
Abstract
Abstract
Introduction
Single incision laparoscopic surgery (SILS) involves using a single 2-cm umbilical incision to access the abdomen by using a specialized SILS port. The SILS port is equipped with three distinct openings: two 5-mm ports and one 5–12-mm port. The positions of these openings are adjustable within the port to allow the use of three surgical instruments at the same time. The obvious benefit of a SILS approach over a traditional LSH is cosmetic. With SILS, the laparoscopic incision is hidden entirely within the folds of the umbilicus.
Although the concept of SILS is relatively straightforward, the unidirectional limitations and the obvious crowding of instruments inherent in this approach increase the complexity of laparoscopic surgery. LSH via a SILS approach also presents another unique challenge: the uterus has to be morcellated through the single umbilical incision. The instruments and techniques used on 4 patients who underwent LSH via a single incision laparoscopy with transumbilical morcellation using a 5-mm transcervical laparoscope, and the operative technique used, are discussed.
Instruments and Techniques
The four procedures were performed using the following instruments and techniques. The patients were placed in a modified dorsolithotomy position. A Foley catheter was inserted. A uterine manipulator was not used. A 1.5–2-cm vertical incision was then made in the center of the umbilicus. Dissection was carried down through the fascia, and the peritoneal cavity was entered using the open Hassan technique. A SILS port (SSL Access System, Ethicon Endo-Surgery, Cincinnati, OH) was placed through the umbilical incision and the abdominal cavity insufflated with CO2 gas. The patient was then placed in steep Trendelenberg position.
A rigid 0° 5-mm extra-long laparoscope was then placed through the SILS port. The surgeon assumed a position between the patient's head and shoulder, allowing the operator to directly face the pelvis while operating. A Harmonic scalpel (Ethicon Endo-Surgery, Cincinnati, OH) was used to bilaterally cauterize and cut the utero-ovarian ligaments, fallopian tubes, and round ligaments. The uterine arteries were skeletonized bilaterally. A peritoneal incision was made just above the bladder in the anterior cul-de-sac. The bladder was reflected inferiorly, just enough to expose the cervix at the level of the internal os.
The uterine arteries were sequentially exposed by severely angulating the fundus laterally in a direction perpendicular to the normal uterine axis. This position exposed the arteries to instruments directed through the umbilical port. The uterine arteries were then cauterized and cut using a bipolar coagulating instrument: Ligasure Advance (Covidien, Atlanta, GA) or Enseal (Ethicon Endo-Surgery, Cincinnati, OH). The arteries were ligated 1–2cm above the level of the internal os. The Harmonic scalpel was then used to cauterize and cut the tissue medial to the uterine artery pedicle. Dissection was carried inferiorly down to the level of the cardinal ligament and below the level of the internal os. A Lina- Loop (Ocean Surgical, Arlington, MA) was placed around the cervix at the level of the internal os. Using unipolar cautery the Lina-Loop was used to amputate the uterine fundus from the cervix. A standard 5-mm trocar was then placed transvaginally through the cervical os into the abdominal cavity (Fig 1). The laparoscope was then placed through this trocar and the umbilical SILS port was visualized. A Storz Rotocut 10-mm morcellator (Storz, Goleta, GA) was placed through the SILS port and the uterine fundus was morcellated under direct vision (Fig 2). Once the morcellation was completed the laparoscope was removed from the cervix and directed back through the abdominal SILS port. Interceed® adhesion barrier (Gynecare, Johnson and Johnson, Arlington, TX) was placed over the cervical stump. An endobag extractor was used to remove the adnexal masses. After hemostasis was assured, the SILS port was removed and the umbilicus was closed in layers. The fascia was closed with a continuous 0 polyglactin 910 (Vicryl) suture and 3–0 polyglactin (Vicryl) inverted sutures were used to re-approximate the superficial layers of the umbilicus (Fig 3).

A standard 5-mm trocar placed transvaginally through the cervical os into the abdominal cavity.
