
Abstract
Abstract
Introduction
Similar to other abdominal operations, cesarean delivery is associated with intra-abdominal adhesions. Consequently, the wider use of cesarean deliveries has made obstetricians more aware of the importance of adhesions after cesarean deliveries. This includes difficulty entering the abdominal cavity (leading to longer time to deliver the baby), increased blood loss, increased risk of uterine and bladder trauma, as well as longer operating time for repeated cesareans.
The purpose of this review is to evaluate the occurrence and clinical relevance of adhesions after cesarean delivery and their implications, as well discussing options for reducing adhesion formation.
Pathophysiology of Adhesion Formation
The peritoneum, a highly vascularized surface layer of mesothelial cells, protects abdominal structures and reduces friction among them. 4 Postoperative peritoneal adhesions result from surgical tissue trauma and the ensuing healing process. 5 Potential causative agents of tissue trauma include injuries (sharp, mechanical, or thermal), infection, ischemia, radiation, desiccation, abrasion, and reactions to foreign bodies (e.g., reactive sutures or tissue char from fulguration). Peritoneal tissue trauma disrupts stromal cells, leading to release of substances that increase vascular permeability and triggering a cascade of inflammatory processes that stimulate mesothelial cell migration to the site of injury.4–6 These events lead to formation of a new mesothelial layer, with accompanying fibrin deposition that often connects adjacent tissues. Adhesions form when two raw peritoneal surfaces are brought together as a consequence of this injury-repair mechanism.
The location and type of surgical incision affect adhesion-formation tendency. Brill and colleagues 7 documented a 27% incidence of adhesions to the omentum and bowel via Pfannenstiel entry, a 55% incidence of adhesions with a midline supraumbilical incision, and a 67% incidence of adhesions with a midline infraumbilical incision. The distribution (omentum alone or omentum and bowel) and severity of adhesions also varied with the type of incision made. In the Pfannenstiel group, 87% had adhesions to the omentum, and 13% had adhesions to the bowel and omentum. In the midline infraumbilical group, 83% had omental adhesions, and 17% had adhesions to the bowel and omentum; and, in the midline supraumbilical group, 60% had omental adhesions, and 40% had adhesions to the bowel/omentum. 7 In addition, it is well-documented that the presence of sepsis and/or peritonitis augments adhesion formation by suppressing the fibrinolytic cascade.8,9 Evidence from rat models shows an increase incidence in abdominal-pelvic adhesions with peritoneal closure in the presence of bacterial colonization/inoculum as compared to nonperitoneal closure. 9 However, it is unclear if the choice of suture material chosen in that study affected adhesion formation as an uncontrolled variable. Unlike the differences in skin keloid formation based on race, race does not seem to influence the formation of peritoneal adhesions. 10 Another factor known to influence adhesiogenesis is the choice of suture material used to close the abdominal wall/peritoneum. In a rat adhesion model, suture material, volume, and diameter were evaluated for type and severity of adhesion formation. 11 Prolene produced a smaller mean adhesion percentage compared to use of Vicryl and Chromic closures. 12 Chromic sutures caused the most extensive and severe of all of the suture subtypes in the study.
When considering adhesions as an obstetric problem, it is important to note that a gravid uterus is larger and more vascular than a nongravid uterus, and that the process of healing following a cesarean section may be different from that following a myomectomy or other type of gynecologic surgery.
The above discussion outlined the complexities and covariables intricately involved to influence the pathogenesis of peritoneal adhesions. Therefore, a “global” perspective of prevention must factor into account all of the nuances of this pathologic entity if any preventive platform is to be successful.
