
Abstract
Abstract
Introduction
Case Report
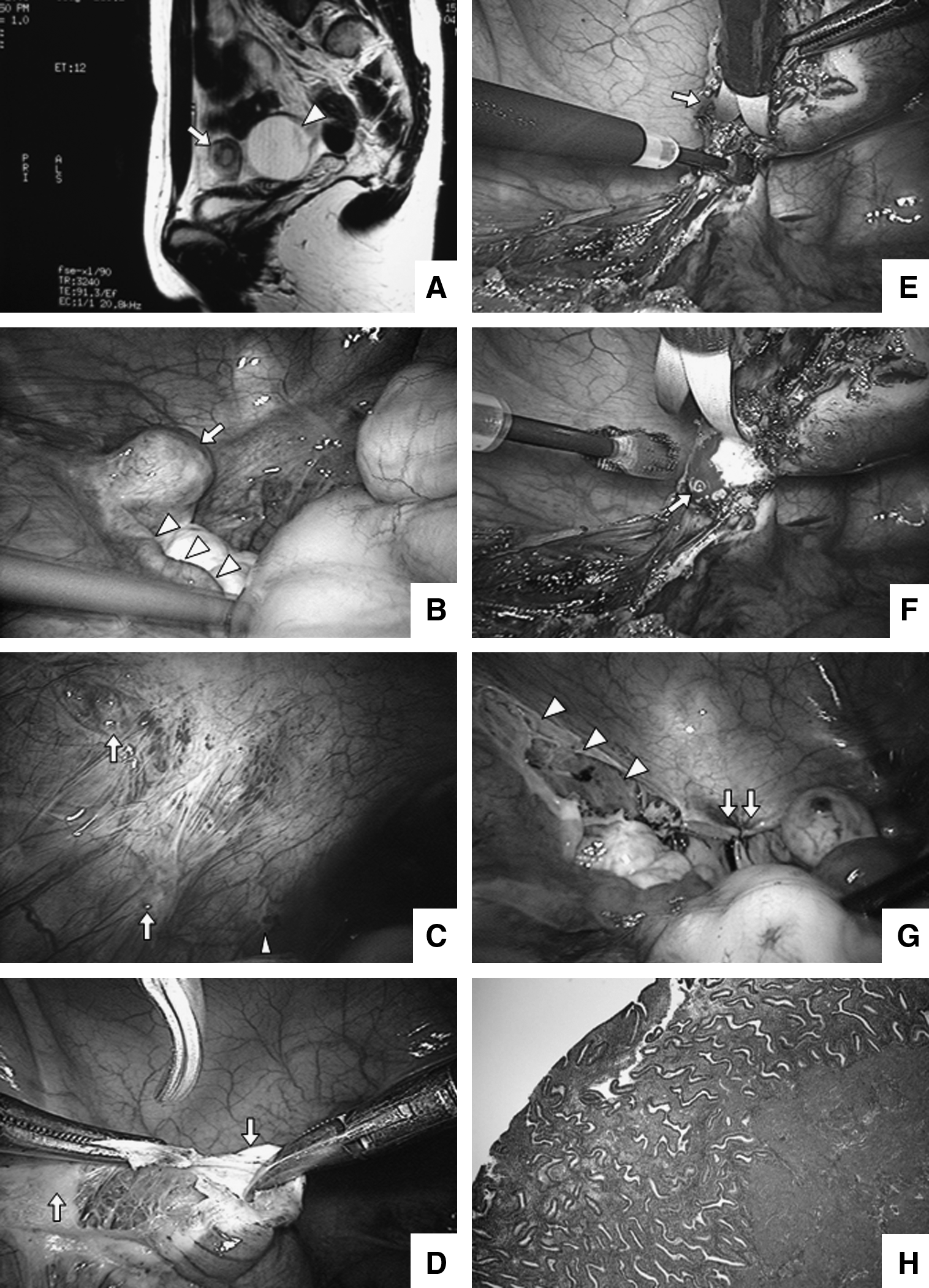
The patient is a 22-year-old Japanese woman with a nonsignificant family medical history. She was born prematurely at 28 weeks with a birth weight of 1500 g. When the patient was 19 years old, she first consulted our institution for primary amenorrhea and monthly severe left-sided pain. Her breasts and external genitalia were normally developed, and she had normal axillary and pubic hair. On gynecological examination, no vagina was detected but a small dent partially surrounded by trace of hymenal ring was detected. On rectal examination, no uterus could be palpated. Magnetic resonance imaging (MRI) revealed that bilateral normal ovaries and rudimentary uterine horns were found in the pelvic cavity. There was a 1-cm high-intensity region in the left rudimentary horn on T2-weighted MRI (Fig. 1A). Bilateral kidneys were detected. On follow-up at age 22, the patient expressed her desire for vaginal plastic surgery/vaginoplasty. At this time, the patient continued to experience left-sided pain monthly, thus heightening the suspicion of functional endometrium within the rudimentary uterus. From these findings, concurrent performance of laparoscopic removal of the left rudimentary uterus and laparoscopic-assisted colpopoiesis with the modified Davydov's procedure were planned.
