
Abstract
Abstract
Introduction
Case Report
A 30-year-old female was referred to the authors' institution with abdominal pain. On physical examination, no palpabe mass in the abdomen was discerned. Preoperative serum CA.125 was in the normal range. Ultrasonography showed an hypoechoic, heterogeneous, round mass adjacent to the lower extremity of the left ovary, measuring 4.5 cm in maximum diameter. A contrast-enhanced abdominal computed tomography (CT) revealed a round (6 cm maximum diameter) pelvic mass in the left side of the uterus, superiorly to the omolateral ovary (Fig. 1). The mass had heterogeneous content and well-defined margins and showed no enhancement after intravenous contrast dye was administered to the patient. Minimal fluid in the pelvis was recognizable. A laparoscopic resection of the mass was performed. Intraoperatively, an extraperitoneal, glistening pelvic mass was discovered: the lesion was attached to the intrapelvic one-third middle portion of the left round ligament (Fig. 2). Macroscopically, the mass measured 6 cm × 6 cm × 3.5 cm and had a smooth and glistening external surface. On cut section, the mass was shown to be an unilocular cyst filled with soft, yellow, amorphous material. Histologically, the wall of the cyst was lined by stratified squamous epithelium with a granular cell layer (Fig. 3). The cavity contained keratin material. Parietal rupture was present, accompanied by granulomatous inflammation (Fig. 4). The patient was well postoperatively and was discharged 3 days after her operation. At 20-month, follow-up the patient was healthy without any symptoms of a recurrent tumor.

Contrast-enhanced computed tomography scan of the pelvis showed a round (6 cm in maximum diameter; arrows) pelvic mass at the left side of the uterus, superiorly to the omolateral ovary with content heterogeneous content in the left side of the uterus with a large cavity (*), superiorly to the omolateral adnexa (arrow head). Minimal fluid in the pelvis was recognizable.
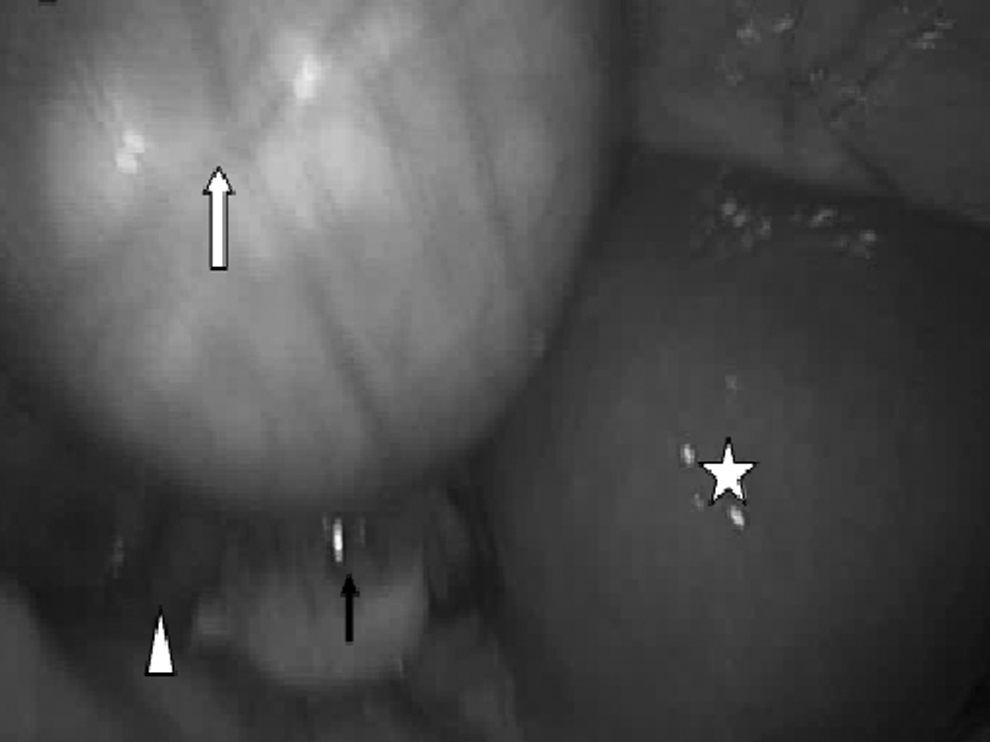
Intraoperatively, there was a 6 cm × 6 cm × 3 cm extraperitoneal pelvic mass attached to the intrapelvic one-third middle portion of the left round ligament, with a glistening and smooth surface. Key for symbols:⇑, cyst of round ligament; ⋆, uterine fundus; ↑, ovary; ▵, fallopian tube.
