
Abstract
Abstract
Introduction
Most surgical procedures are known to have acute effects on physiology and hence on postoperative laboratory assessments. The expected postoperative changes are useful for health professionals to know as they could influence subsequent monitoring and, importantly, the use of medications during the postoperative period.
Although some reports on specific parameters for postgynecological surgery values are available, such as for inflammation following laparoscopic versus abdominal hysterectomy 1 or for lipids,2,3 there is currently a lack of information that can be used to assess what can be expected as “normal” for premenopausal or perimenopausal women who have undergone an abdominal hysterectomy with a prophylactic oophorectomy for benign indications. Newer less invasive surgical options have shown that the inflammatory response is less aggravated in women who have had laparoscopic surgery as opposed to the conventional open abdominal surgery.4,5 Each type of surgery will cause some level of trauma; however, the extent to which systemic inflammation would be affected would be dependent on the invasiveness and type of surgery performed. What is important to note is that regardless of the invasiveness of the surgery (which would have differential effects on inflammation), a bilateral oophorectomy will likely have the same acute effects on the hormonal changes observed.
The purpose of this study was to document a range of postoperative lipid, hormonal, and metabolic measures at hospital discharge following premenopausal abdominal hysterectomy with bilateral oophorectomy and to compare these values with premenopausal reference ranges. These data aim to help physicians guide subsequent care, which often includes the prescription of hormonal therapy to manage postsurgical menopausal symptoms, and to avoid potential risks, which include thromboembolism, stroke, and adverse cardiovascular events.
Materials and Methods
This study is a planned secondary analysis of data from a randomized double-blind trial comparing the effectiveness of either medroxyprogesterone acetate (MPA) or conjugated equine estrogen (CEE) in preventing post-oophorectomy bone loss, 6 controlling vasomotor symptoms such as hot flushes, 7 and comparing the cardiometabolic changes on the two hormone therapies over 12 months (Kalyan et al. 8 ). The measures in the present study were made before randomization to therapy.
Participants
Women were enrolled between 1989 and 1991 and screened for contraindications to the experimental hormonal therapies as described previously. 6 In brief, women scheduled for a hysterectomy with bilateral oophorectomy were identified from preoperative lists at three teaching hospitals and one community hospital in Vancouver, British Columbia. To be eligible, women had to have menstruated within the past 4 months. Exclusion criteria were as follows: malignancy including cervical cancer (from surgical and pathology reports), use of bone-active medication over the previous 6 months (including steroids, hormone therapy, or medications affecting hormonal levels), thrombotic disease, classical migraine headaches with aura, and clinical hypertension. Women were approached to participate in the study prior to hospital discharge, and those who gave written informed consent to participate were immediately enrolled. This research was approved by the Clinical Screening Committee for Research Involving Human Subjects at the University of British Columbia.
Data from the 33 of 41 enrolled women who completed the 1-year randomized trial 6 and for whom all biochemical assays were performed are included in this report. Fasting morning blood and urine samples were taken on the day of hospital discharge before starting randomized therapy.
Biochemical analysis
Table 1 lists the reference ranges for each assay. Routine fasting hematology, lipid levels, and chemistry values were analyzed in the Vancouver General Hospital laboratory and included total cholesterol, high density lipoprotein (HDL), triglycerides, calculated low-density lipoprotein cholesterol (LDL-C) and fasting blood glucose (FBG), HbA1c, hemoglobin, and complete blood cell count. Serum albumin, apolipoprotein-B (Apo-B), and high sensitivity C-reactive protein (CRP) assays were done by immunonephelometry using a BNII Nephelometer (both reagents and instrument from Dade Behring, Newark, DE).
SD, standard deviation; CI, confidence interval; HDL, high-density lipoprotein; APO-B, apolipoprotein B; HbA1c, hemoglobin A1c; DHEAS, dehydroepiandrosterone sulfate; SHBG, sex hormone binding globulin; WBC, white blood cells.
