
Abstract
Abstract
Introduction
Laparoscopic tissue acquisition remains, nevertheless, troublesome, in particular as more high-quality tissue needs to be harvested to comply with the increasing demands of laboratory tests. The introduction of targeted therapies, often based on thorough molecular diagnostics and the pleas for more individualized treatments, make tissue examination a key factor in achieving complete diagnosis. Modern diagnostic techniques require specimens of high quality, meaning sufficient sample volume of representative diseased tissue must be obtained without contamination from other tissues and blood.
Traditional laparoscopic biopsy accessories include punch forceps, and this biopsy tool harvests only superficial samples of the target with a maximal depth of 1 mm. This serious shortcoming precludes further extension of the indications for laparoscopic diagnosis. Acquisition of a representative large sample for all anticipated diagnostic tests remains a challenge. This is particularly true for sites that are difficult to access, for dense tissues and for deeper structures. Some organs can be too slippery to hook and may be difficult to access with most forceps. The Palmer variation of forceps (United States Patent 5482054) seems more appropriate for this procedure, but the sample size and crushing artifacts are difficult to predict.
The new ENDO version of the Spirotome (Medinvents nv, Hasselt, Belgium) a direct and frontal (D&F) type of biopsy instrument, is specifically designed to address the disadvantages of traditional tools. The Spirotome ENDO is able to grip the target lesion by hooking it up at an angle, preventing the structure or organ from slipping away during penetration. The sample size is ∼200–300 mg, and targeting is extremely precise. The D&F concept of tissue acquisition seems to be an ideal accessory for laparoscopic exploration in oncologic diagnosis and staging.
Spirotomes have been extensively studied in animals2,3 and various human pathologies.4,5 Experience, efficacy, and safety were demonstrated in a study of 173 women, each with a suspicious breast lesion. 6 In addition, the technology proves to be highly accurate for removal of small clusters of microcalcifications 7 from the breast, indicating the precision for targeting small lesions. D&F tissue harvest under hysteroscopy and colposcopy guidance is rapidly emerging, and major gynecologic centers have adopted the system for a variety of ambulant oncologic and infertility applications. 8 * Finally, the technique has been used successfully in the exploration of metabolic diseases of the liver under laparoscopic guidance. 9
This article describes, for the first time, the utility and feasibility of the Spirotome ENDO, used in 4 cases, as an important adjunct to laparoscopic exploration of the abdomen in the field of gynecology.
Materials and Methods
The Spirotome ENDO
The Spirotome ENDO (MedInvents NV, Belgium) set contains three elements: (1) the cutting cannula or outer sheath: (2) the receiving needle that contains the helix: and (3) a plastic release element. The set is autoclaved before use or is available sterile in single-use sets (Fig. 1).

The Spirotome ENDO set (Medinvents nv, Hasselt, Belgium).
In Figure 1A, the two parts of the needle are presented. The outer cutting cannula (on top) is a hollow tube with a distal cutting end and a proximal knob. The receiving needle (underneath) is also a hollow tube with a distal helix cut from the wall of the tube and a proximal knob. Both needles are mounted before the procedure and inserted into the abdomen under laparoscopic vision. The helix penetrates the tissue by rotating the needle; for cutting the sample, both cannula and helix work together.
The plastic release element (Fig. 1B) helps to retrieve the sample from the helix with minimal injury to the sample. The helix (with sample) is placed in the sleeve that contains teeth to hold the sample. The helix is rotated counterclockwise to release the sample. After release, the sample can be cut into mirror samples to provide different laboratories with identical materials. The sample is immersed in an appropriate solution (e.g., formalin, RNAlater), depending upon the purpose, and adequately labeled.
The helix is the main feature of the device (Fig. 2). This helix, being cut from the wall of the tube that constitutes the receiving needle, has a body in the shape of a parallelogram in transverse section. The dimensions of that parallelogram are 1.2 mm in length and 0.5 mm in thickness (the thickness of the tube). The shape of the body of the helix creates the cutting edges that work in conjunction with the cutting cannula. The creation of a stable flat helix has been made possible by recent laser innovations and dedicated diamond grinding (Fig. 2).