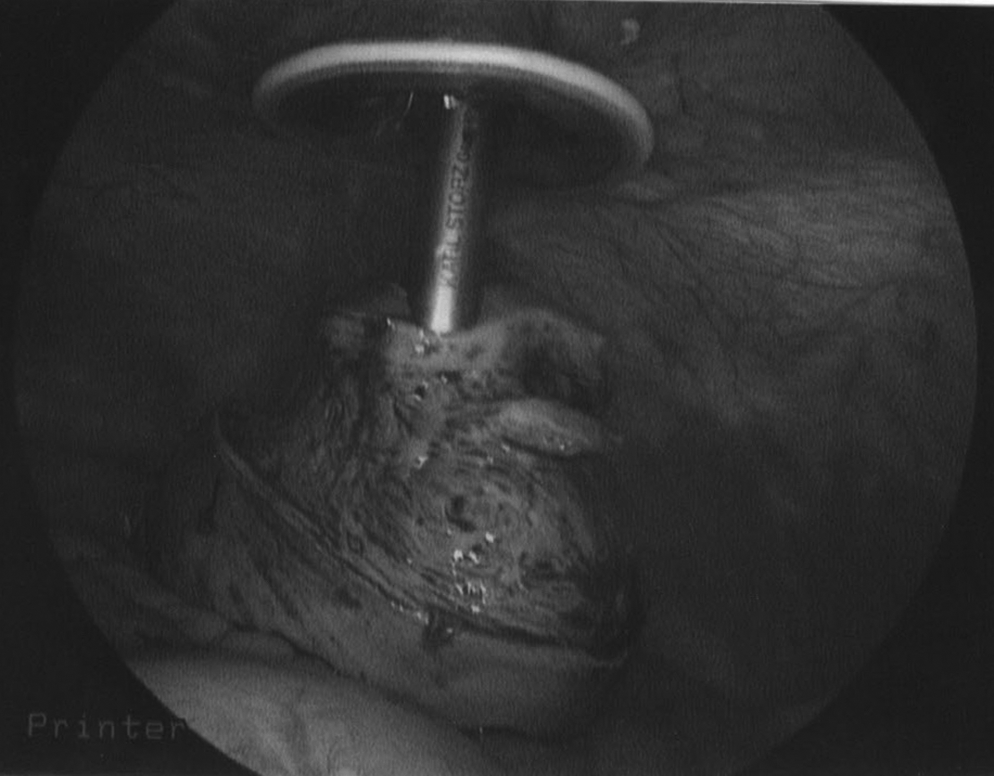
Transumbilical morcellation of the uterine fundus through the SILS port.
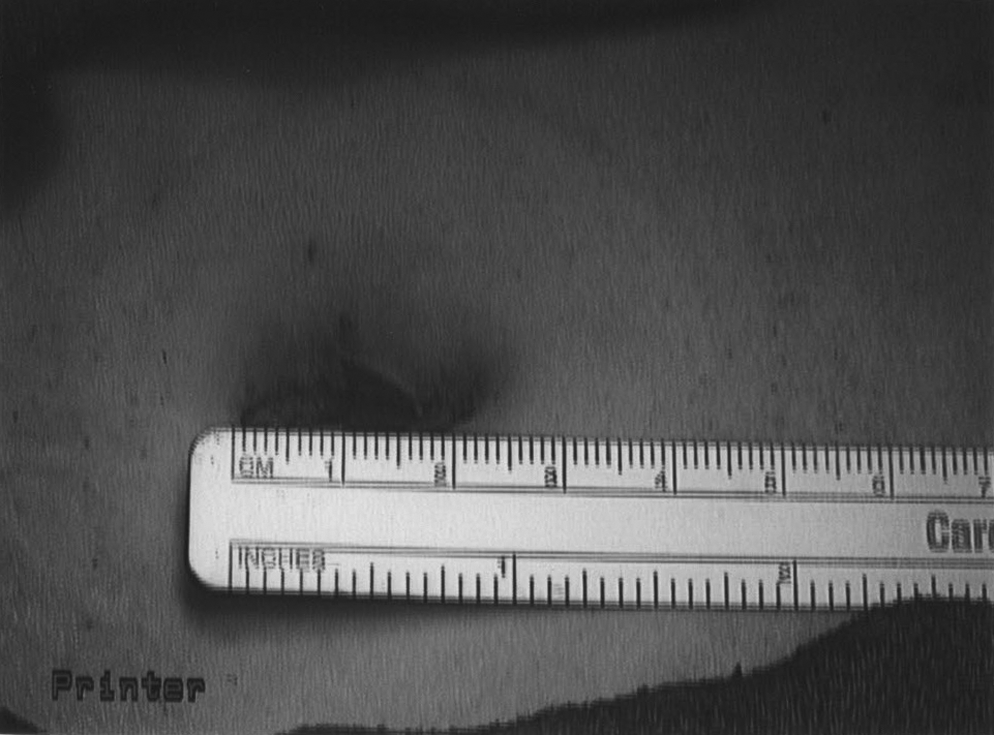
A 2-cm single umbilical skin incision.
Cases
Patient 1 was a 45-year-old gravida 0, para 0, with a fibroid uterus and dysmenorrhea unresponsive to medical therapy. A sonogram demonstrated a uterus measuring 8 cm×7 cm×5 cm with multiple myomas. Her past surgical history included a retropubic transvaginal tape (TVT) and transurethral resection of a primary bladder cancer without any further therapy. Physical examination revealed an enlarged uterus measuring ∼8 weeks' gestational size. Laparoscopy demonstrated an enlarged irregular uterus. Significant scarring and bladder adhesions were noted in the region of the left cardinal ligament. Extensive dissection in this area was required in order to reflect the bladder inferiorly. Cystoscopy was performed to evaluate the bladder. The estimated blood loss (EBL) was 100 cc. Final pathology demonstrated multiple uterine fibroids and a total weight of 87 g. Operative time was 165 minutes and the patient was discharged home in 23 hours.