Below range or †above range indicate skewed distributions of the observed data relative to normal reference ranges.
Serum cortisol, dehydroepiandrosterone sulfate (DHEAS), sex hormone binding globulin (SHBG), and testosterone were measured by the Biochemistry Laboratory of the Royal Melbourne Hospital (Melbourne, Australia) on samples that had been separated immediately, frozen at −70°C, and shipped on dry ice so they remained frozen until analysis. Cortisol concentrations were measured by a radioimmunoassay (RIA) with an intra-assay coefficient of variation (CV) of 7.1%. Both DHEAS and testosterone were measured by radioimmunoassay (Diagnostic Products Corporation, Los Angeles, CA) with intra-assay CVs of 7% and 13.4%, respectively. SHBG was measured using an immunoradiometric assay (IRMA, Orion Diagnostica, Espoo, Finland) with an intra-assay CV of 8%.
Statistical analysis and Z score calculations
Data are reported as standardized scores (Z scores) as calculated from laboratory reference ranges from the time the samples were assayed, using the following formula:
where x is the measured value, μ is the reference mean, and σ is the reference standard deviation. From the reference range, lower limit (LL) to upper limit (UL), we computed mean as (LL+UL)/2 and standard deviation (SD) as (UL-LL)/4. For samples drawn from the reference population, about 95% of the Z scores should lie between the values of −2 and +2 (±2 SD from the mean of 0). In the text, Z scores are reported with mean and 95% confidence intervals as (mean; LCI to UCI) unless otherwise stated. Ninety-five percent (95%) CI excluding 0 are interpreted to indicate significant differences from the standard reference range. We also report the proportion of values below, within, and above the reference range limits (Table 1). Z-scores are represented using Tukey box-and-whisker plots (Prism GraphPad version 5.00 for Windows; GraphPad Software, San Diego, CA) with the boxes signifying the 25% and 75% quartiles and the midline denoting the median. Bold dots on the graph show individual points that lie outside that range (Fig. 1).

Postoperative metabolic and homeostatic parameters in 33 women who underwent a hysterectomy and bilateral oophorectomy for benign reasons. Z scores were calculated from premenopausal reference ranges and are represented using Tukey box-and-whisker plots (black dots denote outliers). Dashed lines indicate 2 standard deviations above or below the normal mean. HbA1c, hemoglobin A1c; FBG, fasting blood glucose; HbG, hemoglobin.
Results
The mean age of the women included in the study was 45 (±4.8) years, and the mean body mass index (BMI) was 23.6 (±3.2) kg/m2. The average time of hospital discharge following abdominal hysterectomy with a bilateral oophorectomy was 6.9 ± 4.9 (95% CI 5.2–8.7) days.
Table 1 provides the laboratory reference ranges and observed values from the women included in this analysis. These values are reported in the original units (mean and SD), as Z scores (mean, 95% CI) as well as the proportion of scores that fell within, below, or above the normal range in these women at hospital discharge following abdominal hysterectomy with bilateral oophorectomy.
Postoperative metabolic and homeostatic factors
Figure 1 provides the women's FBG, HbA1c, hematocrit, and serum creatinine levels, which fell within the normal range at the time of postsurgical sampling. However, both hemoglobin (HbG) (Z score = −2.96; 95% CI −2.75 to −2.16) and serum albumin levels (Z score = −2.46; 95% CI −3.50 to −2.43) were markedly below the reference range.
Postoperative serum hormone levels
As shown in Fig. 2, SHBG and cortisol were within the upper end of the normal range. Seventy percent (70%) of the women had SHBG levels within the normal range and 30% had levels that were above normal (Z score = 1.2; 95% CI 0.4–2.0); 73% had normal cortisol levels with 27% having higher values than the reference (Z score = 0.6; 95% CI 0.2–1.1). On the other hand, DHEAS levels (Z score = −1.38; 95% CI −1.6 to −1.2) gathered at the lower end of the reference range, and 70% of the women were significantly below the normal mean values for premenopausal levels of testosterone (Z score = −2.4; 95% CI −2.6 to −2.2).