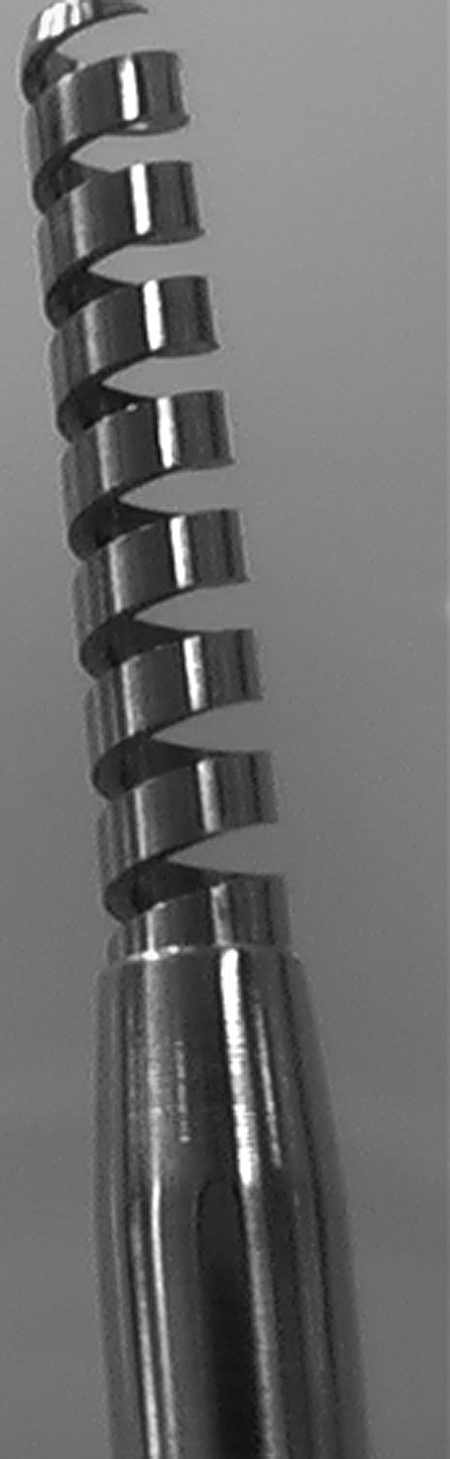
The Spirotome ENDO (Medinvents nv, Hasselt, Belgium)distal part.
Operational features of the Spirotome ENDO
The penetration of the helix into the diseased tissues occurs by turning the needle clockwise. Although the body of the helix has a diameter of only 1.2 [[[times sign]]] 0.5 mm, the penetration is quite comparable to that of a fine subdermal injection needle, causing minimal damage to the organ. The navigation features of the helix have several advantages. Positioning is precise, and the correct direction and position of the helix point can be under continuous imaging and/or laparoscopic control. Because one turn of the helix equals 2 mm, the depth of penetration can be visualized and monitored during laparoscopy.
When depth of penetration and position are satisfactory, the outer cutting cannula is turned clockwise over the helix to free the specimen from the surroundings. The completeness of cutting can be visualized on the proximal end of the instrument: Two marks reflect the position of the outer sheet tip in relation to the helix. Once cutting is complete, the inner needle is removed with the sample.
Tissue damage tends to be minimal or absent and the laparoscopic image remains unchanged without blurring, which may occur in the event of bleeding. The sample is protected during and after cutting inside the helix. Penetration varies between 5 and 20 mm and by virtue of its D&F approach, penetration can be even deeper by taking many samples. Each sample remains in the helix when retracted from an organ, because tissue fibers keep the sample inside the helix. In addition, the sample stays in the helix when the instrument is removed from the abdomen, preventing the sample loss that often occurs with forceps instruments.
The Spirotome ENDO during laparoscopy
D&F tissue acquisition is rather straightforward. Under laparoscopic vision, the point of the helix approaches and penetrates the target area. The most practical diameter of the cutting cannula (outer sheet) is 5 mm. The depth of the sample ranges from three to 20 mm depending upon the clinical needs involved.
Possible bleeding can be managed rather easily if necessary by unipolar coagulation on the instrument (medical-grade stainless steel with plastic trocar). Alternatively, bipolar coagulation is applicable as well through a variant design of the instrument. However, simply leaving the outer sheet (cutting cannula) in place for some moments will stop most bleeding, as collateral damage is minimal or absent. In this feasibility study, there was no need for electrocoagulation.
Patients
For this feasibility study, 4 female patients with abdominal disease, either benign or malignant, were given informed consent forms according to the protocol of the ethical committee of the Hospital Oost-Limburg (Identification Number 01/041 of November 15, 2001) in the Netherlands, entitled: “A phase I clinical trial for testing the performance of the Spirotome.” After being accepted to enter the study, the patients were admitted to the hospital's gynecologic department. Two patients presented with uterine bleeding abnormalities (menorrhagia), 1 patient had ovarian pathology that was suspicious for cancer, and 1 had pain and with a suspicion of ovarian pathology.