Patient 2 was a 46-year-old gravida 0, para 0 with a history of stage IV endometriosis and persistent dysmenorrhea unresponsive to medical therapy. Serial sonograms demonstrated multiple small (2–3 cm) persistent left ovarian cysts and a uterus measuring 8 cm×5 cm×5 cm. Physical examination revealed an enlarged uterus measuring 6 weeks' gestational size. Laparoscopy revealed stage IV endometriosis with two left ovarian endometriomas. Dense adhesions were also noted between the left adnexa, sigmoid colon, left pelvic side wall, and posterior uterine fundus. Specifically, there did not appear to be any endometriosis below the level of the uterosacral ligaments. An extensive lysis of adhesions was performed prior to removing the uterus. After the hysterectomy was completed, the left adnexa was removed. The EBL was 50 cc. Final pathology confirmed endometriosis, and the total weight of the uterine fundus was 47 g. Operative time was 117 minutes and the patient was discharged home on postoperative day 2.
Patient 3 was a 38-year-old gravida 2, para 2 with a long history of fibroid uterus, dysmenorrhea, menorrhagia, and anemia unresponsive to medical therapy. A sonogram demonstrated a fibroid uterus measuring 8 cm×6 cm×5 cm. Physical examination demonstrated a uterus measuring 8–10 weeks gestational size. Laparoscopy revealed an enlarged myomatous uterus. During the course of the hysterectomy, and, after ligating the left uterine artery, significant bleeding was encountered while cauterizing the right uterine artery pedicle. The bleeding artery was isolated and controlled with bipolar cautery. The EBL was 400 cc. The weight of the uterine fundus was 147 g, and the final pathology demonstrated multiple uterine fibroids and adenomyosis. Operative time was 152 minutes and the patient was discharged home in 23 hours.
Patient 4 was a 52-year-old gravida 2, para 2 with fibroid uterus, pelvic pressure, and menorrhagia unresponsive to medical therapy. A sonogram demonstrated a uterus with multiple fibroids and a large fundal subserosal fibroid measuring 7 cm×5 cm×5 cm and a left ovarian clear cyst 8 cm in diameter. Physical examination demonstrated a uterus measuring 14–16 weeks' gestational size. Laparoscopy revealed an enlarged myomatous uterus and an 8-cm left ovarian simple cyst. A left salpingo-oopherectomy was performed prior to removing the uterus. The EBL was 100 cc. The weight of the uterine fundus was 400 g, and the final pathology demonstrated multiple uterine fibroids and a benign left ovarian cyst. Operative time was 213 minutes and the patient was discharged home on postoperative day 1.
Discussion
Performing a LSH via a SILS approach involves not only adjusting to the limitations of a single incision, but also requires modifications to the traditional LSH technique. The single incision approach provides relatively easy access to the fundus of the uterus. As a result, the initial steps of a SILS supracervical hysterectomy are not significantly different from a traditional approach. The changes in technique take place at the level of the uterine arteries. The SILS approach requires changes in how the uterine arteries are approached, how the fundus is amputated from the cervix, and how the specimen is morcellated.
In a traditional LSH the uterine arteries are typically ligated by an instrument placed through a lateral lower quadrant trocar. This allows the arteries to be grasped and coagulated in a direction perpendicular to their course on the lateral edges of the uterus. To accomplish an anatomic approach via SILS requires sharply angulating the uterine fundus laterally to expose each uterine artery. Each uterine artery can then be approached from a perpendicular direction with an instrument placed through the umbilicus. However, such an approach results in more tension on the uterine artery pedicle than is traditionally recommended. To accomplish a secure ligation, a bipolar coagulating device is required. This instrument grasps and secures the pedicles while coagulating them, thus preventing premature separation of the tissue before the artery is completely coagulated.
Securing the uterine arteries is the most technically difficult and a potentially hazardous portion of a SILS LSH. Several tips can be helpful. Patience is key. In order to minimize the risk of incomplete ligation, multiple pre-cut burns are made in the pedicle using the bipolar instrument. Using bipolar cautery results in minimal lateral thermal spread. One should start with the most accessible artery. This will minimize back bleeding when securing the more difficult side. The arteries should be ligated 1–2 cm above the level of the internal os. This creates a margin to potentially re-secure a pedicle if bleeding occurs from an artery that is incompletely ligated (as occurred in the third case). This also provides a margin to prevent thermal injury to the ureter. Further dissection is then performed inferiorly and medial to the uterine artery pedicle down to the cardinal ligament. This exposes the lateral cervix at the level of the internal os.
