
Abstract
Abstract
Introduction
Case
A 74-year-old woman (gravida 3, para 1, with one spontaneous delivery and two first trimester abortions) sought medical attention because of a large adnexal tumor with mainly cystic appearance that had been followed up by sonography in the past at another hospital, and now caused pressure on the urinary bladder causing worsening incontinence. The patient had no other symptoms, in particular no vaginal bleeding. By gynecologic palpation and transvaginal sonography, a leiomyoma or a leiomyosarcoma of the uterus was suspected. As an adnexal tumor could not be ruled out, MRI scanning was performed, MRI imaging with the following sequences was done: sequence T2 SPAIR (spectral adiabatic inversion recovery) (transversal), sequence T2 TSE (turbo-spin echo) (transversal, sagittal), sequence T1 TSE (transversal before and after contrast), and sequence T1 SPAIR after intravenous contrast injection. The T1- and T2-weighted MRI imaging of the pelvic without contrast and the T1-weighted MRI imaging after injection of gadolinium-containing contrast agent showed a lesion, measuring 90×50×60 mm in size, which appeared to fill the uterine corpus entirely. The tumor was smooth and surrounded by a thin uterine wall, seen in the T1-weighted imaging because of the high enhancement of the dense uterine wall. The T2-weighted MRI image further showed a hyperintense mass with a hypointense predominantly fatty component of the tumor (Fig. 1) with compression of the urinary bladder. A pedunculated part of the tumor was clearly seen at the posterior side of the uterus, suggesting a uterine origin.
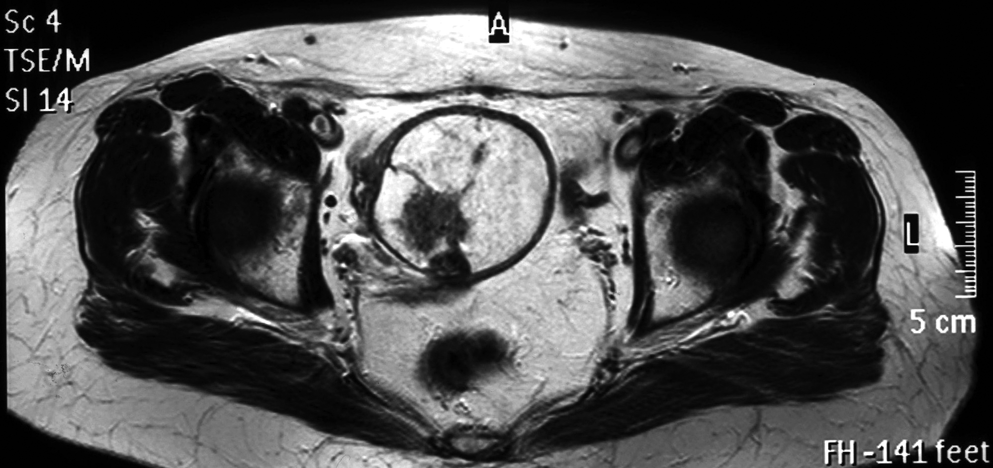
Axial spin-echo, T2-weighted MR image shows a 60×50 mm, sharply demarcated tumor of the uterine corpus.
A diagnostic curettage was performed, which revealed regular mucosa of the cervix and the uterine transition zone and parts of an intramural lipoleiomyoma (smooth fibers of muscle cells and mature fat cells). On laparoscopy, both ovaries appeared normal and the uterus was significantly enlarged. Finally, the tumor was removed by total hysterectomy with bilateral salpingo-oophorectomy. The postoperative course was without any complications, and the patient was discharged on the fourth postoperative day.
Macroscopic investigation showed a uterus with both ovaries (198 g) and corresponding cervix. The uterine cavity was filled out by a lipomatous tumor (90×50×60 mm), originating at the posterior uterine wall. The remaining wall was dilated by the tumor to the size of a thin-walled capsule (Fig. 2). Microscopically, both ovaries (10 mm in size) with fimbria and tubes showed no histologic abnormalities. The lipomatous tumor of the uterus consisted partly of smooth muscle cell bundles, but mainly of homogenous mature univacular adipocytes. There was no nuclear polymorphism or any mitotic activity (Fig. 3). Immunohistochemically, the tumor strongly expressed desmin and progesterone receptor. The CD10 reaction was entirely negative excluding a uterine stromal tumor. A very low Ki67 nuclear index (<0.1%) indicated an extremely low proliferation rate.
