
Abstract
Abstract
Introduction
Uterine ischemia with subsequent necrosis and infection has been reported, requiring immediate resolution with little or no prior experience. 2 The diagnosis is difficult and often made during surgery. The authors report their experience and review the literature.
Case Report
A 68-year-old white woman, gravida 10, para 7, abortion 3, postmenopausal since age of 50, without prior gynecological surveillance, reported to the emergency room for postmenopausal bleeding, which she had been experiencing intermittently for the past 3 years. She denied abdominal pain. Her medical history was otherwise unremarkable. During examination, a red smooth-surfaced mass, approximately 10 cm, was filling her vagina. Hemoglobin level was 13.4 g/dL. Blood biochemistry was normal. She was admitted in order to further study and to schedule surgery. Hours later she developed low abdominal pain, fever (38.6°C) and the mass, now turned necrotic, protruded from the vulva. Immediate surgery was decided. At surgery, the patient was placed in lithotomy position to facilitate an abdominal and vaginal approach. The mass was removed by twisting through the vaginal route. At laparotomy, a doughnut appearance of an inverted uterus with tubes and ovaries abnormally positioned within the crater was observed. Pressure from below and bilateral traction on the round ligaments (Huntington procedure) failed, whereas an incision through the full thickness of the posterior uterine wall at the constriction site ring level combined with traction from below (Haultain procedure) successfully restored the uterus to normal position. Subsequently a total hysterectomy with bilateral adnexectomy was performed without difficulties. The postoperative course was uneventful and she was discharged on postoperative day 4. Histological study of the mass revealed an endometrial polyp; large areas of necrotic and hemorrhagic abnormalities due to ischemia were observed, but well-preserved endometrial glands without cytologic or architectural atypia were identified.
Discussion
Nonpuerperal uterine inversion is a rare condition. A review of English literature from 1940 to October 2000 by Takano et al. found 88 cases: 6.8% were caused by endometrial carcinoma, 71.6% by leiomyomas, 13.6% by sarcomas, and 8.0% were idiopathic.1,3 A MEDLINE® search using the term “uterine inversion” in conjunction with limits for “review and case report articles” found 142 cases: 59.1% were associated with leiomyomas, 25.3% with sarcomas, and 9.2% with endometrial carcinoma. The results are summarized in Table 1.4–35
Cited by Uludag. 7
Cited by Gowri. 35
Cited by da Silva. 17
Cited by Buyukkurt. 19
Of the total 142 reported cases, only 1 presented evidence of endometrial polyps alone (Table 2). 1
