
Abstract
Abstract
Introduction
The diagnosis of appendicitis is based on clinical signs and symptoms, laboratory data, supplemented with noninvasive imaging techniques. A recent study evaluated magnetic resonance (MR) imaging performed in 148 consecutive pregnant patients. Fourteen (14; 10%) of patients had findings consistent with appendicitis. Perforation occurred in 3 (21%). MR results were negative in 125 of the 134 patients; the false-positive rate was 9 (7%). 5
The major risk factor for acute appendicitis in pregnancy is in fact perforation. The accompanying complications associated with perforation are maternal and fetal morbidity. Two (2) studies determined that the presence of perforation was the only predictive factor for maternal morbidity.6,7 Preterm labor and fetal mortality are complications, which occur with greater frequency with perforation (52% versus 17%). 7 In one study of 94/9793 appendectomies in pregnancy, the overall perforation rate was 14.9% (8.7% first trimester, 12.5% second trimester, 26.1% during third trimester. Infant mortality 3.2% abortion rate 13.0%). 8
In the study cited previously, out of 22 cases of acute appendicitis in pregnancy, 12 cases were found to have perforated (55%). In still another report out of 67 cases, 8 were perforated at the time of surgery (12%). 9
Andersen and Nielsen retrospectively reviewed case records of 56 women who underwent appendectomy during pregnancy (1985–1997). They reported no maternal morbidity related to appendectomy even with perforation. However, 4/12 (33%) women who underwent appendectomy in the first trimester aborted. Preterm delivery occurred in 14% of women who underwent second trimester appendectomy. 10 No pregnancy complications occurred following third-trimester appendectomy. All of the above citations recommended the prompt surgical treatment of not only perforated but also of acute appendicitis during pregnancy. Recently the medical management of ruptured appendix during pregnancy has been reported, but in only 2 cases. 11 Nonsurgical treatment of ruptured appendix has also been reported for nonpregnant patients but is typically followed by interim appendectomy after the phlegmon has receded, particularly if abscess formation persistent or recurrent.12,13