A summary of the patient characteristics is presented in Table 1.
Preparation of the patients was traditional and the procedures were all performed under general anesthesia. Surgery was documented through camera and video imaging, and efficacy and safety characteristics (bleeding, complications) were recorded during and after laparoscopy in the medical research file. The operator judged the performance of the equipment, and the pathologist judged the quality of the tissue material.
Results
In this feasibility study, the D&F approach of tissue acquisition during laparoscopic exploration was evaluated for use in benign diseases and oncologic staging.
Performance of the Spirotome ENDO during laparoscopy
Deep biopsies from different tissues, such as the uterus, ovaries, peritoneal implants, and masses were taken. One myoma of the uterus was explored. Laparoscopic evaluation was possible, and abundant malignant peritoneal tissue was observed in 1 patient. In this case, complete debulking did not seem to be indicated, and neoadjuvant treatment was scheduled. In summary, biopsies were taken with the Spirotome ENDO from peritoneal-cancer implants (Fig. 3), myoma uteri (Fig. 4), uterus (Fig. 5), and ovaries (Fig. 6). Eleven samples were shipped to the hospital's pathology department.
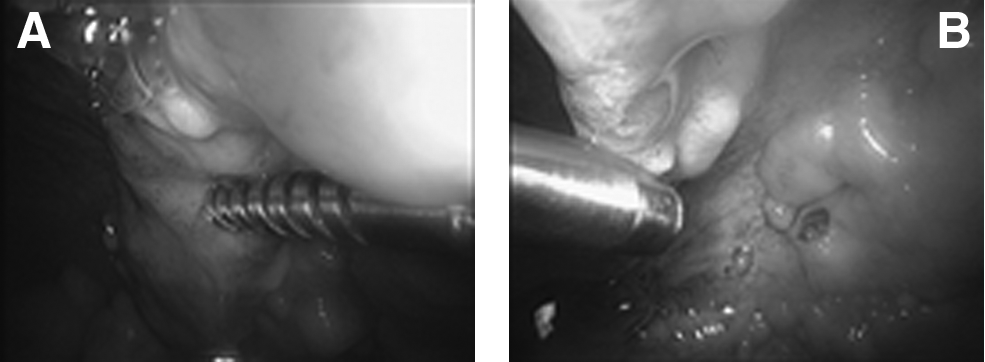

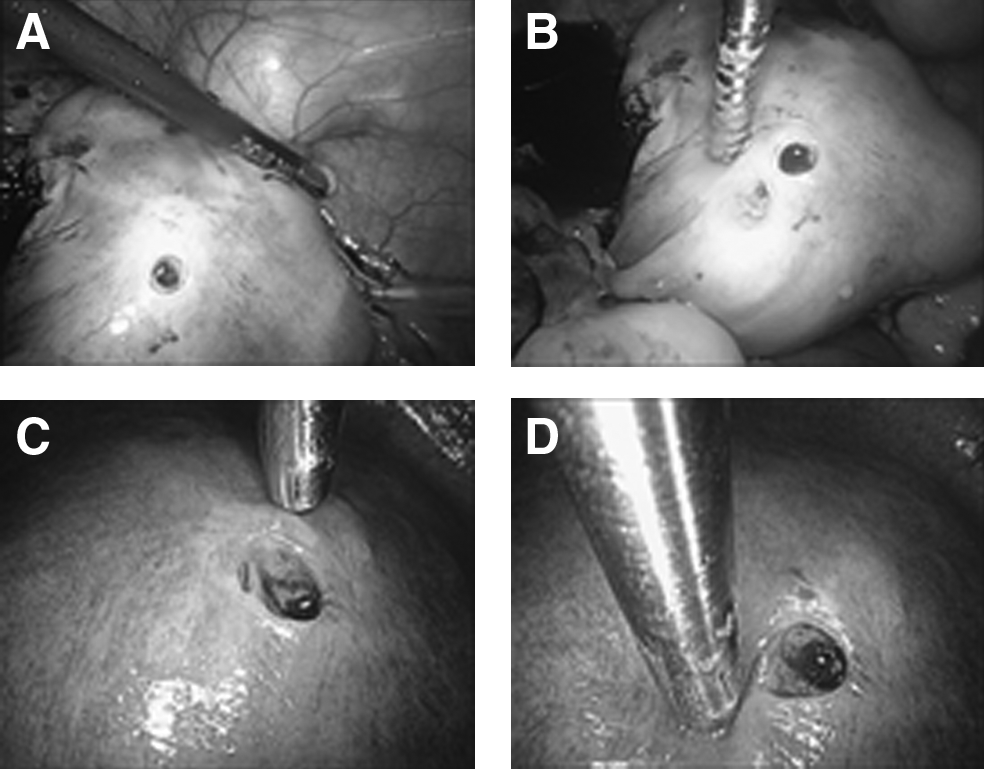
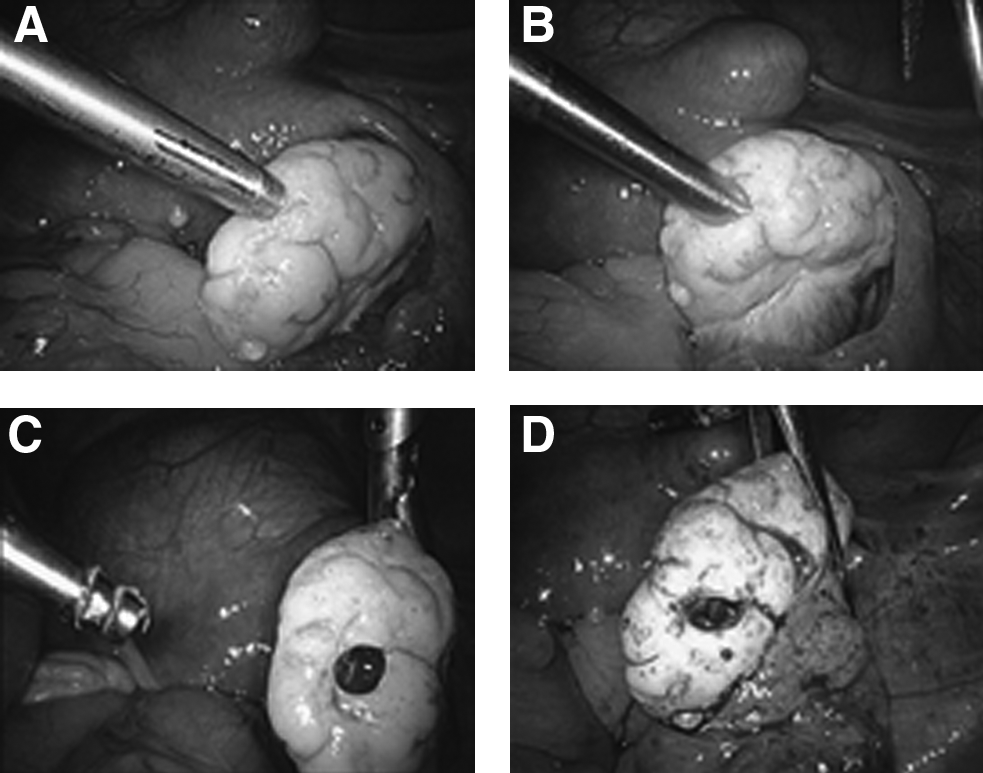
As shown in Figsures 3–6, the biopsy procedure can be monitored easily under direct vision. Penetration is initiated by hooking the point of the helix into the smooth surface of the organs. The depth of penetration is controlled by visualizing the helix turns (one turn is 2 mm). There is no collateral damage. None of the samples was lost during the procedures.
