
Abstract
Abstract
Introduction
Lasmar et al. 6 suggested a new classification (NC) system for submucosal leiomyoma based on size, width of base, location, and penetration depth into the myometrium. These researchers scored submucosal leiomyomas in 55 women who underwent myolysis and suggested whether or not an alternative nonhysteroscopic technique was reasonable based on the total score.7–9 In patients with high scores for submucosal leiomyomas, transabdominal myomectomy was deemed necessary for the preservation of the uteri. 6
The current authors have performed transvaginal radiofrequency (RF) myolysis since 2004 for premenopausal, postchildbearing patients with submucosal leiomyoma who exhibited symptoms but wanted to preserve their uteri. RF myolysis does not require general anaesthesia or admission care and reduces postoperative bleeding and pain. Patients may resume their daily activities within a few hours of surgery. In the present prospective observational study, this article reports the current authors' experience with a group of patients who underwent transvaginal RF thermal ablation of uterine submucosal leiomyomas of all NC grades, with emphasis on the safety and efficacy of this procedure.
Materials and Methods
Methods
Premenopausal women who visited St. Mary's Hospital, Seoul, South Korea, with a symptomatic single submucosal uterine myoma from January 2005 to October 2007 were included in this study. All patients were past childbearing age but had declined hysterectomy or a uterus-preserving procedure, such as myomectomy or uterine artery embolization. Exclusion criteria were as follows: previous treatment with gonadotropin-releasing hormone agonists; more than three uterine fibroids; abnormal findings in cancer-screening tests and coagulation tests; current pregnancy; recent pelvic/endometrial inflammatory disease; and a positive Chlamydia/gonorrhoea polymerase chain reaction test. Myoma size was not included in the exclusion criteria.
The myomas were grouped on the basis of the NC scoring system of Lasmar et al. 6 and preoperative transvaginal ultrasonography and magnetic resonance imaging. The NC scoring system considers the size, degree of nodule penetration into the myometrium, nodule base extension with respect to the uterine wall, and myoma location. Scoring was based on the size (myomas ≤2 cm, score 0; 2- to 5-cm myomas, score 1; and myomas >5 cm, score 2), the degree of nodule penetration into the myometrium (myomas completely within the cavity, score 0; greater penetration into the cavity, score 1; greater penetration into the myometrium, score 2), the extension of the nodule base with respect to the uterine wall (myomas covering one third or less of the wall, score 0; nodule base occupying one third to two thirds of the wall, score 1; and nodule affecting more than two thirds of the wall, score 2), and the location of the myoma (nodules located in the upper third of the uterus, score 2; those located in the middle third, score 1; those in the lower third score 0; if the myoma was located on the lateral wall, an additional point was added regardless of the affected portion of the uterus). In the current study, myoma classifications were established according to the final score, and management plans were based on myoma classification, as suggested by Lasmar et al. 6
All patients were advised extensively on the potential risks and benefits of the procedure and on possible alternative surgical treatments. The study protocol was reviewed and approved by the ethics and research committee of the Catholic University Medical College of Korea, in Seoul, and informed consent was obtained from all patients.
Pre- and postoperative myoma volumes were measured by three-dimensional ultrasonography using the vital organ computer-aided analysis (VOCAL) volume calculation method. Sonographic evaluation was repeated at 1, 3, 6, 12, and 18 months postoperatively. To minimize interpersonal variation, ultrasonograms were assessed by a single trained gynecologist. Patients were followed for postoperative complications, such as vaginal bleeding, abdominal pain, fever, increased vaginal discharge, and dyspnea during hospital visits for routine follow-up ultrasonograms. Patients were questioned about their satisfaction with RF myolysis at 18 postoperative months. The effect of their symptoms on health-related quality of life (HRQoL) was assessed at their initial visit and last follow-up visit by using the Uterine Fibroids Symptom and Quality of Life (UFS-QOL) questionnaire. 7 Patients were asked to rate their severity of symptoms (higher scores indicated greater symptom severity and lower scores denoted minimal symptom severity). Summed scores were based on the HRQoL subscales, which included concerns, activities, energy/mood, control, self-consciousness, and sexual function. Higher summed scores indicated better HRQoL.