Incidence of Postcesarean Adhesions
Despite the use of good surgical techniques, adhesions form in most women who undergo gynecologic pelvic surgery. Even though cesarean deliveries are performed much more frequently than hysterectomies, the rate of adhesion following primary or repeat cesarean deliveries is less well-documented. However, cesarean deliveries are inherently shorter procedures, involve more fluids, and are immunologically very different than other gynecologic pelvic surgeries. These factors are important considerations when differentiating gynecologic from obstetric surgery. Before the recent publication of a few retrospective studies, awareness of the impact of postcesarean adhesions came from anecdotal and personal experience. In a 2007 retrospective cohort analysis, Morales and colleagues reported that 4% of women had documented adhesions at primary cesarean section, and 46% had adhesions at the time of their second cesarean delivery (Fig. 1). 13 More than half of the adhesions were considered severe, and adhesions with anterior abdominal involvement were noted in 77% of women with repeat cesarean deliveries. The development of dense adhesions is a common occurrence among women who have undergone many cesarean deliveries, 14 and the extent of adhesions is directly related to the number of cesarean deliveries.15,16 In a retrospective study of 371 patients with a history of repeat cesarean section, Sobande and Eskandar found that having undergone 3 or more cesarean deliveries was associated with a higher prevalence of dense intra-abdominal adhesions and bladder injury, compared with a single cesarean section. 17 In a prospective cohort study, Lyell and coworkers reported that 63% of women undergoing a repeat cesarean delivery had “dense and filmy” adhesions. 18 In an observational chart review of 191 patients who had undergone repeat cesareans, Myers and colleagues observed that 6% of patients who had closure of the visceral and parietal peritoneum had severe (Grade 3 or 4) adhesions, compared with 42% of patients who did not undergo peritoneal closure (p = 0.003). 10
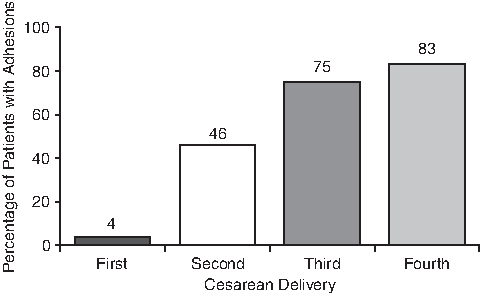
Incidence of adhesions following cesarean delivery in 542 women increased in parallel with number of previous cesarean deliveries. 13
Consequences of Postcesarean Adhesions
Adhesions may cause abdominal pain, infertility, or bowel obstruction.19,20 In addition, patients may need to undergo repeat surgery, with the potential for associated surgical complications. 5 The presence of dense adhesions can create technical difficulties for surgeons during repeat cesarean deliveries that often lead to prolongation of these operations, and that may increase the risk of injury to adjacent organs. 14 In addition to the consistency of the adhesions, their location is important. For example, while adhesions between the omentum and the liver have little clinical significance, adhesions that may prolong delivery time are clinically meaningful for the mother as well as the fetus. Another obstetrical consideration is the presence of adhesions between the uterus and bladder. This is related to the conventional incision in the thin lower uterine segment to reduce blood loss. Dense adhesions covering this area make it difficult to expose the surgical field, delaying surgery and, consequently, delaying delivery of the neonate. In addition, the presence of adhesions is associated with an increased risk of bladder injury during cesareans (p = 0.0006), as reported in a recently published retrospective review. 21 Results of a case-control study of women undergoing cesarean delivery also suggested that adhesions from previous cesarean sections increase the risk of bladder injury during a subsequent cesarean delivery. 22 These examples illustrate the increased importance of adhesions in obstetrics that are unique to this procedure.
Prevention of Adhesions
The main strategies used to decrease and prevent adhesion formation include: (1) decreasing peritoneal trauma utilizing gentle surgical techniques; (2) modifying the fibrin formation and degradation balance; and (3) using physical barriers to prevent organs from attaching to other abdominal structures. 6 In addition to being effective, an adhesion-reducing substance should be nontoxic, easy to apply, and biodegradable. Also, it should not interfere with healing and immune response. 6
Closure of the parietal peritoneum during cesarean section has been a matter of debate for many years, with the favored practice changing in cycles. A 2003 Cochrane analysis of 14 controlled studies concluded that, compared with suturing the peritoneum, nonclosure of the peritoneum is associated with reduced cesarean operating time, decreased postoperative fever, reduced postoperative hospital stay, and decreased number of postoperative analgesic doses. 23 However, inadequate data were available to determine the potential long-term risks and benefits of peritoneal nonclosure on adhesion formation. In a randomized study comparing nonclosure versus closure of the parietal peritoneum during cesarean section, long-term patient follow-up revealed similar long-term morbidities, including infertility, abdominal pain, and urinary symptoms. 24 Unfortunately, data on adhesions were available for only 20 of the 280 women recruited in the original study, 25 making it difficult to draw any conclusions.
