
Abstract
Abstract
Introduction
Endometriosis at the region of the umbilicus is very rare, having an estimated incidence of 0.5%–4% of all cases of endometriosis,3–5 but has been reported to be found in up to 40% of patients with extrapelvic endometriosis.1,5 Cutaneous endometriosis (including umbilical) predominantly occurs following surgical procedures, which likely lead to iatrogenic seeding of the implants into the region of the scar, but can arise spontaneously. Umbilical endometriosis, first described by Villar in 1886, 6 is the most common site of primary cutaneous endometriosis. Victory et al. performed a review of the literature regarding umbilical endometriosis and recommend that the finding of spontaneous or primary umbilical endometriosis be described as Villar's nodule. 5 The occurrence of primary umbilical endometriosis is thought to arise from retrograde menstruation that migrates from the peritoneal cavity to the umbilicus, but may also be due to embryologic tracts, in which cells fated to become endometrium are laid down in areas other than within the uterus. Patients with umbilical endometriosis typically present with pain (81.5%) or swelling (90.9%) at the site and cyclic bleeding from the region (49.2%). The mean age of those presenting with umbilical endometriosis is 37.7 (ranging from age 23 to 58), with a mean duration of symptoms prior to presentation of 17.8 months (although 2 patients out of 44 experienced symptoms for more than 12 years), and 73.1% of the patients having no history of pelvic endometriosis. 5
Extrapelvic endometriosis has also been shown to occur in the lungs. Joseph et al. reviewed the English language literature from 1966 to 1994 and found 110 cases of thoracic endometriosis. The forms of thoracic endometriosis were distributed as follows: catamenial pneumothorax (73%), catamenial hemothorax (14%), catamenial hemoptysis (7%), and lung nodules (6%). 7 The entity of catamenial pneumothorax is a variant of spontaneous pneumothorax that occurs only in women of reproductive age around the time of menstruation. First described by Maurer et al. in 1958, the menstrually related spontaneous pneumothorax was later named catamenial pneumothorax by Lillington in 1972. 8 Catamenial pneumothorax have been found to occur within 72 hours of the start of menses and are commonly recurrent. 9 Korom et al. state that “not all of a patient's menses coincide with a pneumothorax, but each episode of a catamenial pneumothorax is associated with the menstrual flow.” 10 The mean age of diagnosis is 35 years, with the most common presenting symptoms being chest pain (90%) and dyspnea (31%). 11 A case is presented in which a patient is diagnosed with both primary umbilical endometriosis and recurrent catamenial pneumothorax.
Case Report
The patient is a 43-year-old G2P2002 white woman without significant medical or surgical history. She began menarche at age 13, reported regular menses, and denies any dysmenorrhea or dyspareunia. The patient noted umbilical bleeding at age 23. The bleeding subsequently stopped and no further workup or treatment was performed. On a combined oral contraceptive pill (OCP) from age 25 to 31, the patient recalled some cyclic umbilical bleeding, although decreased. Upon the patient stopping OCPs, the cyclic umbilical bleeding worsened, occurring during most menses. The patient had no difficulty conceiving her 2 children and delivered them vaginally at ages 31 and 34. Following the birth of her youngest child, the patient restarted OCPs, and remained on them for approximately 7 years, with continued cyclic intermittent umbilical bleeding.
At the age of 41 the patient stopped OCPs. One (1) year following the discontinuation of OCPs, the patient experienced her first spontaneous pneumothorax. The patient complained of dyspnea on exertion and pleuritic chest pain following an airplane flight. Although the pneumothorax was not correlated with her menses at the time, the patient recalls her menses occurring within a few days prior to the pneumothorax. A diagnosis of a large right spontaneous tension pneumothorax was made from an x-ray film (Fig. 1A). The patient underwent a right thoracoscopy with a nondiagnostic pleural biopsy and mechanical pleurodesis. A chest tube was placed with full recovery.