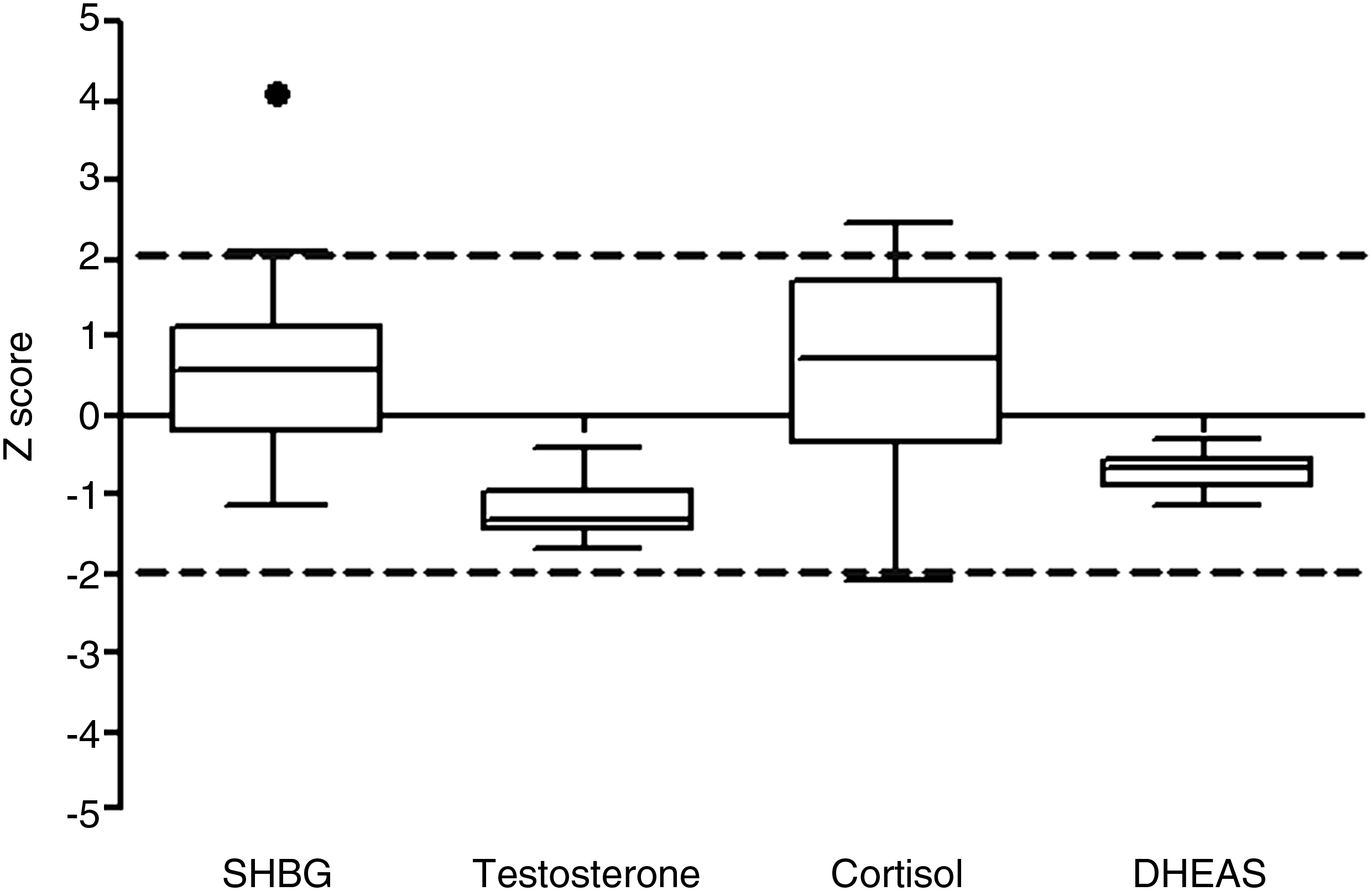
Postoperative serum hormone levels in 33 women who underwent a hysterectomy and bilateral oophorectomy for benign reasons. Z scores were calculated from premenopausal reference ranges and are represented using Tukey box-and-whisker plots (black dots denote outliers). Dashed lines indicate 2 standard deviations above or below the normal mean. SHBG, sex hormone binding globulin; DHEAS, dehydroepiandrosterone sulfate.