Magnetic resonance (MRI) images, (
Operation
Measures to prevent ureteric injury were taken also; these included preoperative ureteral stent placement and intraoperative confirmation of ureteral position using forceps. Three (3) trocars were inserted at the subumbilical, bilateral iliac midclavicular positions. Bilateral rudimentary uteri were observed in both right and left sides of the pelvic cavity. The left rudimentary uterine horn was measured to be 2.5 cm × 2.0 cm × 1.8 cm. The right rudimentary uterine horn was clearly smaller than the left, and bilateral normal adnexae were detected (Fig. 1B). There was no evidence of adhesions in the pelvic cavity. Peritoneal endometriosis (clear lesion and blueberry spot: Fig. 1C) was detected on the left pelvic cavity (Fig. 1C), and then vaporized. For removal of the left rudimentary uterus, coagulotomy of the left round ligament was performed, and the retroperitoneal space was expanded (Fig. 1D).
The left ovarian ligament and fallopian tube were isolated, and parametrial tissue was dissected as in routine hysterectomy (Fig. 1E). The ascending branch of the left uterine artery was present in the adjacent parametrial tissue, and coagulotomy was performed (Fig. 1F). Caudal expansion was subsequently done with precaution to avoid any bladder injuries. The left rudimentary uterus was externalized through the neovagina during vaginoplasty. Colpopoiesis by the modified Davydov's procedure was performed sequentially. Metreurynter (Fiji Latex Co., Ltd., Tokyo Japan), a balloon catheter, was inserted into the neovagina. The balloon component was inflated with 250 mL saline to dilate the vaginal cavity and then removed. 1 The most dependent deep cul-de-sac peritoneum was pulled down to the vaginal canal and fixed to the entrance of the vaginal canal, and a vault was made by laparoscopic suturing. An acrylic mold was inserted into the neovagina. 2 The peritoneal deficiency after rudimentary uterus resection did not preclude peritoneal suturing (Fig. 1G). The patient was discharged on postoperative day 6. Histological examination of the resected left rudimentary uterus revealed the presence of endometrium within the cavity of the specimen (Fig. 1H). The postoperative course was favorable with no signs of stenosis of the neovaginal cavity after 1 month.
Discussion
When endometrial presence is suspected in the rudimentary uterus of a patient with MRKH, careful diagnosis and treatment are necessary. According to a report by Fedele et al., 9 of 24 patients are estimated to have functional endometrium present in their rudimentary uterus by MRI imaging. 3 In these cases, there may be typical clinical manifestations of obstruction (i.e., cyclic pain from hematometra). In selected cases, it may be possible to anastamose the cavity of the rudimentary horn to the vaginal vestibulum to allow cyclic menstruation. 4 Indiscriminant removal of the uterine horns in all patients may damage the ovarian vascular supply. 3 Other authors have reported laparoscopic removal of the rudimentary uterus in women with MRKH who have reported symptoms of monthly recurrent pain. 5 In our case, the patient complained of left pelvic pain once a month, and subsequently an association between the pain and the presence of the functional endometrium in the rudimentary uterus was suspected. Moreover, because the patient was desirous of removal of the left rudimentary uterus, an optimal resection procedure was planned. By ligating adjacent ligaments, the rudimentary uterus was exposed and was resected relatively easily.
It was possible to remove the rudimentary uterus by anatomical recognition in a procedure similar to a normal hysterectomy. 6 Externalization of the rudimentary uterus via the neovagina during colpopoiesis was possible. There was concern that the peritoneum would have limited stretchability for vaginoplasty because of peritoneal deficiency after rudimentary uterus extraction. An initial concern was that resection of the rudimentary uterus and peritoneum would compromise our ability to stretch the peritoneum for the vaginoplasty. This did not prove to be an issue. Finally, the presence of peritoneal endometriosis was significant. Although there was a functional endometrium present, a connection between the left uterine cavity and fallopian tube could not be identified by dissection. It was also noted that there was no hematometra.
Conclusions
Thus, whether endometriosis originated through retrograde flow through the fallopian tubes or through metaplasia has yet to be determined.
Footnotes
Acknowledgments
We are grateful to Professor Tasuku Harada, Tottori University, Japan for support based on his clinical experience. We also thank Dr. Clarissa Velayo and Mr. Hisataka Hasegawa for the preparation of the manuscript.
Disclosure Statement
All authors do not have a commercial interest, financial interest, or other relationship with manufacturers of pharmaceuticals, laboratory supplies, and medical devices or with commercial providers of medically related services.