Approximately 6 months following the pneumothorax, the patient noticed an 8-mm purple–bluish papule at her umbilicus that was removed in the office setting. Histopathology revealed endometriosis (Fig. 2). One (1) year later, 18 months after the first pneumothorax, the patient experienced pleuritic chest pain after jogging. Her menses had begun 2 days prior. Chest x-ray film showed a large right-sided pneumothorax with tension component and volume expansion in the right hemithorax with a leftward shift of the mediastinal structures (Fig. 1B). A chest tube was placed. The patient was placed on continuous OCPs.
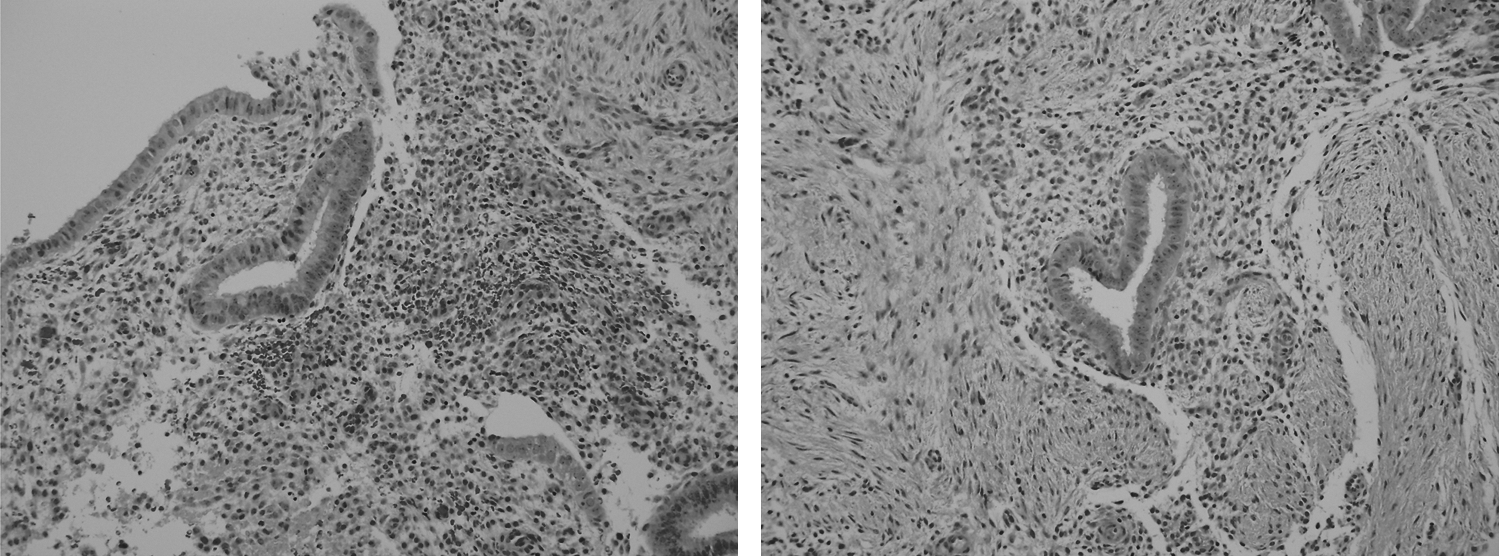
Pathology of umbilical papule. Two histopathology images of the umbilical mass demonstrating glands with columnar epithelium, myxoid stroma, erythrocyte extravasation, and hemosiderin. Both images stained with hematoxylin and eosin at a magnification of 200 × .
While on continuous OCPs, the patient initially had a few episodes of bleeding, with periodic light spotting later in the treatment. Two (2) days following an episode of spotting, the patient experienced a third pneumothorax while running, occurring 9 months after the last pneumothorax (Fig. 1C). A right thoracoscopy revealed a few tiny lesions on the diaphragm that ranged in appearance from brownish to yellow, both porous and intact, with some appearing white and fibrosed (Fig. 3). Mechanical pleurodesis and partial apical pleurectomy were performed. The patient was started on gonadotropin-releasing hormone agonist with an overlap with the OCP until achieving downregulation. Following recovery, the plan is total abdominal hysterectomy, bilateral salpingo-oophorectomy for long-term management.