Postoperative lipids
Although the majority of women had postoperative triglyceride levels within the reference interval, the values were found to be on the upper end (Z score = 0.7; 95% CI 0.3–1.1), with 9% having above normal values (Fig. 3). Postoperative HDL levels, however, were conspicuously low (Z score = −1.7; 95% CI −2.0 to −1.4). In contrast, levels of total cholesterol tended to be on the upper range of normal (Z score = 1.5; 95% CI 1.3–1.8), with 22% of the women's values above the normal range. Levels for Apo-B, the main constituent of LDL-C, spanned the normal range (Z score = −0.1; 95% CI −0.6–0.4).

Postoperative lipid levels in 33 women who underwent a hysterectomy and bilateral oophorectomy for benign reasons. Z-scores were calculated from premenopausal reference ranges and are represented using Tukey box-and-whisker plots (black dots denote outliers). Dashed lines indicate 2 standard deviations above or below the normal mean. CHOL, cholesterol; HDL, high-density lipoprotein; TRIG, triglycerides; APO-B, apolipoprotein B.
Postoperative hematology
Postoperative white blood cell (WBC) counts were mostly normal (Fig. 4). The lymphocyte (Z score = −1.1; 95% CI −1.6 to −0.6) and monocyte (Z score = −0.7; CI −1.1 to −0.3) fractions of the WBC differential were marginally low and the platelet count was high (Z score = 1.53; 95% CI 1.1–1.9).

Postoperative hematology in 33 women who underwent a hysterectomy and bilateral oophorectomy for benign reasons. Z scores were calculated from premenopausal reference ranges and are represented using Tukey box-and-whisker plots (black dots denote outliers). Dashed lines indicate 2 standard deviations above or below the normal mean. WBC, white blood cells.
Postoperative C-reactive protein
Postsurgical CRP levels (Z score = 20.34; 95% CI 12.4–28.3) were markedly elevated relative to the normal reference range, even though they were measured almost a week after surgery (Fig. 5). Most (82%) women had values significantly higher than the upper limit of the reference range. There was also a negative rank correlation between serum albumin levels and CRP (Spearman r = −0.4; two-tailed p = 0.02).

Postoperative C-reactive protein levels in 33 women who underwent a hysterectomy and bilateral oophorectomy for benign reasons. Z scores were calculated from premenopausal reference ranges and are represented using Tukey box-and-whisker plots (black dots denote outliers). Dashed lines indicate 2 standard deviations above the normal mean.
Discussion
Using a comprehensive list of Z scores for hematological, metabolic, lipid, and hormonal values reference intervals, this study of 33 healthy women having premenopausal oophorectomy and abdominal hysterectomy for benign disease showed depressed levels of HDL, albumin, testosterone, DHEAS, and hemoglobin and significantly elevated levels of circulating CRP. These results provide important information for clinicians in postoperative care by drawing attention to the physiological state of women following this common gynecological surgery at time of hospital discharge.