We report a case of the nonsurgical management of a ruptured appendix during the second trimester of pregnancy, which resulted in serious complications including the rare occurrence of a uterocutaneous fistula.
Case Report
A 19-year-old white, primigravid woman at 23 weeks' gestation presented on October 14, 2009 with a 4-day history of abdominal pain mainly in the right lower quadrant, nausea, and vomiting. The past medical history was negative and the review of systems revealed no abnormalities other than the above noted gastrointestinal symptoms. Abdominal examination revealed a 22-week uterus, abdominal guarding, and tenderness but no rebound. A CT scan on the day of admission showed a 4.2 × 5.1-cm right lower quadrant mass consistent with focal phlegmon and periappendiceal abscess measuring up to 1.8 cm. The appendix itself was not visualized. The terminal ileum was thickened as well. Diagnosis was made of probable ruptured appendix. The patient had intermittent but irregular uterine contractions. The fetal heart rate was 140 beats per minute, and the white blood cell (WBC) count was 14,900 with a left shift. Blood pressure was 110/59, pulse was 97, respirations were 18, and temperature was 100.3°F. The heart rate subsequently rose to 120 beats per minute. By October 15 the patient felt better and the guarding had diminished; however, her temperature rose to 102.8°F and the WBCs remained elevated at 12,700, hemoglobin was 8.0, and hematocrit was 24. The general surgical consults did not wish to perform a laparotomy but instead recommended that antibiotics be administered and any abdominal collection be drained with imaging guidance percutaneously. On October 19, 2009 an ultrasound-guided attempt at peritoneal abscess drainage was attempted. A second attempt at drainage occurred on October 22, 2009, a small amount of gross pus was aspirated. The culture of the pus was positive for Escherichia coli. On October 23, 2009, a pelvic examination revealed the cervix to be 1–2-cm dilated and 70% effaced. A maternal fetal medicine (MFM) consultation was obtained and antenatal steroids were administered in two doses. The patient continued with intermittent abdominal pain and borderline WBC counts. On October 25, 2009, the WBC was 17,000. On November 11, 2009, the patient was in active labor. Because of the breech