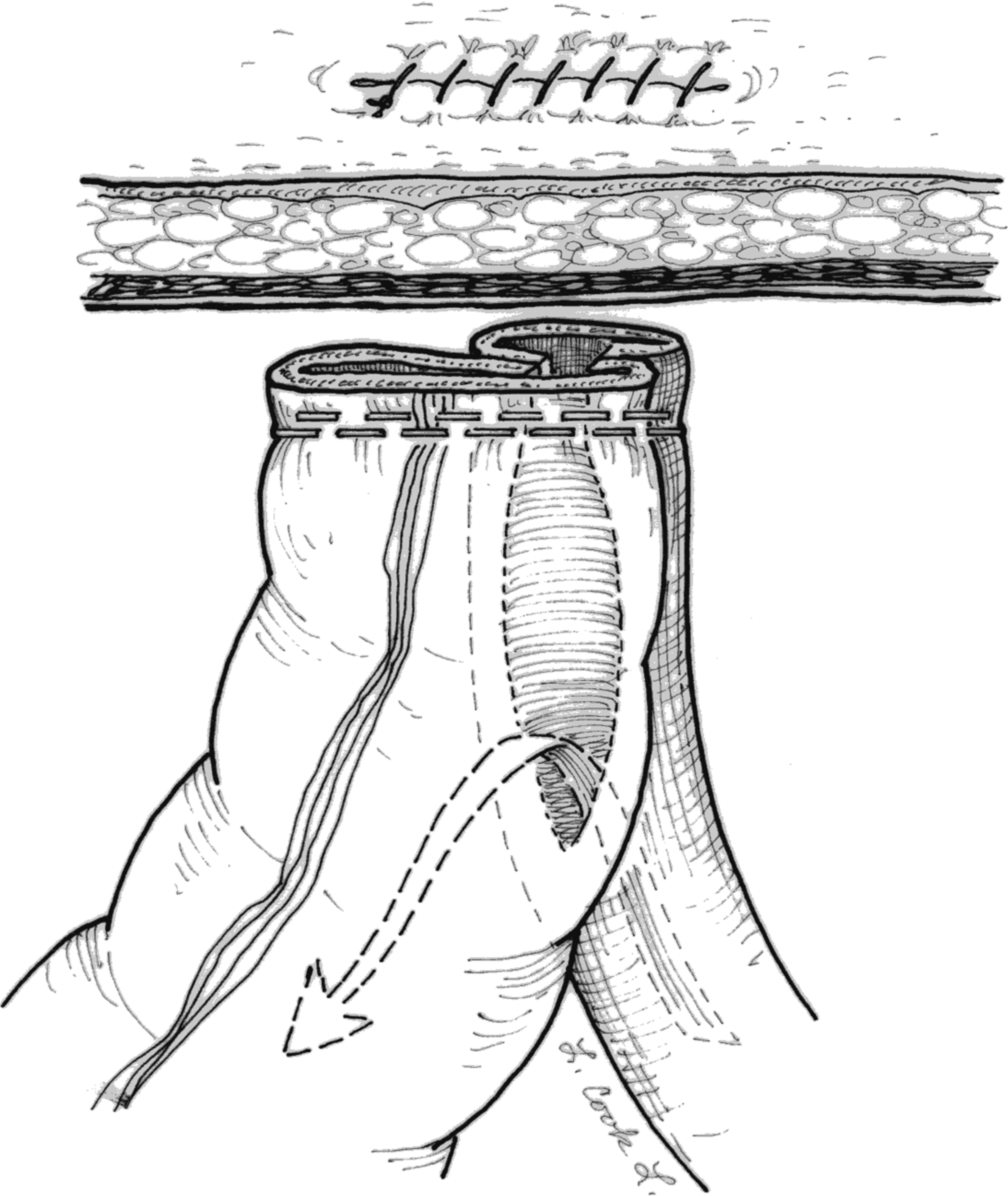
Skin and subcutaneous tissue are loosely reapproximated.
Discussion
Cancer patients with recurrent disease present a difficult challenge for management, both from the surgical and medical points of view. These patients frequently have a history of multiple lines of chemotherapy, prior abdominal surgical procedures, and often, radiation therapy to pelvic and abdominal fields. For patients presenting with MBO, management is generally focused on palliative rather than curative goals. Therefore, a balance must be made between expected survival and the anticipated impact of surgery on the patient's quality of life (QoL).
Palliative surgery for MBO in recurrent ovarian cancer patients is associated with a mortality and morbidity rates of up to 15% and 49%, respectively.6–8 Previous series have reported a median survival of 3–6 months in patients who present with bowel obstruction caused by recurrent ovarian cancer.9,10 It was recently reported recently that, when surgical correction of MBO was possible, almost 80% of patients were able to receive further chemotherapy, with an associated median survival of 9.7 months versus 2.4 for patients in whom surgery was not possible. 11 A pooled data analysis of 787 patients from 15 different studies of MBO caused by recurrent ovarian cancer showed that an attempt at surgical palliation in selected patients will result in a success rate of 90%, with an associated major complication rate of 32%. 11 However, a review of the literature reveals no consensus on criteria for selecting patients who are likely to benefit from surgery. Clinical parameters associated with poor outcomes for surgical management include extensive peritoneal carcinomatosis, presence of ascites, nutritional debility, and low performance status, along with concurrent medical illnesses. 12 Available literature supports surgical intervention in patients without contraindications and patients who have a life expectancy >2 months and who are candidates for further chemotherapy.13–15
For patients with distal small-bowel obstruction, such as the case presented here, the need for surgical correction is created by the failure of conservative management to alleviate obstruction, identifiable poor prognostic factors, and the good prospect of further chemotherapy.
Prompt recovery of bowel function supported the indication for definitive closure of the ostomy in this patient. Whenever feasible a concurrent rectosigmoid obstruction should be excluded preoperatively. This approach will help avoid reanastomosis proximal to a large bowel obstruction.
Conclusions
This new technique of double-barreled ileocolostomy is both feasible and simple. It may be a helpful technique for appropriately selected patients. The possibility of definitive closure and take down with a simple and brief surgical procedure is an added advantage of this technique. In addition, it may provide benefit for patients in terms of QoL and reduction in psychologic and economic burden associated with a definitive ostomy.
Footnotes
Disclosure Statement
No competing financial interests exist.