Amputation of the uterine fundus from the cervix is traditionally accomplished from a direction similar to that used for ligation of the uterine arteries. It is performed with unipolar cautery or harmonic scalpel through a lateral lower quadrant trocar approaching the uterus from a direction perpendicular to its axis. Manipulation of the uterus cannot recreate this anatomic relationship and expose the cervix to the umbilicus, as can be done with the uterine arteries. As such, a different approach is required to accomplish amputation of the fundus via SILS.
Amputation could be performed with an articulating instrument using unipolar cautery. However, the Lina Loop provides a simple solution. The loop is essentially a wire endoloop attached to unipolar cautery. The loop is placed through the SILS port and around the uterine fundus. It is secured around the cervix at the level of the internal os. Activation of unipolar current allows the wire to cut through the cervix while simultaneously coagulating the cervical stump.
The final step to completing a SILS LSH is removal of the uterus from the abdomen. In a total laparoscopic hysterectomy (LH) the uterus is removed through the vaginal apex. LH has been performed via SILS. 2 However, total hysterectomy is associated with significantly higher morbidity than supracervical hysterectomy. 3
The biggest limitation of morcellation is that it has to be done under direct visualization. When using a SILS approach this can theoretically be accomplished three ways. A flexible laparoscope with a reticulating camera tip could provide triangulation and potentially enough intracorporeal working space to visualize the morcellation process. Although conceptually possible, the current authors operate with a rigid, straight laparoscope, which precludes that approach. The other two options require a second port and use transvaginal assistance. Yoon et al. describe placing a 15-mm morcellator through the cervix, and morcellating the fundus under direct vision from the umbilicus. After morcellation they sutured the peritoneum over the cervical defect. 4 Alternately, the laparoscope could be placed transcervically and morcellation could occur through the umbilicus.
After considering the options, it was decided that placing a smaller 5-mm laparoscope through the cervix was more desirable than placing a 15-mm morcellator through the cervix. To minimize the risk of bacterial contamination of the laparoscope, a 5-mm trocar should be inserted into the cervix. The trocar head rests outside the vagina, making the trocar a sterile "delivery system" allowing laparoscopic access to the abdomen. By placing a 5-mm instrument through the cervix, the cervical dilation is also significantly smaller than if a 15-mm instrument had been placed. As such, the cervical stump was not sutured in the 4 cases described previously.
Traditionally, the specimen to be removed is stabilized with a grasper and guided into the morcellator. Without additional ports this also becomes impossible. To accomplish morcellation via the umbilicus without assistance, the tissue to be removed should be held in a strict vertical plane using a 10-mm tenaculum while the patient is in steep Trendelenberg position. Thus, when morcellation occurs, the specimen easily spins, is not sheared off prematurely, and is removed in long strips. After removing the larger portions of the tissue, a 10-mm grasper should be introduced and used to pick up the small remaining pieces that may have fragmented during the morcellation. Unassisted transumbilical morcellation via transvaginal visualization is not technically difficult. Although it can be initially disorienting, the learning curve appears short.
The surgical technique described for SILS LSH evolved over 6 months. It was developed as part of a deliberate strategy to gradually reduce the number and size of the accessory ports needed to perform an LSH. Multiple puncture sites increase trocar-associated complications, such as pain, bleeding, hernias, and wound infection. Furthermore, the cosmetic results are not as optimal. This article reports the first cases of LSH-SILS with transumbilical morcellation, and the surgeries demonstrate that the presence of adnexal pathology, pelvic adhesive disease, or even a large fibroid uterus does not preclude a single-incision approach. The operative times compare favorably to those of the traditional approach to LSH. Although a pure single incision approach is not yet feasible for every LSH, these techniques can be used in every hysterectomy to decrease morbidity by minimizing the size and number of accessory trocars. Many of the hysterectomies performed by the authors over the last 6 months have been accomplished via a "modified" SILS approach. These surgeries used a single incision approach and added one 5-mm accessory trocar in the lower abdomen.
The tools for SILS will certainly improve. New and improved multichannel SILS ports will facilitate the single incision approach for all gynecologic procedures. New articulating tools and more ergonomic instruments are also being developed. An articulating bipolar coagulating device would certainly facilitate performing an LSH. It would make ligation of the uterine artery pedicles easier and more reliable. As instrumentation improves, LSH via SILS will certainly become more common, especially among experienced laparoscopists. These cases, and the techniques reviewed, demonstrate that LSH via SILS is feasible and can be safely performed using current technology and tools.
Footnotes
Disclosure Statement
Dr. Wagner is a consultant to Ethicon Endo-Surgery.