presentation, the ongoing intra-abdominal abscess formation, and suspected chorioamnionitis, a cesarean section (C-section) was performed on November 11, 2009. The general surgeons were also asked to scrub. A classical C-section was performed. The placenta weighed only 163 g and was stained with meconium. The infant was in good condition and was transferred to the neonatal intensive care unit. The surgeons found an abscess adherent to the anterior abdominal wall located between the uterus and the abdominal wall. The cavity was in fact entered and contained only the percutaneous drainage catheter. Extensive intestinal adhesiolysis was carried out but the appendix was not removed. A large amount of adhesions and matted bowel remained in the right lower abdomen. The patient was discharged November 16, 2009. She was readmitted to the hospital via the emergency room on November 19, 2009 with abdominal pain and fever. A CT scan revealed an abscess in the right lower abdomen and pelvis measuring 14 × 14 × 7 cm and containing gas bubbles. A (10 french) percutaneous drain was placed into the abscess for drainage (500 mL recovered). The patient received Ivanz 1 g IV daily. The culture showed mixed gram positive and negative organisms. The patient was discharged on November 25, 2009 with the drain in place.
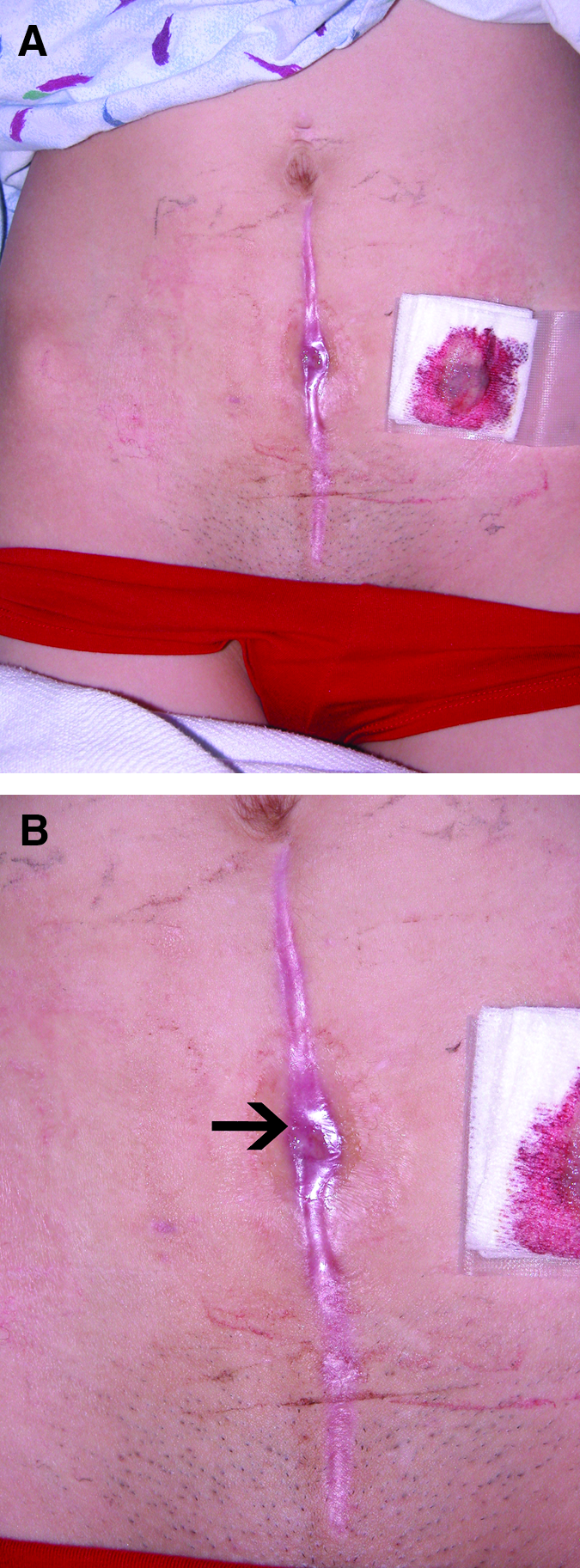
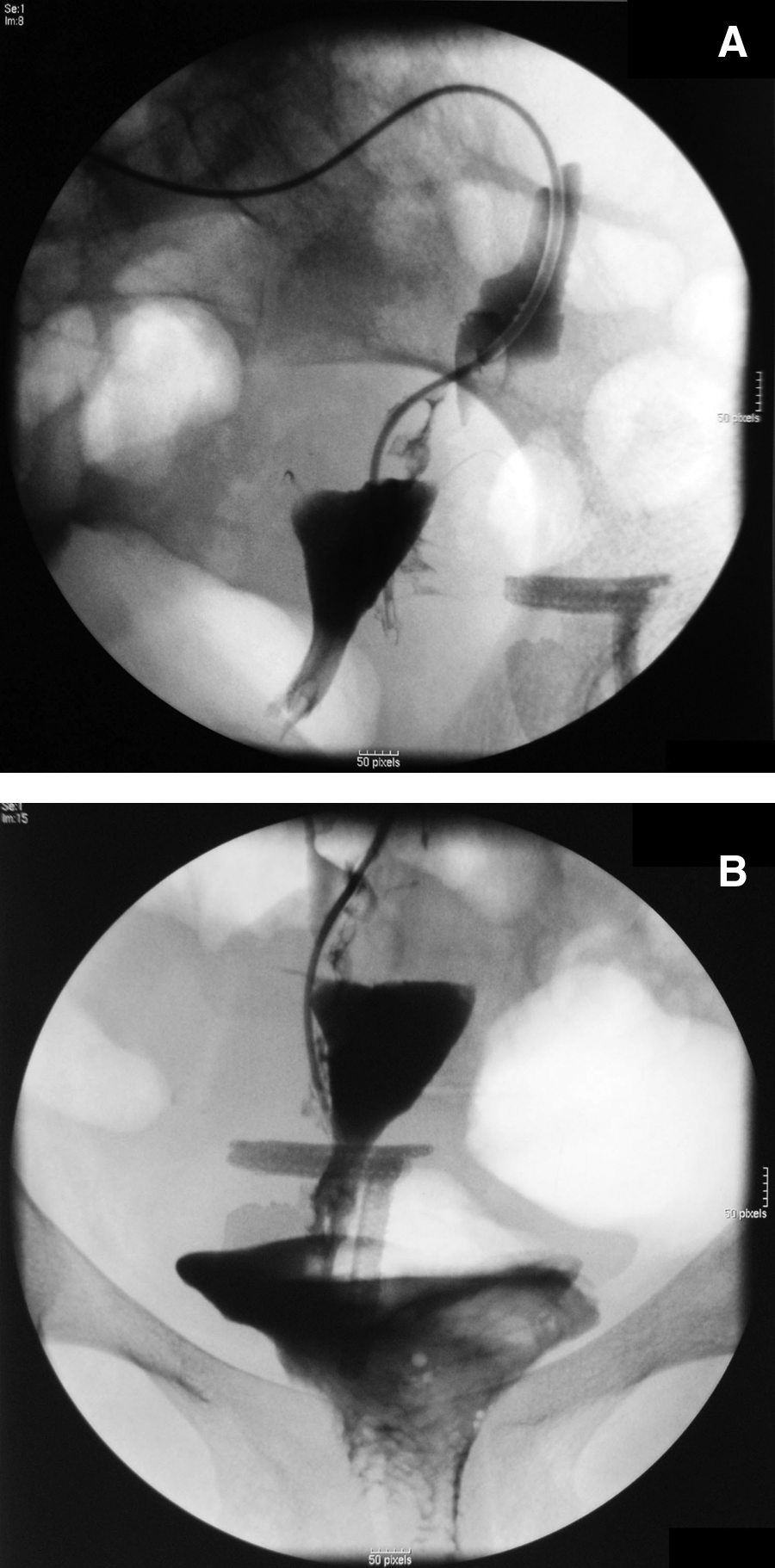
The patient was readmitted for the third time January 26, 2010 and a CT scan again revealed a pelvic collection. An attempt to drain the collection was not successful. The patient began menstruating and noted blood emitting from her abdominal incision (Fig. 1A, B). A CT scan revealed a uterocutaneous fistula (Fig. 2). On January 28, 2010, a fistulogram verified the rather large tract and communication with the uterine cavity (Fig. 3). The patient returned to the gynecology clinic on March 10, 2010 to discuss surgery aimed at taking down the fistula and exploring the appendix and the distal ileum. Preparatory to this plan, the patient had a repeat CT scan. The scan showed the terminal ileum to be thickened and an ilealcutaneous fistula to be exiting the abdominal wall in juxtaposition to the uterocutaneous fistula (Fig. 4). The patient is scheduled for a colonoscopy and gastroenterology consultation.