Materials
The RF delivery system (RF Medical System, M-1004) consisted of an RF generator operating at 400 KHz with a maximum power of 120 watts and at temperatures ranging from 40°C to 99°C.
The generator displays the temperature of the needle tip, tissue impedance characteristics, and procedure time. The system is connected to a needle to a 25-cm-long, 18-gauge needle that is centrally cooled with an exposed tip at the distal end. The needle for RF myolysis is of the straight, firm type with a sharp end.
Procedure
RF ablation of uterine myomas was performed under intravenous (i.v.) anaesthesia with propofol sodium under the supervision of an anesthetist. Propofol was administered i.v. in a single bolus dose (2 mg/kg) and then injected continuously (5 mg/(kg · h)) via an infusion pump. Patients inhaled 8 L/minute oxygen through a mask and were monitored using a pulse oximeter.
The patients were placed in the lithotomy position. Preoperative i.v. antibiotics were not given and skin preparation and enema were not performed. To confirm pathology, biopsy was performed at the center of the myoma using a biopsy gun under ultrasonographic guidance before myolysis.
The RF needle was transvaginally inserted through the cervical canal. Under ultrasonographic guidance, the needle tip was centralized in the leiomyoma. Ultrasonography was performed transabdominally or transrectally. After needle centralization, ablation was performed. The temperature of the needle tip was 85°C, and the generator automatically adjusted the power to maintain the selected temperature. During ablation, the myoma was monitored by ultrasonography, and the duration of ablation was based on the increased echogenicity of the myoma. If a postechogenic shadow was noted, this meant that the ablation was progressing successfully. Myomas have high echogenicity during ablation, and ablation was stopped when the area of high echogenicity reached 90% of the leiomyoma cut area. Increased echogenicity disappeared within 20 minutes after ablation. Complete ablation of a 3-cm myoma typically took 5 minutes, while that of a 5-cm myoma took almost 10 minutes. Multiple overlapping ablation cycles were performed for fibroids if they showed an inadequate increase in echogencity during procedure.
After surgery, the patients were monitored for 2 hours. Routine intramuscular injections of 75 mg of diclofenac sodium were used to control pain. The postoperative medication regimen was as follows: 100 mg b.i.d. aceclofenac and 250 mg t.i.d. cefaclor monohydrate for 7 days. If the patient did not have any abnormal findings, such as unstable vital signs, increased temperature, severe abdominal pain, or profuse vaginal bleeding within 2 hours postoperation, the patient was discharged and permitted to resume daily activities.
Statistical analysis
The volume reduction rate was calculated as follows: (initial volume − final volume) × 100/initial volume. Statistical differences were determined using Student's t-tests and analysis of variance (ANOVA) multiple comparison. Statistical significance was set at p < 0.05.
Results
A total of 68 patients, each with a single submucosal myoma, were initially included in this study; however, 2 patients were excluded because they did not keep their appointments at the hospital as scheduled. Eight (8) patients with grade I submucosal myoma who underwent transcervical myomectomy immediately following myolysis under i.v. anaesthesia without hysteroscopy were also excluded. Thus, a total of 58 patients were finally included in this study.
Mean patient age was 45 years (range: 42–51), and mean parity was 1.9 (range: 1 to 6). Preoperative presenting symptoms included menorrhagia (38%), abnormal bleeding (37.8%), dysmenorrhoea (10.2%), and mixed symptoms (14%). Preoperative leiomyoma grades are shown in Table 1.
Groups refer to Lasmer's management groups. See ref. 6.