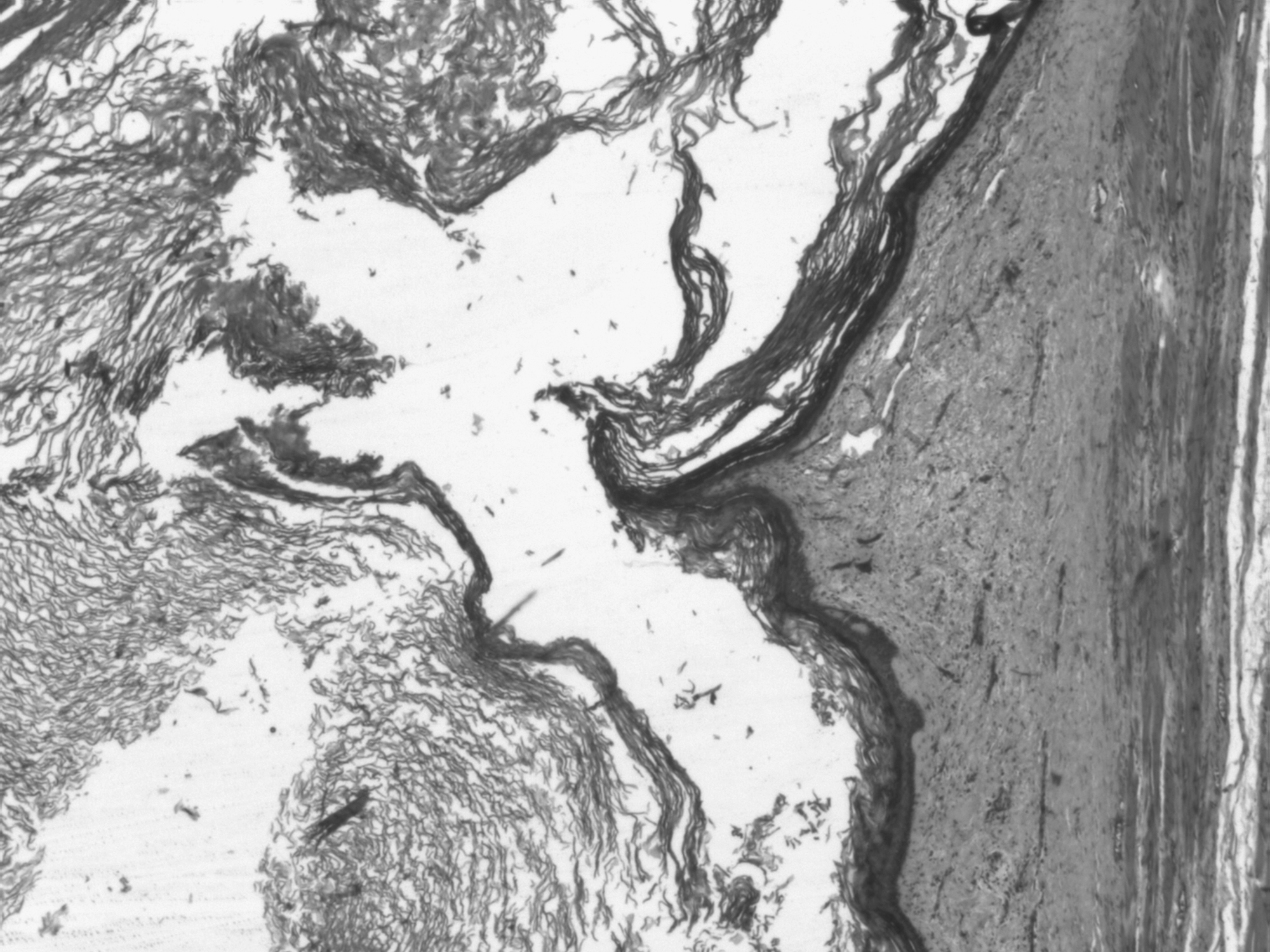
The wall of the cyst was lined by a stratified squamous epithelium with a granular cell layer. The cavity contained keratin material (H.E; 40 ×).