(

The computed tomography scan shows the uterus (U) communicating with the anterior abdominal wall. The small arrow points to contrast material and air.
(
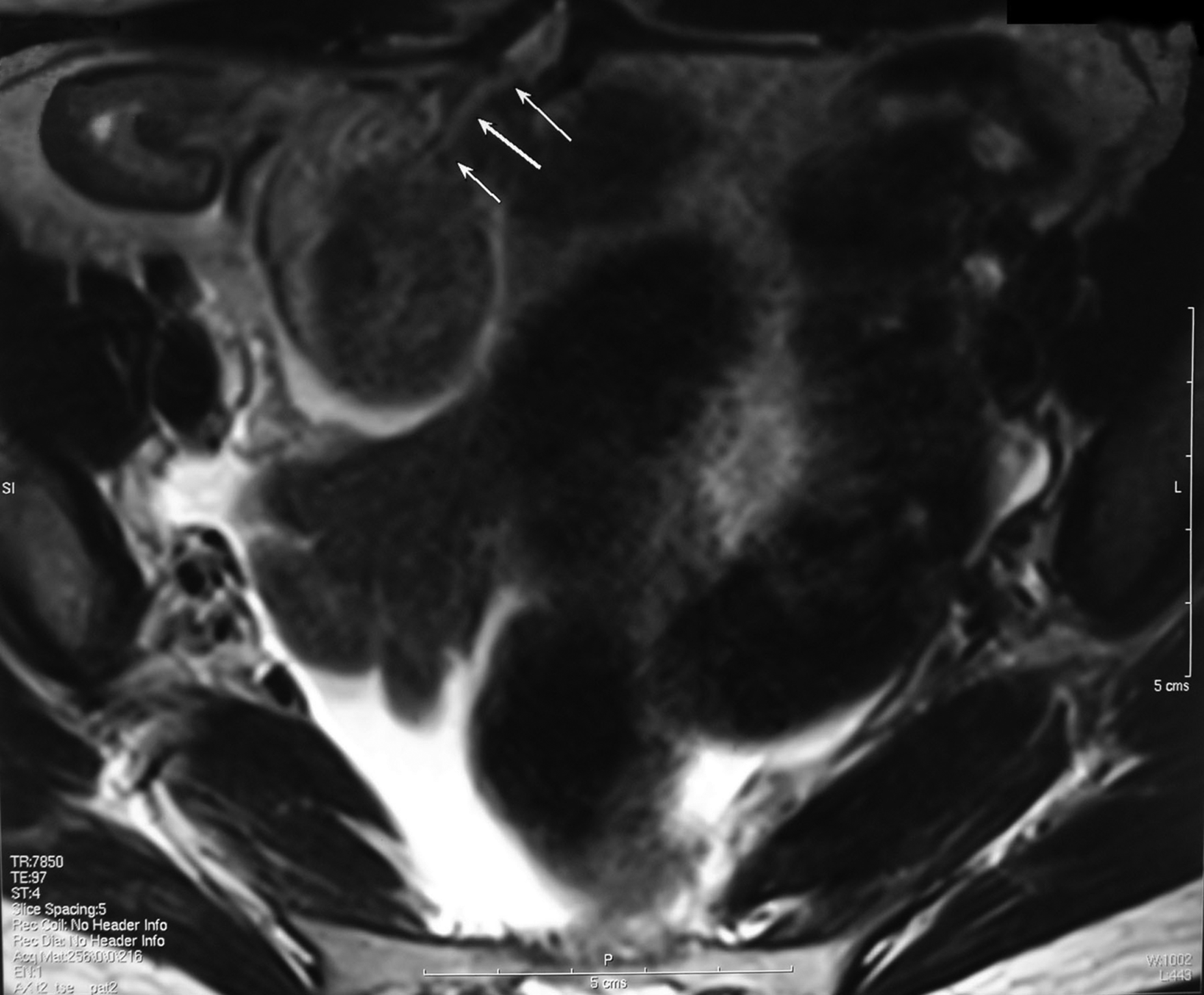
The computed tomography scan of March 2010 shows the uterocutaneous fistula and the ilealcutaneous fistula. The fistulas are juxtaposed and may share a terminal, common channel to the skin surface.