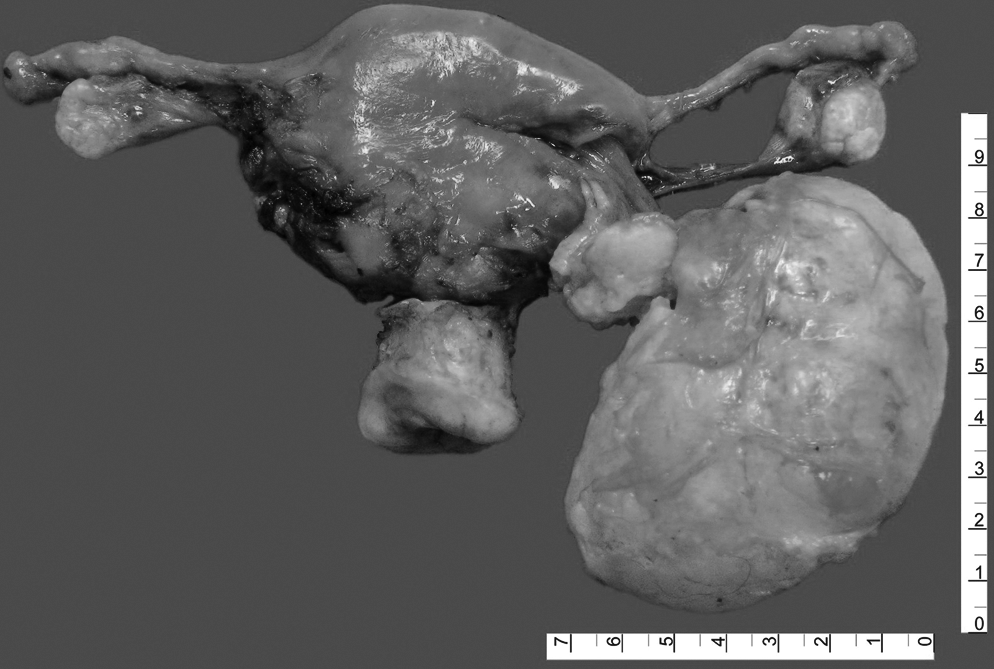
Gross appearance of the lipomatous tumor after incision of the uterus. Note the pedunculated origin from the posterior uterine wall.

Microscopic finding of the lipoleiomyoma (hematoxylin-eosin, original magnification x 25). The tumor consists of smooth-muscle cells and mature univacuolar adipocytes.
Discussion
Lipomatous tumors can be divided into three groups. 1 Pure lipomas consist exclusively of mature fat cells and a characteristic chicken wire-like capillary network. Histologically mixed tumors, including lipoleiomyomas, 1 angiomyolipomas, 2 fibromyolipomas, 3 and osteolipomas are rare tumors composed of different mesodermal components such as mature fat tissue, smooth muscle tissue, connective tissue, or bone, respectively. These two tumor groups are strictly benign and because of their noninvasive nature, reveal a sharply demarcated surface. The third group of the different entities of liposarcomas, 4 consists of tumors with malignant or dedifferentiated fat cells, which grow locally invasive and potentially metastasize.
Lipoleiomyomas are rare benign tumors with an incidence of 0.03%–0.2 % in utero,5,6 which are diagnosed most frequently in postmenopausal women between 45 and 70 years of age.1,5 The histogenetic origin of uterine lipoleiomyomas is still unclear, and is debated in the literature. Some authors suggest differentiation of misplaced embryonic adipocytic or stromal mesenchymal cells. Other authors favor direct metaplasia of smooth muscle cells, proliferation of accompanying perivascular fat cells into the blood vessels, embedding of fat cells into the uterine wall during an operation, and a fatty infiltration or degeneration of the connective tissue.5,7–10 It has also been suggested that lipoleiomyomas develop from an omnipotent undifferentiated mesenchymal cell. 9 Histopathologic studies showed that the lipoleiomyoma may also derive from an in-utero pre-existing myoma caused by lipomatous metaplasia. 11
Studies of extrauterine tumors suggested that in some cases gene defects [12q15 (40, 41) (HMGA2)], which also exist in lipomas, are responsible for the development of a leiomyolipoma and hence, leiomyolipomas represent a genuine neoplastic entity. 12 However, the authors of this article propose that extrauterine and uterine lipoleiomas represent entirely different entities and that data derived from extrauterine tumors cannot be transferred to uterine tumors. This case strongly suggests the pre-existence of a pedunculated progesterone-positive benign uterine leiomyoma, which underwent lipomatous degeneration and metaplasia because of insufficient blood supply though the pedunculated connection to the blood circulation. It is well known that muscle tissue can undergo lipomatous degeneration in cases of malnutrition. Consistently, malignant transformation of lipoleiomyomas has never been reported in the literature.
Conclusions
In summary, the differential diagnosis of leiomyolipoma includes angiomyolipoma, fibromyolipoma, and other benign mixed fatty tumors and the exclusion of a low-grade sarcoma. Furthermore, fibroma, benign pelvic lipoma, pelvic fibrolipomatosis, benign ovarian mature cystic teratoma, extra-adrenal myelolipoma, lipoblastic lymphadenopathies, and retroperitoneal cystic hamartoma have to be excluded.1,6,13,14 MRI appears to be the best method for diagnostic differentiation. In contrast to leiomyomas, which demonstrate distinct low signal intensity relatively to the myometrium, uterine lipoleiomyoma is characterized by an abundance of fat tissue. 15 The tumor is usually a well-demarcated mass that is hyperintense with hypointense amorphous areas on T1- and T2-weighted MR images. The MR images may be variable depending upon the volume of mesodermal tissue such as fat, muscle, connective tissue, and stromal degeneration. Therefore, in rare cases with a small percentage of fat tissue, the diagnosis may be difficult and demands different MR imaging variations such as STIR (Short-Tau Inversion Recovery) and chemical shift images to demonstrate the small fat components indicated by chemical shift artifacts within the lesion.16,17 Fat suppression MRI sequence enables the differentiation of fat tissue from hemorrhage in uterine leiomyosarcoma, as well.16,17
Although lipoleiomyomas are strictly benign tumors, complete surgical excision seems reasonable to rule out the presence of malignant uterine sarcomas and liposarcomas, which cannot be accomplished entirely by imaging studies.
Footnotes
Acknowledgments
The authors thankfully acknowledge the support of the German Sarcoma Reference Center by the Deutsche Krebshilfe to R.B. (grant 107193).
Disclosure Statement
No competing financial conflicts exist.