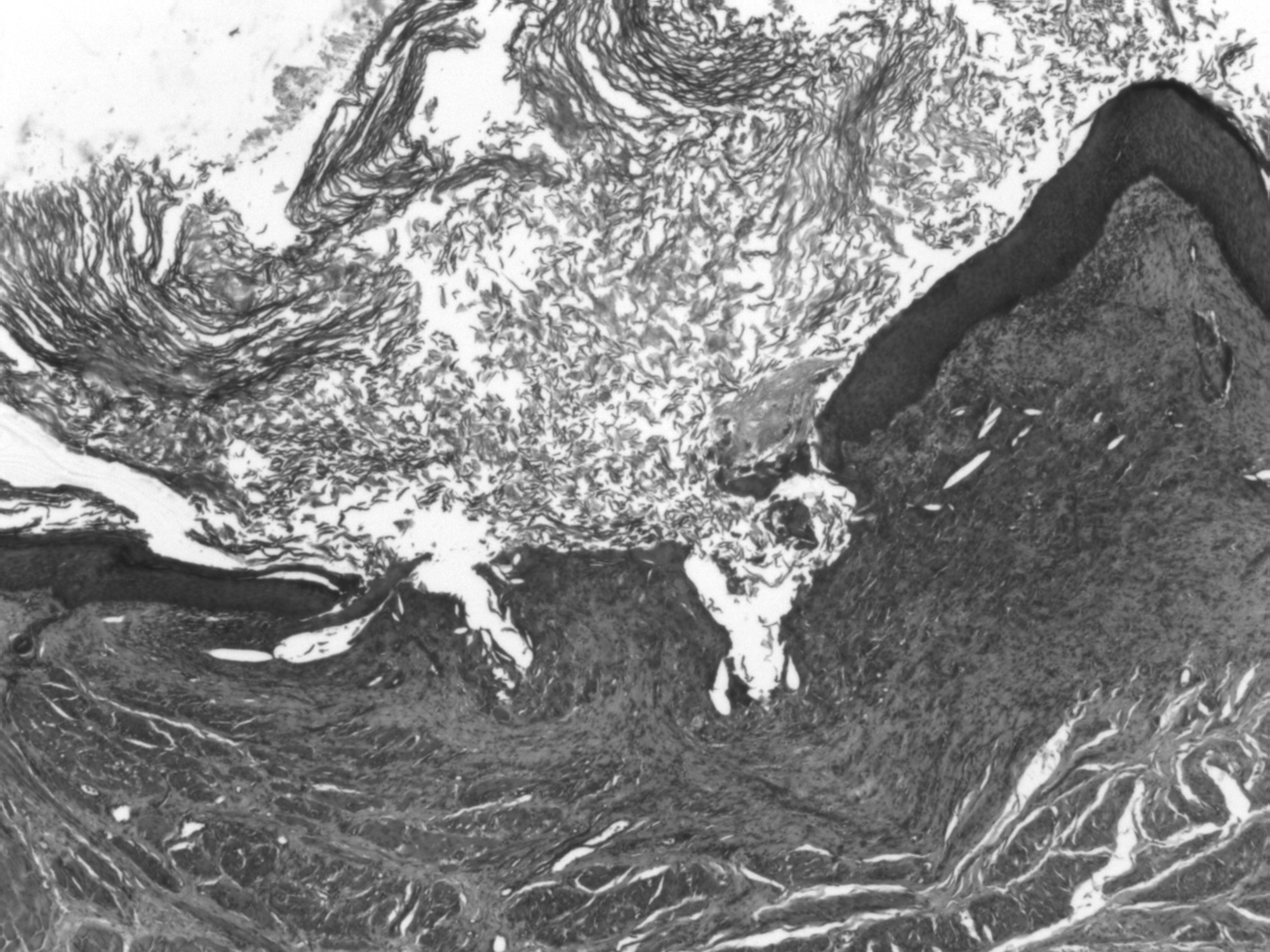
Parietal rupture was present, accompanied by granulomatous inflammation (H.E; 40 ×).