The concept that closure of the parietal or visceral peritoneum is unnecessary was based on the results of trials suggesting more adhesion formation following peritoneal closure, and this practice is associated with longer operating time and more post-operative pain. 26 For example, in a retrospective chart review of 100 patients who had undergone 2 cesarean deliveries, the researchers reported that adhesions were found in 28% of patients with peritoneal closure and in 14% of those without peritoneal closure. 27 While operating time was longer in the group with peritoneal closure, the incidence of postoperative urinary-tract infections, endometritis, wound infection, and respiratory-tract infections were similar in both groups. Komoto and coworkers found no difference in postoperative complications after a first cesarean delivery but did find a significantly higher incidence of adhesions in women who had closure of the peritoneum than in those without peritoneal closure. 28 In a randomized study of 360 women undergoing their first cesarean delivery (and including 65 women who had a second cesarean), Weerawetwat and colleagues reported that, while postoperative complications and number of adhesions were similar in nonclosure and closure groups, the adhesions appeared to be more severe in the closure group. 29 Another randomized study involving 600 women showed that, compared with a what was seen in a peritoneal-closure group, nonclosure of the peritoneum was associated with shorter operative time, shorter time to ambulation and oral intake, shorter hospital stay, and less adhesion formation. 30 Based on these results, many surgeons discontinued the practice of closing the peritoneum during cesarean delivery.
In contrast, several retrospective chart-review studies, a prospective, nonrandomized case series, and another prospective randomized study demonstrated that peritoneal closure reduced the risk of adhesion formation, calling nonclosure of the peritoneum into question. More specifically, in Lyell and coworkers' prospectively scored, nonrandomized series of 173 patients undergoing a first repeat cesarean delivery, patients with prior parietal peritoneal closure had fewer dense and filmy adhesions compared with patients whose peritoneum was left open (52% versus 73%, p = 0.006). 18 Similarly, in a retrospective chart review of a smaller cohort of patients, Myers and colleagues found adhesions in significantly fewer patients with prior peritoneal closure, compared with those with no prior peritoneal closure (6% versus 42%, respectively; p = 0.003). 31 Another retrospective study of 62 cases of repeat cesarean sections found that fewer patients with peritoneal closures had adhesions compared with patients with nonclosure (31% versus 70%; p = 0.013). 32 The results of these studies are summarized in Table 1.
In a prospective randomized study of nonclosure versus closure of the peritoneum during cesarean section, severe adhesions were diagnosed in 54% of patients with nonclosure, compared with 15% in patients with closure (relative risk, 3.2; 95% confidence interval [CI] 1.0 −10.2). 33 While this study suggested that peritoneal closure may reduce the risk of adhesion, statistical interpretation of the results is limited by the small sample size (45 patients), as demonstrated by the wide CI.
These recent data and increased awareness of the uniqueness of cesarean sections relative to other gynecologic surgeries have swung the pendulum back to a preference for peritoneal closure. A key distinction is that, while in gynecologic surgeries it is rare that incisions are repeatedly made in the same region, women often undergo repeat cesareans within a period of a few years. The need to reenter the previous incision line with repeated cesarean deliveries underscores the importance of preventing or reducing adhesion formation. The size of the postcesarean uterus and its contact with the fascial suture closure may predispose a patient to adhesion formation. In addition, the enhanced vascularity of the gravid uterus often leads to “oozing” of blood from damaged surfaces after uterine closure leading to fibrin deposition and adhesion formation. Other factors that may predispose a patient to adhesions with cesarean delivery include the presence of meconium (which can cause chemical peritonitis), fetal hair, tissues, and fats, and placental debris. Compared with minimally invasive surgery for gynecologic procedures, cesarean delivery requires a laparotomy and considerable manipulation not only of the uterine surface and the uterus itself, but also of the adjacent tissue such as the small bowel and bladder.
