
Abstract
Abstract
Introduction
Although the tendency is to avoid surgical interventions in women during pregnancy, the major challenge is when these women present with acute abdomen, making immediate intervention inevitable. Such cases are most often the result of acute intra-abdominal inflammatory processes, most often, acute appendicitis, cholecystitis, or pancreatitis; or noninflammatory processes, such as adnexal masses, torsion, and intestinal obstruction. 2 The most common cause of acute abdomen in pregnant women is acute appendicitis, occurring with an average rate of 0.0018%, followed by gallbladder disease with a frequency from 0.05% to 0.3%.3,4
In such cases, close cooperation among the gynecologist, surgeon, and anaesthetist is the key to minimizing operative risk and ensuring the best possible result for both mother and her fetus.
The need for minimally invasive techniques in such cases is evident. Laparoscopic procedures seem to cover this need for minimizing surgical trauma, which is considered a major risk factor in these cases. Despite this, there is still some concern regarding the use of general anesthesia and some other specific features of laparoscopic surgery, such as the need for increased intra-abdominal pressure, insuflation of CO2, and technical difficulties caused by the presence of the pregnant uterus. 5
The aim of this article is to present experience, during the last 5 years, with treating 5 pregnant women with acute abdomen who had laparoscopic procedures.
Materials and Methods
During a period of 5 years, from 2002 to 2007, 5 pregnant women with acute abdomen were treated. The patients were 26–33 years old and had all completed the second trimester of gestation at when they were operated on. Three (3) patients presented symptoms involving the right lower quadrant of the abdomen. Intraoperatively, 2 patients were seen to have acute appendicitis and were subjected to laparoscopic appendectomy, and 1 patient, who had undergone in-vitro fertilization (IVF), was found to have a torsion of an enlarged right ovary, which was reduced laparoscopically. The remaining 2 patients presented with signs and symptoms of acute cholecystitis and were subjected to laparoscopic cholecystectomy. All patients were investigated preoperatively with ultrasonographic imaging, and the correct diagnosis was determined in 4 of the 5 patients. In the patient with the twisted ovary, the appendix was not visualised in the sonogram.
In the operating room, all of the women were positioned in a slightly leftward lateral position and pneumoperitoneum was induced via the open (Hasson) technique, aided by ultrasonographic guidance to identify the height of the uterus (Fig. 1). Intra-abdominal pressure was kept below 12 mmHg in all patients. Trocar placing was not standard as it would be for a nonpregnancy case, as the location of the first port was moved 3–4 cm above the umbilicus to avoid injury to the enlarged uterus (Fig. 2). The mean duration of the operation was 50 minutes for the cholecystectomy patients, 43 minutes for the appendectomy patients, and 40 minutes for the patient who required removal of her twisted ovary (Table 1).

Schematic diagram of uterine fundal height on the basis of gestational age in weeks.
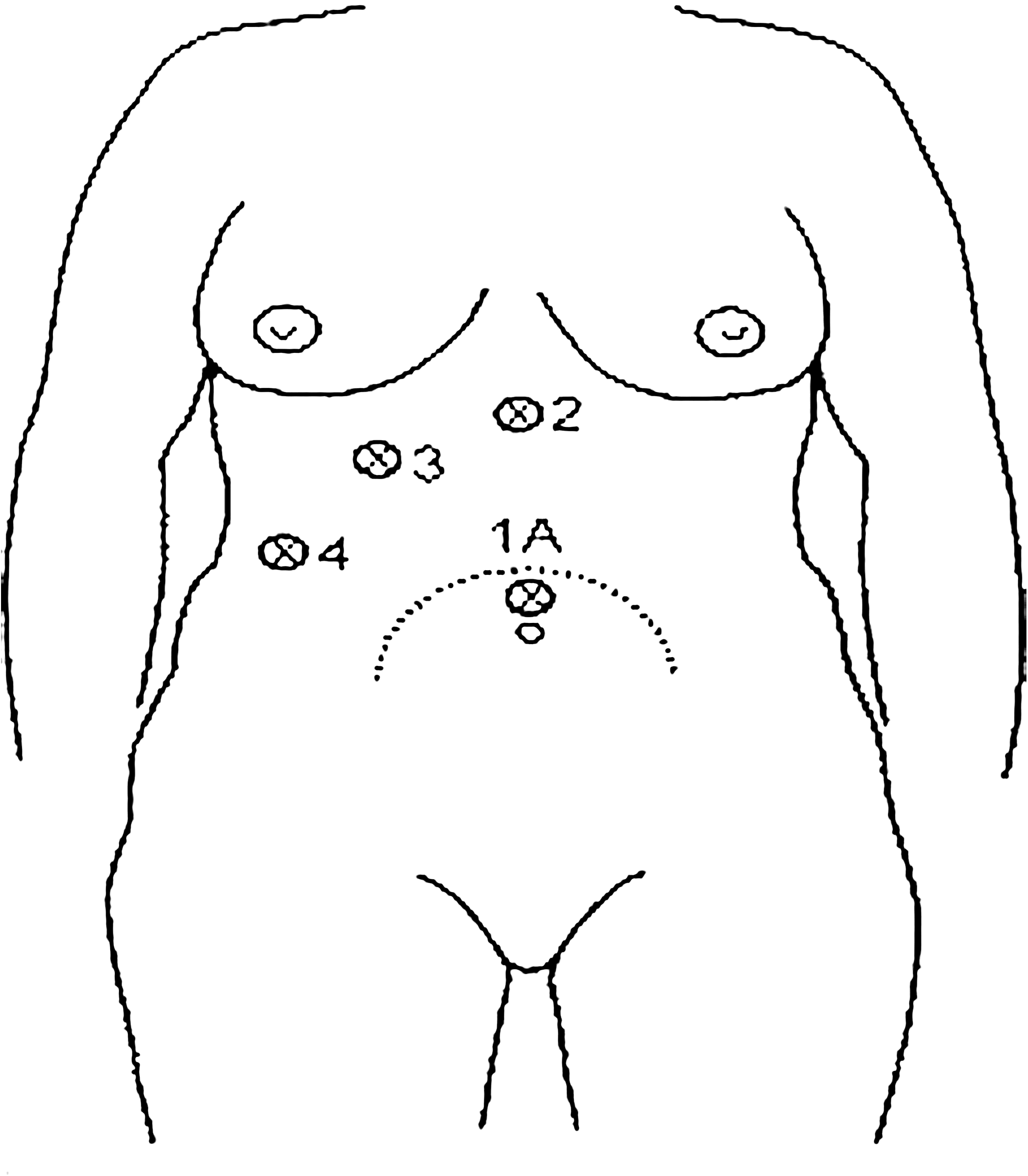
Schematic representation of trocar positioning for the laparoscopic approach of a pregnant patient during second trimester. Supraumbilical positioning of laparoscope may be required to permit clear visualization.
Results
All patients recovered in the operating room and were discharged from the hospital after a mean stay of 1.5 days. No major or minor postoperative complications of the mothers or fetuses were observed. All women gave birth to normal neonates in term with the exception of 1 of the cholecystectomy patients who gave birth 20 days preterm.
