
Abstract
Abstract
Introduction
Molar pregnancy and gestational trophoblastic neoplasm (GTN) describe a broad spectrum of diseases that vary in presentation, course of disease, and tendency for local invasion and metastasis. Invasive GTN can erode into uterine vessels and through myometrium, causing vaginal or intraabdominal hemorrhage. 6 Metastases are often also hemorrhagic at the site; thus, patients may present with hemoptysis, intraperitoneal bleeding from hepatic rupture, or acute neurologic changes. 7 The most common sites of metastatic disease include the lung (80%), vagina (30%), brain (10%), and liver (10%). Adrenal metastasis has rarely been reported. 8
Idiopathic adrenal hemorrhage in a patient with GTN in the absence of metastatic disease has not been published previously. We present a case of spontaneous adrenal hemorrhage in a woman who had nonmetastatic GTN and who presented with abdominal pain, fever, and a 16-cm right upper quadrant mass.
Case
A 33-year-old G1P0 with last menstrual period on April 22, 2009 presented to her gynecologist on June 23, 2009 with heavy vaginal bleeding. She had an unremarkable past medical history. Surgical history included loop electrosurgical excision procedure, knee surgery, and sinus surgery. Medications included prenatal vitamins. She was married, denied alcohol, tobacco, or drug use, and denied a history of trauma. A quantitative human chorionic gonadotropin (hCG) was 21,494 and pelvic ultrasound revealed a normal uterus, without evidence of intrauterine pregnancy or retained products of conception, and normal adnexa bilaterally. Her vaginal bleeding subsided over the next 5 days. The working diagnosis was a spontaneous abortion as hCG levels were decreasing. Suspicion of an ectopic pregnancy was low on the differential.
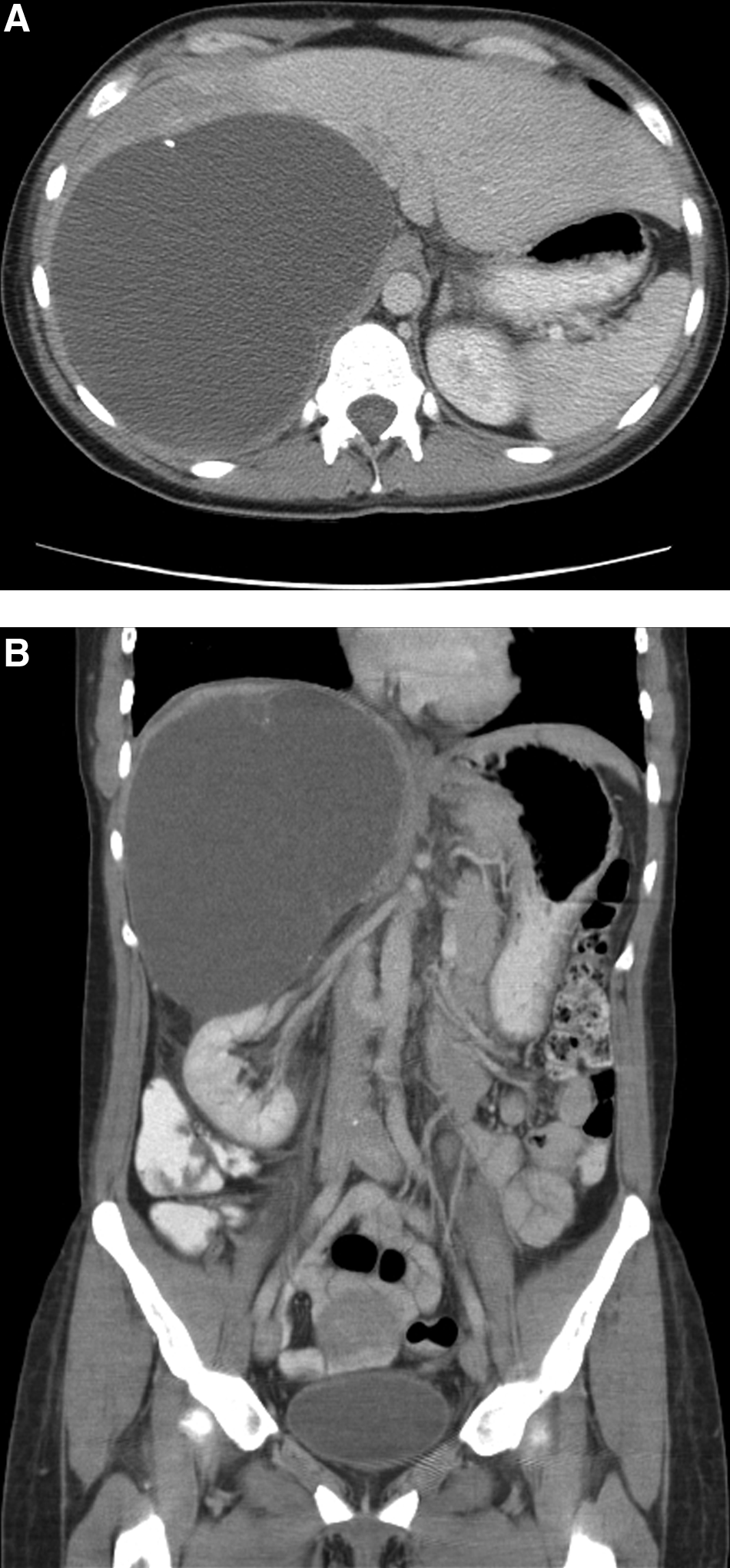
On June 28, 2009, she presented to the Emergency Department with worsening abdominal pain and fever. Pelvic ultrasound was unchanged, and her quantitative hCG was 1028. She was admitted for observation because of her fever of 103°F and abdominal pain out of proportion for a spontaneous abortion. Her heart rate and blood pressure were within normal range. Laboratory values revealed normal chemistry and hepatic panels, white blood cells 12,300, hemoglobin 11.5 g/dL, platelets 344 109/L, fibrinogen 728 mg/dL, international normalized ratio 1.28, and partial thromboplastin time 37. Urinalysis results were normal and blood cultures were negative. A computed tomography (CT) scan of the abdomen and pelvis revealed a 16.5-cm × 15.1-cm × 13.4-cm cystic lesion in the right upper quadrant of the abdomen with unclear origin (Fig. 1A and B). The cystic lesion was initially thought to be arising from the liver. Aspiration of the cyst was performed and analysis was remarkable only for the presence of erythrocytes. Cytopathology was negative for malignancy. Studies for echinococcus antibody, aerobic culture, anaerobic culture, fungal culture, and parasite stain were all negative. Serum tests for echinococcus antibody and Entamoeba histolytica antibody were obtained and were negative, and serum metanephrine was normal. At this point, she was transferred to the University of Minnesota Medical Center for further management. A magnetic resonance imaging scan of the abdomen and pelvis confirmed a 17.3 × 14.9 × 13.8-cm mass in the right upper quadrant causing marked compression of the right hepatic lobe and intimately associated with the hepatic capsule and the right adrenal gland. On July 8, 2009, the patient underwent ultrasound-guided placement of a percutaneous catheter to drain the cyst. Again, bloody fluid was aspirated and cultures, Gram stain, fungal and parasitic studies, and cytopathology were all negative. She was discharged home 2 days later with the drainage catheter in place and with a plan for surgery by the hepatobiliary team.