CRP levels are known to rise after most kinds of surgical trauma, as it is generally an indication of the acute phase response associated with inflammation. CRP levels were shown to rise following both laparoscopic and abdominal myomectomy for fibroids. 1 That study found an increase 4–12 hours following surgery, with CRP values continuing to rise at least up to the third postoperative day. 1 The early release of the inflammatory cytokine, interleukin-6 (IL-6), which peaks on the first postoperative day and subsequently is rapidly downregulated, 1 induces the later release of hepatic CRP as part of the acute phase response. The women in our study also had significantly low levels of albumin. The mean Z-score for serum albumin was −2.5, and 70% of the women had levels below the normal range an average of 1 week following surgery. In some situations, a low serum albumin level is taken as an indication of poor nutritional status or severe liver or kidney disease, but it is also a recognized marker of inflammation. 9 Consistent with the role of albumin in the inflammatory process in our study, we found a significant negative rank correlation between serum albumin levels and CRP. Future studies need to verify that this inverse correlation can be used to assess the degree and severity of systemic inflammation and to monitor postsurgical recovery.
We continued to follow those women who met eligibility criteria for our subsequent randomized controlled trial (RCT), evaluating the cardiometabolic profile of CEE versus MPA for the control of vasomotor symptoms experienced following surgical menopause (Kalyan et al. 8 ). There were no obvious repercussions or adverse events that were proven to be a direct cause of the observed high level of postsurgical inflammation, though one woman was dropped early from the study due to the subsequent development of thyrotoxicosis (cause unknown). Of particular note, the inverse relationship of high CRP and low albumin we report was still present in the CEE arm, but not in the MPA arm of our double-blind parallel RCT (Kalyan et al. 8 ). This is important because CRP, like other metabolic inflammatory markers (such as IL-6 and tumor necrosis factor-α), is also associated with the metabolic syndrome and cardiovascular disease, both of which have a component of dysregulated inflammation.10–12 Therefore, it may be particularly pertinent for women who have undergone surgical menopause to ensure that they do not sustain unhealthy levels of systemic inflammation over an extended period of time.
Lipid profiles are markedly affected by surgical trauma. 3 We found the women had an average Z score of −1.7 for HDL cholesterol at the time of hospital discharge, and their total cholesterol was at the upper end of the normal mean with an average Z score of +1.5. We also noted that triglycerides were slightly increased, although remaining within the normal range, which is similar to previous studies investigating the effects of surgery on lipid metabolism. 3 Others have found that total cholesterol, Apo-B, and HDL are significantly depressed on the first postoperative day, 3 and have generally returned to preoperative levels by 6 months. 2 The degree to which various cholesterol fractions are negatively affected is associated with the type and extent of surgery.2,3 Reron and Huras 2 suggested that women who had a hysterectomy with bilateral oophorectomy were at particular risk of developing atherosclerosis, as they had the highest levels of LDL-C and total cholesterol and lowest levels of HDL cholesterol 6 months following their procedure. These results with surgical menopause were in contrast to women who had a hysterectomy alone, a hysterectomy with unilateral oophorectomy, or a conservative myomectomy. The abnormal blood lipids are important information (and many physicians treating women may be unaware of the consequence of surgery on blood lipids) because these women are most often started on estrogen therapy following bilateral oophorectomy. Our subsequent RCT evaluating the effect of CEE versus MPA found that women on the conventional CEE therapy had significantly elevated triglyceride levels as well as elevated CRP levels (Kalyan et al. 8 ). Together, this may place women at greater risk of cardiovascular events, as has been documented in women taking estrogen following surgical menopause. 13 Should these high levels of CRP, low levels of albumin, and altered lipid metabolism be sustained, these women who underwent premenopausal oophorectomy could potentially be at increased risk for cardiovascular events in the future.
The total mean testosterone and DHEAS were notably below the normal range following the surgery. Seventy percent (70%) of the women had testosterone levels below the expected values for premenopausal women. This observation is consistent with other studies that suggest that testosterone is the major androgen secreted by the postmenopausal ovary.14,15 The women in our study were at the typical later reproductive or early perimenopausal ages (mean age 45 years); therefore, the low levels of these hormones may be reflective of the absolute decline in total testosterone and DHEAS that is observed in the decades preceding menopause. Alternatively, our observation could be a direct effect of oophorectomy, or it could be a combination of the two factors. Women who have had an oophorectomy are found to have significantly lower levels of circulating DHEAS in comparison to age-matched women who still have their ovaries intact. 16
In contrast to the DHEAS and testosterone levels, we found that both SHBG and cortisol values sat within the positive end of the normal reference range and had a much larger degree of variation between women. Hassa et al. 16 found that, although women who had a hysterectomy with or without an oophorectomy had a notable decline in DHEAS by postoperative day 7, only women who had both their ovaries removed had a SHBG level increase, compared with their preoperative values, a week following their surgery. This event may be an acute response to the removal of the ovaries since oophorectomized women eventually come to have relatively low levels of SHBG due to their very low levels of endogenous estrogen, which regulates SHBG expression.