Thoracoscopy photos at the time of the third pneumothorax showing endometriosis, identical to endometrial implants commonly seen in the pelvis.
Discussion
While most umbilical endometriotic lesions develop following surgery, a few primary umbilical endometriosis cases have been reported.1,3–6,12,13 While it is strongly believed that the majority of umbilical endometriosis occurs when endometrial cells are transported or carried during surgery to the site of the umbilicus, this cannot be used to explain primary umbilical endometriosis. One theory is that the endometrial tissue that enters the peritoneal cavity through retrograde menstruation migrates to the umbilicus. Another thought is that embryologic cells destined to become endometrial cells remain in other tissue during the development. These remnant cells may differentiate into functioning endometrial glands and stroma at times of estrogen stimulation. The differential diagnosis of umbilical nodules can include primary or metastatic cancer, hernia, keloid, residual embryonic tissue, nodual melanoma, pyogenic granuloma, and cutaneous endosalpingiosis. 12 One should always biopsy an umbilical lesion due to the possibility of cancer. 13
Treatment of umbilical endometriosis usually consists of surgical excision, although medical therapy has also been used. In the review by Victory, 67.6% underwent surgical therapy, and 5.9% were treated with medical therapy (one quarter of the patients reviewed had no data available on their form of treatment). 5 Surgery involves a wide or local excision of the lesion and any further repair required following the removal of the tissue. Historically, medical therapy usually consists of either progesterone therapy or danazol.
Recurrent spontaneous pneumothorax associated with the menstrual cycle, or catamenial pneumothorax, although rare should be considered for all women who present with a pneumothorax during their menses. Korom et al. estimate that up to one third of women with spontaneous pneumothorax may truly have a diagnosis of catamenial pneumothorax. 10 Some of the theories that exist to explain how catamenial pneumothorax occurs are (1) loss of the cervical mucous plug during the menstrual phase leading to air in the peritoneum, which then transverses through the diaphragm into the pleural space; (2) spontaneous rupture of blebs or bullae during hormonal changes; (3) elevated prostaglandins leading to bronchiolar vasospasm and constriction; and (4) metastatic spread of endometrial tissue. 8 Once catamenial pneumothorax is suspected, a video-assisted thoracic surgery to examine the lung parenchyma and diaphragm is the suggested approach. This procedure should be timed with the menstrual cycle, so as to increase the likelihood of visualization of any endometriotic implants present, and any lesions should be excised. The treatment of thoracic endometriosis should entail either suppression or eradication of thoracic endometrial tissue, prevention of reseeding from the pelvis, and prevention of air leakage across diaphragmatic gaps or perforations. Either mechanical or chemical pleurodesis can be performed to cause irritation between the parietal and the visceral layers of the pleura, attempting to close off the space between them and preventing further fluid from accumulating. Unfortunately, there is a high recurrence rate of pneumothorax regardless of treatment modality. However, in an analysis of 110 cases, Joseph and Sahn showed surgical management (pleurodesis) to have a significantly lower recurrence from 6 months onwards. They noted that of 80 patients with pneumothorax, 21 of the 28 patients (75%) treated with medical management and 20 of the 42 (48%) treated surgically had recurrence. 7
Conclusions
This case shows a patient presenting with two rare manifestations of extrapelvic endometriosis, but asymptomatic for pelvic endometriosis. It allows a review of umbilical and lung extrapelvic endometriosis, the theories regarding the etiology of extrapelvic endometriosis, and the treatments available for patients with endometriosis in their lungs, skin, or both. Endometriosis, although predominantly thought of as a gynecologic disease, can afflict patients requiring care with multiple specialists. The case demonstrates the importance of communication and sharing of information between specialties for the good of the patient.
Footnotes
Disclosure Statement
No competing financial interests exist.