During that hospitalization, her hCG decreased to 693. The Gynecology Department was consulted, and a repeat pelvic ultrasound was again unchanged. The working diagnosis remained a spontaneous abortion, and follow-up was arranged as an outpatient with her primary gynecologist. At her follow-up visit, the hCG level was dramatically elevated to 4180
On July 23, 2009, en bloc resection of the right adrenal gland and mass was performed, as intraoperative findings showed the mass to be arising from the right adrenal gland, consistent with an adrenal hematoma. Pathology review confirmed adrenal hematoma with no evidence of trophoblastic tissue to suggest metastatic GTN. She had an uncomplicated postoperative course and was followed up in the gynecologic oncology clinic for GTN.
On the day of her surgery, approximately 1 week after receiving methotrexate, the hCG was 1572. She continued weekly methotrexate 50 mg/m2 IM. On July 31, 2009, her hCG was 2583, and on August 6, 2009, the hCG was 3075. Workup for possible sites of metastatic disease was initiated and CT imaging results of her head, chest, abdomen, and pelvis were negative. She continued treatment with methotrexate, and her subsequent hCG levels regressed and remained negative after 9 weekly doses of methotrexate.
Conclusions
This is a case of spontaneous adrenal hemorrhage in the setting of gestational trophoblastic disease without evidence of metastatic disease. This is the first published case to our knowledge of this combination of events. It is most common for hemorrhagic complications associated with GTN to be secondary to metastatic disease, and cases of idiopathic nontraumatic adrenal hemorrhage are rare.
The patient presented with abdominal pain, fever, and a large abdominal mass at the same time she was being evaluated for GTN, initially raising the suspicion of metastatic disease. Intraoperatively, it was apparent that the mass was a hematoma of the adrenal gland, and pathological analysis confirmed no evidence of metastatic disease. Because metastatic GTN is commonly associated with hemorrhage, this should be at the top of the differential when cases such as these arise.
Unilateral adrenal hemorrhage is usually secondary to trauma, NSAID use, coagulopathy, underlying adrenal tumor, or stress. Severe stress that has been shown to cause adrenal hemorrhage includes surgery, sepsis, hypotension, and burns. 9 In this case, there was no history of trauma, NSAID or anticoagulant use, or evidence of underlying adrenal tumor. A potential underlying cause for adrenal hemorrhage in this case was stress from GTN. It has not been previously reported that adrenal hemorrhage has occurred in the presence of malignancy, aside from metastases to the adrenal gland itself. In addition, the potential stress caused by malignancy is not generally known to be so severe that it causes secondary problems such as adrenal hemorrhage. Therefore, given the absence of metastatic GTN to the adrenal gland in this patient, we assume that the two processes were unrelated and occurred coincidentally at the same time in this case.
Adrenal hemorrhage can cause acute adrenal insufficiency and shock, and these patients must be closely observed and corticosteroids must be administered if signs of adrenal insufficiency are present. Although nontraumatic adrenal hemorrhage is rare, it should be considered when patients present with abdominal pain, fever, and an abdominal mass.
Footnotes
Disclosure Statement
No competing financial interests exist. J.S. Carter is supported by award number T32CA132715 from the National Cancer Institute.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health.