Discussion
In contrast to the occurrence of appendicitis in pregnancy, uterocutaneous fistula formation is a medical rarity. Approximately 120 cases have been reported in the world literature in its entirety over the past 200 years. The term menstrual fistula was first reported by Ballin. 14 A great number of these cases followed C-section, particularly classical C-section. An excellent review on the subject was written by Kirkland in the American Journal of Obstetrics and Gynecology. 15 He divided the fistulas into two types: one in which the fistula emanated from the uterine cavity and communicated directly with the anterior abdominal wall, and a second type where the connection was indirect via the oviduct or tubal stump. Kirkland also identified collateral factors that played an etiologic role and included infections (including tuberculosis); foreign body (e.g., retained gauze, sponge, drain, permanent suture material); and hematometra. Finally, he also reported that spontaneous healing of a uterocutaneous fistula was rare. Aimakhu reported a uteroabdominal sinus following a classical C-section in a 22-year-old woman. 16 The patient menstruated vaginally and additionally menstruated through a small opening in the abdominal scar. Gupta et al. reported a uterocutaneous fistula following a septic abortion in a 32-year-old woman. 17 The patient developed a postabortal abscess in the right perinephric area, which was drained of 400 mL of pus. The abscess reaccumulated and again pus was drained in the amount of 200 mL pus. The wound failed to heal and subsequently the entire menstrual flow drained via the unhealed scar. The patient subsequently underwent a hysterectomy together with excision of the fistulous tract. An article from Turkey similarly reported a uterocutaneous fistula following surgery for an incomplete septic abortion. 18
Okoro and Onwere, 19 Dragoumis et al., 20 and Dessouky and Bolan 21 reported uterocutaneous fistulas following c-section. Shukla et al. reported described an alternative technique for fistulous tract excision. 22
In the case presented here, multiple etiologic factors were involved. The surgeons decision not to perform an appendectomy and explore the ileum and cecum was faulty and resulted in repeated abscess formation as well as preterm labor.
Classical C-section combined with a failure to treat the primary source of the intraabdominal infection created the milieu for uterocutaneous fistula formation. The possibility of Crohn's disease concurrent with appendiceal perforation was never considered because no exploration of the ileocecal area was performed. Inflammatory bowel disease is not uncommon during pregnancy. Generally Crohn's disease does not exacerbate during pregnancy, but it is possible to become active, particularly if there is a provocative event triggering the inflammatory response.23,24
Conclusions
Uterocutaneous fistula is an uncommon complication associated with infection, c-section, and uterine perforation. This complication may be avoided by careful peritonization of the C-section incision, by preventing infection, and by interposition of material between the uterus and abdominal wall.
The ultimate plan for this patient will focus on controlling her inflammatory bowel disease and eliminating the fistulas. This will in all likelihood require excisions of the tracts, repair of the uterus with omental interposition, bowel resection, and possibly ileostomy. 25
Footnotes
Disclosure Statement
No competing financial interests exist.