
Abstract
Abstract
Introduction
Case Report
A 36-year-old patient, at her first pregnancy and with a medical history psoriasis, cholecystectomy, and appendectomy, was referred to a gynecological emergency unit after 9 weeks of amenorrhea for blackened-sepia metrorrhage and pelvic pain. An interstitial ectopic pregnancy was diagnosed on the basis of positive serum human chorionic gonadotropin (29.034 U/mL) and the three echographic criteria of Timor-Tritsch:
1
empty uterus distance between gestational sac and uterine cavity > 1 cm myometrial mantle around sac
In this case, the diameter of the ovum was 42 mm, with the presence of an embryo with cardiac activity. Despite two iterative weight-adjusted injections of methotrexate (1 mg/kg), β-human chorionic gonadotropin did not fall, and an emergency laparoscopy was ordered.
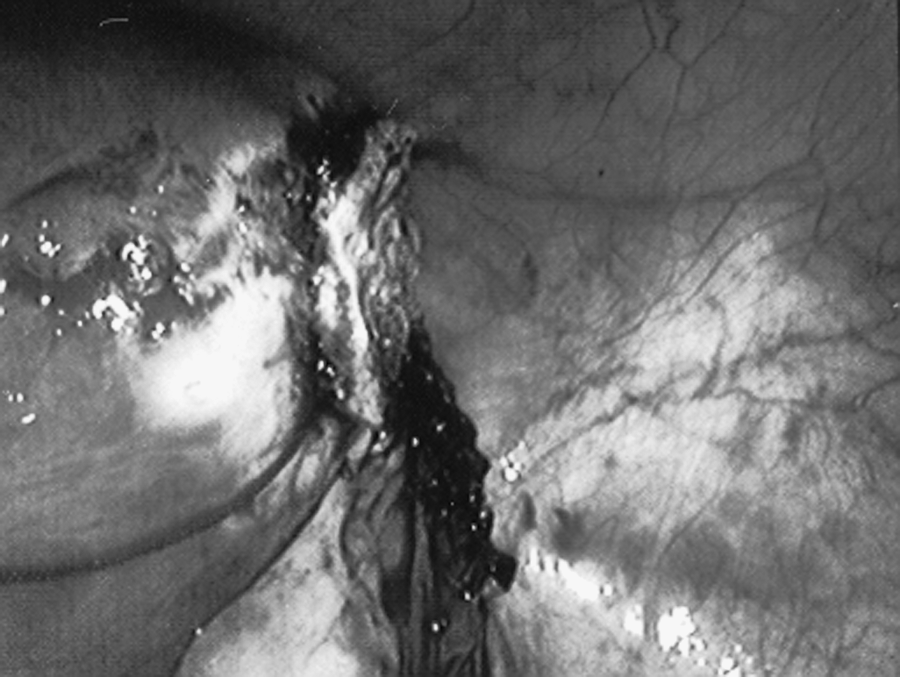
After the classical installation of a 10-mm umbilical cannula for the optical system, and three operating cannulae (one of diameter 5 mm in the right iliac fossa, one of diameter 5 mm in the left iliac fossa, and one subpubic cannula 10 mm in diameter), laparoscopic examination confirmed an intact right interstitial pregnancy without invasion of the Douglas space (Fig. 1).

Right interstitial pregnancy.
A retrograde right salpingectomy was performed (from the tube opening to the uterine horn) by a series of bipolar coagulations and endoscopic section of the mesosalpinx and right utero-ovarian ligament. Once the tube was pediculized, the endoloop was introduced through the subpubic cannula, positioned around the ectopic pregnancy, and tightened flush with the uterus (Fig. 2). The tube stump section was simply carried out endoscopically.

Fitting of the endoloop (top left of picture) at the base of the interstitial pregnancy. Maximum pull on the wire ensures hemostasis of the uterine horn.
There was no active bleeding at the uterine horn (Fig. 3). The operating section was extracted by means of an endoscopic sac through the 10-mm subpubic cannula. Blood loss was less than 50 mL and operating time was estimated at 30 minutes. Patient release was authorized on postoperative day 2. Negative serum human chorionic gonadotropin was confirmed on postoperative day 8. At 18 months postoperatively, the patient underwent a myomectomy by laparoscopy. There were no significant adhesions or defects in the cornual area of the previous operation.
Appearance of the uterus after cornual resection.
Discussion
Interstitial ectopic pregnancies develop in the proximal and intramural part of the fallopian tube, laterally to the round ligament. 2 Natural course can lead to hemorrhagic rupture of the uterus (20% beyond 12 weeks of amenorrhea), which explains the excess mortality (relative risk × 2) compared with classical ampullary ectopic pregnancies. 3 Although alternative medical management has recently been proposed, it is not yet codified: one or more injections of methotrexate by the systemic or local route, sometimes associated with KCl, with success rates ranging between 35% and 87%.4,5
The “gold standard” of treatment is still surgery, consisting of cornual resection, or hysterectomy, according to the hemodynamic conditions. 6 Alongside the classical laparotomy route, the laparoscopic approach has been developed, and its efficacy for ampullary ectopic pregnancies management is unchallenged. The main problem of interstitial pregnancy management is controlling bleeding, which requires efficient coagulation of the uterine horn. In some cases, a conservative treatment by salpingotomy and aspiration of the interstitial pregnancy is feasible and sufficient for an early pregnancy of low volume. In other cases, and in particular when the diameter of the gestational sac exceeds 40 mm, salpingectomy with cornual resection is necessary. 7 To ensure efficient coagulation of the uterine horn, some have advocated biological glue, 8 endoloop ligature, 9 an encircling suture, 10 wire sutures, or automatic staplers. 11 The advantage of the endoloop lies in its simplicity, efficacy, rapidity, and low cost. Once the tube is pediculized by the retrograde route, the installation of the endoloop flush with the uterine horn is simple and ensures efficient hemostasis by the pull on the wire.
The largest series described in the literature 9 comprised 15 cases of nonruptured interstitial pregnancies and 3 ruptured cases, all successfully treated by laparoscopic endoloop ligature except for 1 case that needed additional methotrexate treatment.
For a surgeon trained in laparoscopy, the endoloop ligature technique is a safe and effective approach to the endoscopic management of interstitial pregnancies.
Footnotes
Disclosure Statement
No competing financial interests exist.