Discussion
The RL of the uterus is a derivative of the gubernaculum and attaches to the paramesonephric duct near the uterotubal junction during development (at 9 weeks' gestation). 1 The RL extends caudally through the inguinal canal to the labioscrotal swelling, forming a fibrous band by the end of the first trimester of pregnancy. Nuck's canal, a portion of peritoneum known in women as the processus vaginalis, carries some layers of the abdominal wall to be incorporated in the round ligament. The RL extends from the uterus through the inguinal canal to terminate in the region of the mons pubis and labia majora. RLs are approximately 10–12 cm long and contain veins, branches from the ovarian artery, lymphatics, smooth muscle, and nerves. RL function is to maintain the anteversion of the uterus. The RL is only rarely the site of primary disease. Tumors of the RL may present intra-abdominally, in the inguinal canal or in the labium, where the ligament is inserted. Common RL tumors are leiomyomas (including epithelioid and bizarre types),2,3 endometriosis, and mesothelial cysts. 4 Other rare tumors such as leiomyosarcomas, 5 malignant perivascular epithelioid cell tumors, 6 “fibromas,” benign mesenchymomas, angiomyolipomas, dermoid cysts, haemangiomas, and nodular fasciitis have been reported.7,8 Striated muscle heteroplasia is an inconsequential incidental finding, which is thought to represent an aberrant persistence of gubernacular rhabdomyoblasts. 9 Only 1 case of EC of RL has been reported in the literature to date. This article described the clinical and pathological features of this case in detail, because the summary has not reported by PubMed and the journal Minerva Ginecologica, which did include such a case, is not easily available. In 1968, Lecca and Belvederi described a pedunculate mass arising from the left RL in a 23 year-old woman. 10 The preoperative diagnosis was ovarian cyst. A laparotomy resection of the lesion was performed. The mass weighed 60 g, was 6 cm in maximum diameter, and was an unilocular cyst, lined by a keratinized squamous epithelium with keratin content, as was shown in one of the figures in the article. 10 A diagnosis of “epidermoid cyst” was decided upon. The patient was well postoperatively and was discharged 11 days after being operated on. To date, the current authors are unaware of any subsequent disease in that patient. The clinical and radiologic differential diagnosis between pelvic RL neoplasms and ovarian/abdominal-wall tumors is difficult. A preoperative diagnosis of the lesion nature is essential for planning optimal treatment. The differential diagnosis of pelvic cystic masses arising adjacent to the ovary includes mesothelial cysts, endometriotic lesions, and dermoid tumors. Because EC is rare, it is is not usually considered in the differential diagnosis.
Conclusions
In the case described in the current article, imaging procedures were helpful for establishing preoperatively the benign nature of a pelvic mass found in a very unusual site. The well-defined margins were been considered as a feature of a benign growth. A minimally invasive laparoscopic approach for tumor excision was chosen. Thus, if a pelvic mass arising adjacent to the ovary is encountered an EC of the RL should be included in the differential diagnosis. Imaging procedures may shown the benign nature of the lesion and it may be removed with a minimally invasive laparoscopic approach.
Footnotes
Disclosure Statement
No competing financial interests exist.