Adhesion-Reducing Substances
Currently available adhesion-reducing substances, including peritoneal instillates, and surgical-adhesion barriers have not been rigorously studied relative to cesarean delivery. 5
A 2008 Cochrane review evaluated randomized controlled trials of surgical barriers for adhesion prevention after gynecologic surgery. This review included 16 studies; 11 of these studies compared oxidized regenerated cellulose (INTERCEED®) with no treatment, two studies compared INTERCEED with the expanded polytetrafluoroethylene Gore-Tex surgical membrane (Preclude®), 1 study compared Preclude with no treatment, 1 study compared chemically modified sodium hyaluronate/carboxymethylcellulose (Seprafilm®) with no treatment, and another study compared a fibrin sheet with no treatment. 34 None of these studies evaluated pregnancy or pain reduction as the primary outcome. This review showed that the use of INTERCEED reduced the incidence of adhesion formation and reformation. In addition, Preclude appeared to be more effective than either no barrier or INTERCEED for preventing adhesion formation following myomectomy. However, the use of Preclude was limited because of the need for suturing to anchor the fabric to the tissue, the difficulty in handling it, and the possible need for its later removal because of its lack of absorbability. In a small retrospective study, INTERCEED use was associated with increased pregnancy rate. 35
It is difficult to extrapolate from these data what the possible efficacy and difficulties associated with the use of these substances in cesarean sections might be. Currently, there are only two small studies evaluating the effectiveness of adhesion barriers for preventing the formation of adhesions following cesarean section. Kim et al studied 45 patients who underwent a primary cesarean section in their institution and subsequently returned for a repeated cesarean delivery. 36 At the time of the primary cesarean section, the surgeons had applied INTERCEED on the vesicouterine fold in 8 patients, while an additional 37 patients did not receive INTERCEED. Adhesions were graded at the time of repeated cesarean delivery from Grade 0 (no adhesions) to Grade 3 (severe vesicouterine and peritoneal adhesions causing a difficult delivery). The researchers reported that all patients in the INTERCEED group had Grade 0 adhesions, whereas in the non-INTERCEED group, 30 patients had Grade 1 adhesions, 4 patients had Grade 2 adhesions, and 3 patients had Grade 3 adhesions (Table 2).
Adhesion scores were determined by two different methods for each of the above studies.
Fushiki and colleagues examined the efficacy of Seprafilm as an adhesion barrier in repeat caesarean delivery. 37 At the time of the first cesarean, Seprafilm was placed on the peritoneal sutures along the vesicouterine fold and vertically along the uterine serosa in 27 patients. When the incidence of adhesions was compared with that seen in 25 patients who did not receive Seprafilm, adhesions were found in 2 of the 27 patients (7.4%) in the Seprafilm group and in 12 of the 25 patients (48%) in the non-Seprafilm group (p = 0.001; Table 2). 37 Large prospective randomized studies with long-term follow-up will be needed to substantiate the conclusion that adhesion barriers reduce adhesion formation following cesarean sections.
Conclusions: Future Prospects
Adhesion prevention is a difficult area to study for many reasons, and research on the use of adhesion-reducing substances at cesarean delivery raises another set of barriers. For example, not all patients return to the same institution for repeat cesareans, and, to date, there are no standardized grading systems for severity of adhesions during a cesarean. Second-look laparoscopy is not always feasible, and one has to rely on subsequent cesarean procedures to assess adhesion formation. Understandably, not all patients will undergo repeat cesarean delivery. Despite the main objective of delivering a healthy baby, variability remains in the way cesarean sections are performed. For example, following the delivery of the neonate and placenta, some obstetricians suture the uterine incision while the uterus remains in the abdominal cavity, while other surgeons prefer to suture with the uterus outside the abdominal cavity. There is a need for well-designed, prospective, randomized studies to evaluate adhesion rates after cesarean deliveries performed with and without adhesion-reducing substances, and to assess their repercussions on subsequent deliveries as well as on general health.
Footnotes
Acknowledgments
Nancy Bella, PharmD, of MedErgy provided editorial assistance, which was funded by Ethicon.
Disclosure Statement
Dr. Chapa serves as a medical consultant for Ethicon Women's Health and Urology. He has received an investigator-initiated study grant from Johnson & Johnson's Medical Affairs department for the investigation of postcesarean section adhesions; study initiation was slated for early 2010. No financial incentive was given for the formulation of the material presented in this article.
Dr. Sbarra serves as a medical consultant for Ethicon Women's Health and Urology. No financial incentive was given for the formulation of this material presented in this article.