Discussion
Acute abdominal emergencies in pregnant women are one of the most puzzling medical problems from both diagnostic and therapeutic aspects. A patient with symptoms and signs that set the diagnosis of acute abdomen is invariably a surgical patient. This is also true in the pregnant patient with acute abdomen but, in these cases, diagnosis is obscured and intervention delayed by the enlarged uterus, which does not permit accurate clinical evaluation; by the maternal physiology that involves alterations in hematologic and biochemical measurements; and by the presence of symptoms, such as nausea and vomiting, that apply to pregnancy and to a number of pathologic disorders. An added factor in delaying the intervention in such cases is the reluctance of many surgeons to lead a pregnant woman promptly to the operating theatre. 6 However, it is usually not the treatment but the delay in diagnosis and severity of the primary disease process that affect outcomes negatively. 7
The need for prompt surgical intervention indicated becomes tragically obvious if one considers the complication rates. The risk of fetal death in a pregnant woman with acute appendicitis without perforation is 1.5%, but, if perforation occurs, the risk climbs to a staggering 35%. 8 Preterm labor and premature delivery rates are as high as 40% in perforated appendicitis, 9 compared with a 13% rate of preterm labor and 4% rate of premature delivery in acute appendicitis. 10 Similarly, gallbladder disease is accompanied with a fetal mortality of 3%–5%, but if pancreatitis occurs the fetal death rate is more than 60%.11,12
The use of laparoscopic surgery in acute abdominal operations in pregnant women has many established advantages, but also comes with some concerns. Laparoscopic surgery as a minimally invasive technique has the advantages of early patient ambulation; decreased risk for thromboembolism, which is higher in pregnancy; decreased postoperative pain, minimized need for analgesics; shorter hospital stay; and better cosmetic results. 13
Despite all the advantages, use of laparoscopy in pregnancy is accompanied by skepticism mainly because of the technique itself and the presence of an enlarged uterus. Factors of major concern are increased intra-abdominal pressure during the operation; use of CO2; and possible adverse effects these factors may have on uteroplacental blood flow for the former and of absorption for the latter. These disadvantages can be counterbalanced by keeping the intra-abdominal pressure well below 12 mm Hg and by shortening the time of the operation reducing exposure of the fetus to CO2. 14
Moreover, preoperative ultrasonographic image showing the height of uterus combined with use of the open technique for the first trocar instead of the Veress needle avoids injury to the enlarged uterus. To date, there is no definitive link between laparoscopic surgery and complications for the course of the pregnancy and fetal development.15,16
In the current small series of operations, no adverse effects were observed in all cases except the occurrence of preterm delivery in 1 woman, which cannot be linked causatively to the operation itself.
Conclusions
Early intervention in acute abdominal emergencies in pregnancy can prove lifesaving for the fetus and for mother is undisputed, and, use of minimally invasive techniques is proving to be as safe as it is in all other cases, providing significant advantages for patient mobilization, length of stay, postoperative pain, and cosmetic concerns. All the above leads to the conclusion that laparoscopic surgery is safe and effective if used prudently in pregnant patients although it still has to face the test of time.
Footnotes
Disclosure Statement
No competing financial conflicts exist.