Preoperative mean leiomyoma diameter was 4.9 ± 1.8 cm (range: 2.5–8 cm). Postoperative mean diameter was 3.0 ± 1.8 cm (range: 0–6.5 cm) 3 months and 2.1 ± 1.2 cm (range: 0–4.1 cm) 6 months after surgery. The volume reduction rate of the leiomyomas was 75.5 ± 14.1% at 3 months and 80.7 ± 22.1 % at 6 months postoperation. There were no differences in the volume reduction rate according to the preoperative leiomyoma grade.
The reoperation rate among patients was 3.4%. A second myolysis was performed on 2 patients with grade III submucosal leiomyomas within 2 months of their first myolysis caused by bleeding as a result of transcervical fibroid tissue passage. In 1 patient, the leiomyoma disappeared completely during follow-up (Fig. 1).
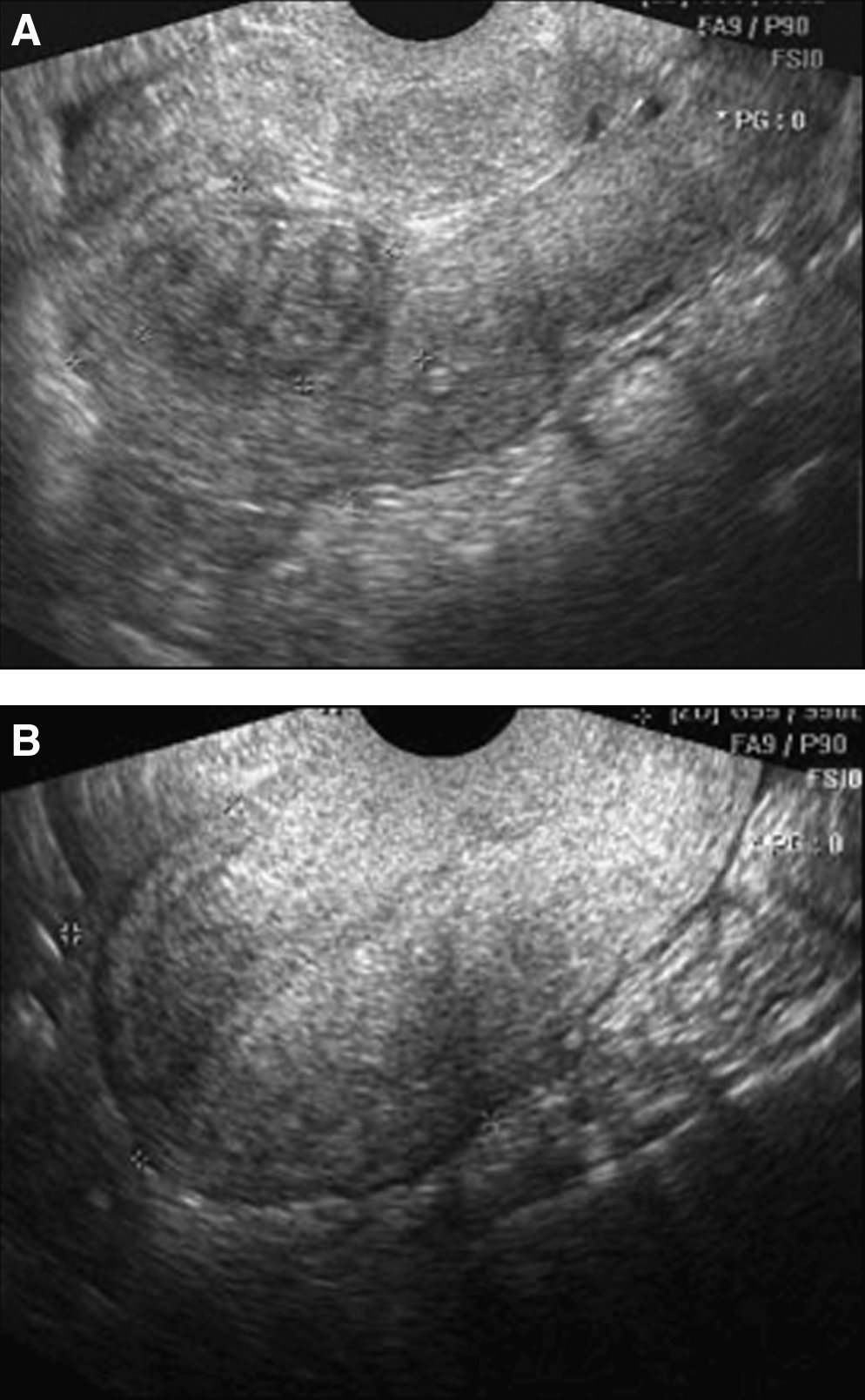
Premyolysis and postmyolysis views of submucosal leiomyoma. 2.4 × 3-cm-sized submucosal leiomyoma
Symptom scores and HRQoL scores, as measured by the UFS-QOL questionnaire, showed improvements 18 months after myolysis (Table 2), with no differences observed in the scores between preoperative grades. Patient satisfaction rates at 18 postoperative months were as follows: “Very satisfied,” 62.0%; “satisfied,” 22.4%; “not bad,” 12.0%; “unsatisfied,” 3.4%; and “very unsatisfied,” 0%.
p-Value < 0.05 versus the previous assessment.
HRQoL, health-related quality of life.
Complications
Penetration/burn injuries of the bowel or bladder, sepsis, shock, embolism, and peritonitis were not seen. The distribution of postoperative pain duration was as follows: within 2 hours, 75.5%; within 2–24 hours, 21.1%; and within 1–7 days, 3.4%. The distribution of postoperative vaginal spotting duration was as follows: 2 weeks, 29.3%; 2–4 weeks, 65.5%; and 4–8 weeks, 5.1%. Increased vaginal discharge was noted in 20.6% of the women; of these, the discharge lasted <4 weeks in 9 women (75%), 4–6 weeks in 2 women (16%), and 8 weeks in 1 woman (8%).