The inversion mechanism of uterine inversion is not clearly defined, but several factors may contribute: the thinning of the uterine walls due to the intrauterine tumor, rapid growth of the tumor, large tumor, fundic localization of the tumor, tumor attachment to the uterine wall with a thin pedicle, dilatation of the cervix by distension of the uterine cavity, and sudden emptying of the uterus previously distended from a tumor (Fig. 1).1,19
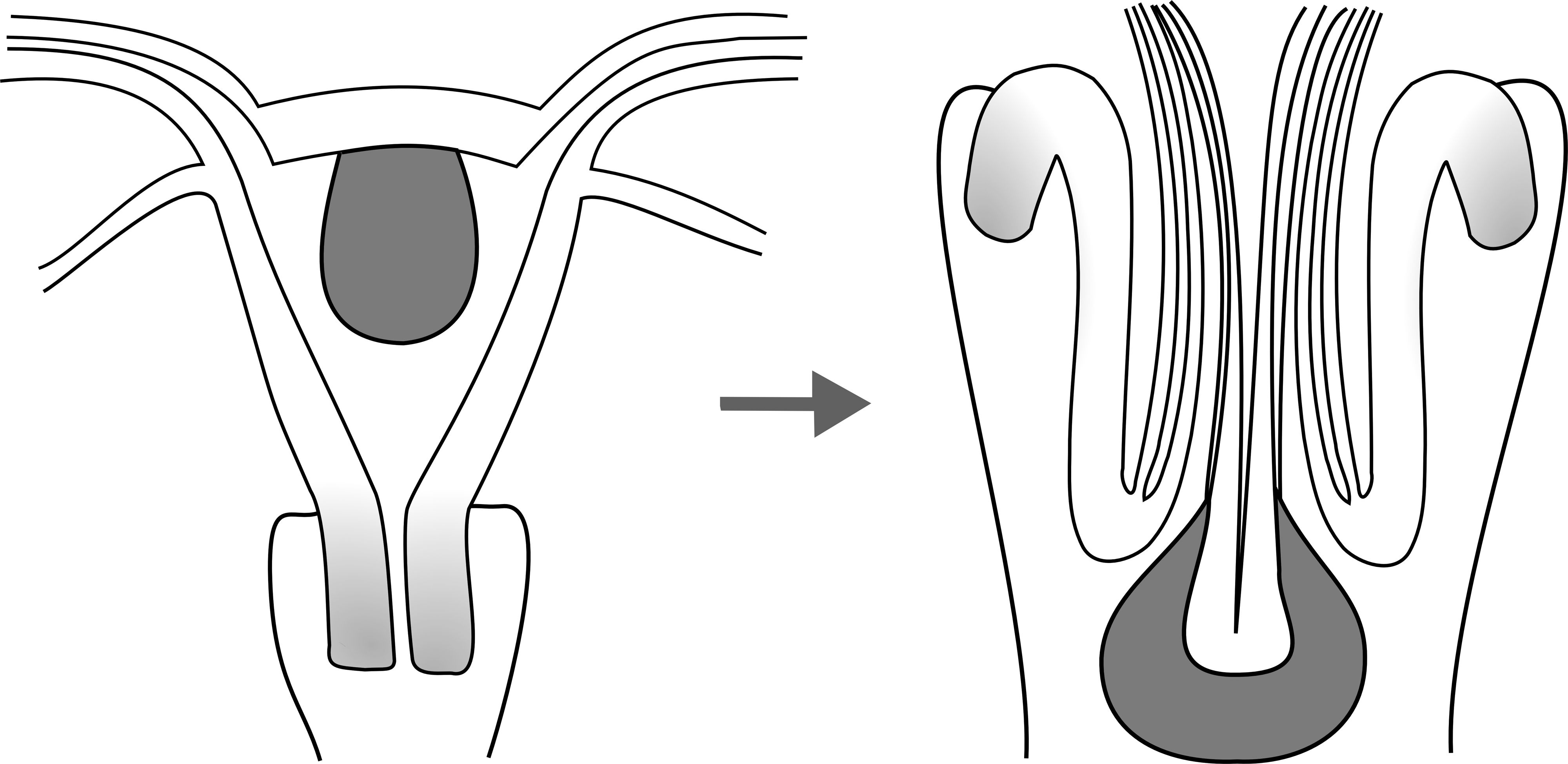
Diagram representing uterine inversion mechanism.
The diagnosis of uterine inversion is difficult and often made during surgery; patients can present with painful vaginal bleeding, shock, lower abdominal pain or pressure, bowel or bladder difficulties, weakness, and fatigue. 1 Lascaraides et al. proposed two diagnostic criteria: inability to palpate the uterine corpus on bimanual examination and nonvisualization of the cervix after excision of the vaginal mass. 3 Ultrasonography and magnetic resonance imaging have been shown useful as diagnostic tools.1,3 Lewin and Bryan reported that a U-shaped uterine cavity and a thickened and inverted fundus on a T2-weighted image in a sagittal magnetic resonance imaging are indicative of uterine inversion. 36
Five (5) surgical approaches have been described: two vaginal and three abdominal. The Kustner and Spinelli procedures are performed vaginally. The Kustner procedure involves entering the space of Douglas through a posterior colpotomy and a vertical incision in the posterior uterine wall is performed. Upward pressure restores anatomic position and subsequent suturing of the uterine incision or vaginal hysterectomy may be performed. The Spinelli procedure is similar but the uterine incision is performed in the anterior uterine wall after upward dissection of the bladder. 1 Tjalma and Huntington procedures are performed through an abdominal route without incision of the uterus, favoring these options in oncological surgery. 19 The Huntington procedure consists of grasping the round ligaments and uterus below the area of inversion and pulling upward until the uterus is reverted; this technique is unsuccessful in most cases due to a strong constriction ring. 19 In the Tjalma method, the retroperitoneal spaces are opened after securing the round and infundibulopelvic ligaments; both ureters are dissected and the uterine arteries are selectively tied. The anterior wall of the vagina is opened and the incision is continued circumferentially, with clamping of the parametrial and uterosacral ligaments; the removal of the inverted uterus follows. 37 The Haultain procedure, chosen in this case, consists of incising the posterior uterine wall in order to reposition the inverted uterus. 19 The Haultain operation is easy and surgically safe. Some expertise is required for the Tjalma method.
At admission, the patient complained of vaginal spotting and shortly thereafter protrusion of the mass occurred with subsequent uterine inversion and infection. Prompt surgical intervention favorably contributed to the outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.