WBC counts normally peak on the first postoperative day, 1 but we found that levels of WBC were relatively normal at hospital discharge, with only 9% of the women presenting with levels above the reference range. The blood cell differential showed that the neutrophil and platelet fractions were still relatively higher than normal, whereas the lymphocyte fraction was slightly low, which is indicative of the role of the innate immune response in healing and trauma. Platelet counts are known to increase in the presence of catecholamine levels and thus also may indicate increased metabolic stress. However, both short-term (FBG) and long-term (HbA1c) measures of blood glucose were within the expected reference range.
These data augment a surprisingly sparse literature on the expected postoperative levels of homeostatic, metabolic, lipid, and hematological values for women who have undergone a premenopausal abdominal hysterectomy with a bilateral oophorectomy for benign reasons. Acute effects can be expected following any type of surgical trauma, especially on markers of inflammation. However, the extent, magnitude, duration, and specific metabolic parameters that deviate from normal would be expected to vary with the type of surgery and whether or not malignancy was present. We were unable to find published longitudinal studies of women who had undergone this common gynecological surgery (who remained hormone-treatment free) that report all of the biochemical parameters we assessed, so it is difficult to say whether these acute effects have any long-term consequences. One study that examined postsurgical inflammatory markers (CRP and IL-6) found that levels had normalized by week 4. 4 However, studies examining lipid levels in women who have had some gynecological surgery have found that abnormalities are still evident at 6 months. 2
Conclusions
It is important to determine how these acute events we report may influence or be influenced by hormonal therapy, which is a common course of treatment for this population of women. In light of the postsurgical inflammatory and lipid values, immediate pharmacological treatment for menopausal symptoms should be considered carefully, because oral estrogen may potentially increase inflammation and put women at greater risk of adverse cardiovascular events.
Footnotes
Acknowledgments
We are grateful to Nenita Alojado, RN, who facilitated the recruitment of participants, Yvette Vigna, who also followed this cohort and managed the database, and Dr. Doug Yackel (as well as the other gynecologists) for referral for potential participation of women under their care. We would also like to acknowledge the contribution of Dr. Sandra Sirrs who, as an endocrine fellow working with Dr. Prior in the late 1990s, had done a preliminary appraisal of part of the data presented in this study. We especially thank the women who participated, kept careful records, provided their observations, and who made this study possible. We also are very appreciative of the technical support from the laboratory staff at the Department of Clinical Chemistry at the Vancouver Hospital and Health Sciences Centre. We also thank Drs. John Wark and Peter Ebeling for facilitation of analyses by the Biochemistry Laboratory of the Royal Melbourne Hospital (Melbourne, Australia). Finally, the Centre for Menstrual Cycle and Ovulation Research is very grateful for the continued support of donors who help fund our nonprofit research organization. This research was approved by the Clinical Screening Committee for Research Involving Human Subjects at the University of British Columbia (Protocol approved April 12, 1988, #C87-272). Funding support was provided by the British Columbia Medical Services through a Vancouver Foundation Grant, an investigator-initiated and controlled grant from Upjohn, and UBC Medical Research #20R-54590, and Centre for Menstrual Cycle and Ovulation Research. Funding bodies did not participate in or dictate the design, analysis, conduct, or reporting of the results of this trial.
Disclosure Statement
No competing financial interests exist.