Discussion
Hysteroscopic myomectomy has been the standard approach for treating submucous leiomyoma since it was first described in 1976. 8
Hysteroscopy is a minimally invasive surgical procedure, but it is not harmless. Three types of complications could develop during or after hysteroscopy: (1) intraoperative (perforation, shock, bleeding, cervical tear); (2) postoperative (infection, bleeding, hematoma); and (3) late adhesions. The success of hysteroscopic surgery depends mainly on the size of the uterus and the ratio between the intracavitary portion and the intramuscular portion of the leiomyoma. Fernandez et al. 9 studied 289 cases of hysteroscopic resection of leiomyoma and reported the predictive factors of failure: size (>5 cm); number of intracavitary leiomyomas (>3); and hysterometry (>12 cm). Many researchers agree with these limitations of hysteroscopic myomectomy. Donnez et al. 10 and Hart et al. 11 noted that, when myomas were larger than 50 mm or when submucosal leiomyomas were associated with an enlarged uterus and/or were of intramural class 2 (submucosal fibroids whose largest portion is located in the myometrium) or 3 (multiple > 2 submucosal fibroids diagnosed by hysterography and echgraphy), the results of hysteroscopic myomectomy were not expected to be good.
Hart et al. 11 showed that the best results were obtained when the uterus was smaller than the typical size at 6 weeks gestation and the fibroid was smaller than 3 cm in diameter and located mainly intracavitary. 11 Salim et al. 12 concluded in 2005 that myomas >50% intramural should be treated with hysteroscopic surgery only. Preoperative evaluation of the state of submucosal myomas in terms of size, location, and extension into the myometrium is therefore very important for achieving the best postoperative results.
The current study used the NC scoring system suggested by Lasmar et al. 6 Myoma grouping was based on the total score. Lasmar et al. suggested treatment according to the highest score obtained. For example, if the total score is 0–4, the myoma is classified as group I, and the suggested treatment for this grade is hysteroscopic myomectomy. Myomas scoring 5–6 are group II, and complex hysteroscopic myomectomy with preoperative GnRH analogue therapy and/or two-stage surgery are suggested for this grade. If the score is 7–9, the myoma is considered group III, and the recommended treatment is nonhysteroscopic resection technique.
In the current study all grades of submucosal leiomyoma were treated with RF myolysis. The volume reduction rate of leiomyomas was 95.5 % (grade I), 85.6% (grade II), and 91.1% (grade III), with no statistical differences among the grades. The similarity among the reduction rates, regardless of grade, was very encouraging. If patients of postchildbearing age have a submucosal myoma of a high group and do not desire a hysterectomy or hysterotomy, RF myolysis could be an appropriate treatment for these patients.
Although complete resolution of myoma was noted in 1 case, in most cases, submucosal leiomyomas did not disappear completely after RF myolysis. As with uterine artery embolization, it is difficult to judge uterine wall integrity and strength after myolysis, and fibroid-related distortion of the endometrial cavity remains unexplored. Thus, it is not clear whether RF myolysis is suitable for patients who want to preserve their fertility and bear children in the future. Nevertheless, for all fibroid-related symptoms except infertility, myolysis offers an opportunity for significant improvement in symptom resolution and HRQL. In the current study, patients showed considerable improvement in symptom scoring and HRQoL even if their submucosal leiomyomas were graded high. These results are similar to our previous report on RF myolysis. 13
Leiomyomas undergo hydropic degeneration and necrosis after myolysis, 14 and ischemic necrosis after embolization. 15
Walker et al. 16 reported that 58% of the women who had undergone embolization presented with increased vaginal discharge after the procedure; of these women, the discharge lasted for less than 4 weeks in 28%, 4–8 weeks in 20%, and more than 8 weeks in 16%. These researchers also reported that the persistent discharge in these patients was caused by a superficial cavity within the infarcted leiomyoma communicating with the endometrial cavity. In the current study, increased vaginal discharge was noted in 20.6% of the women; however, the reason for this discharge was not clear.
Postoperative complications such as spontaneous expulsion (2–3%)17,18 and infection (minor infection 5.9%, major infection 2.6%) 17 rarely occur after embolization in submucosal leiomyoma patients, and it is possible that similar complications could occur after myolysis. In this study, transcervical tissue passage with bleeding was noted in 2 patients; however, no incidents of infection or sepsis were reported. These observations may have been the result of the limited sample size; therefore, it is important to consider the possibility of infection and sepsis in future cases.
The mean fibroid volume reduction rate was 80.7% at 6 months after myolysis, and 47.3% after uterine artery embolization (UAE) in a multicentric study 17 ; 3.4% patients underwent further treatment after myolysis, and 18.3% 17 after UAE. However, the overall safety of myolysis is unknown, and the number of procedures performed is too small to draw any conclusion.
In the current authors' experience, approximately 5% of leiomyoma patients are treated using myolysis. The patient selection criteria for myolysis have not yet been established, and the long-term side effects and the rate of tumor regrowth remain unclear. There is no appropriate method to check the margin of the coagulated area in the operative field; therefore, if coagulation is incomplete, the leiomyoma will recur after a few years. More studies are required on the efficacy and safety of this procedure.
Conclusions
Transvaginal RF thermal ablation represents a promising treatment modality for patients with symptomatic submucosal leiomyoma, especially for those with high-grade myomas with no other choice for treatment except hysterectomy or hysterotomy. RF thermal ablation appears to be safe and effective for all patients with leiomyoma-related symptoms, except infertility in the current authors' experience. Therefore, when leiomyoma patients have reached postchildbearing age, RF thermal ablation can offer significant improvements in symptom resolution and HRQoL and should be considered for the treatment of symptomatic submucosal leiomyoma.
Disclosure Statement
No competing financial conflicts exists.