Sample quality
The samples were evaluated macroscopically. Each of the biopsies resulted insamples of various length, depending upon the anticipated depth of the biopsy. The samples were immersed in formaldehyde for pathologic evaluation. It was possible to prepare mirror samples from the original samples captured on the plastic release element of the Spirotome ENDO. The samples were then cut in length so that the pathology and molecular biology laboratories received identical samples. At this research stage, however, no mirror sample was taken for molecular biology analysis.
Safety
No abnormal bleeding or other types of complications were observed during and after the Spirotome ENDO procedures. Patients did not mention side-effects other than the usual abdominal-wall irritation that occurs after explorative laparoscopies.
Histologic verification
Histologic examination of the samples from patient 1, mostly 3–4 mm in diameter and 5–12 mm in length, showed, unequivocally, an “extraovarian type” of serous ovarian cancer. All samples showed extensive presence of cancer cells. The cancer cells lay in clusters and lines without glandular differentiations. Some fields showed pseudoglandular structures in a few areas. The malignant cells were slightly eosinophilic with generally only poorly demarcated cytoplasm. Some of the cancer cells had open cytoplasm with clear cell borders. The nuclei were polymorphic and hyperchromatic and had distinct nucleoli in some parts. The cytoplasm contained granular materials. Immunohistochemical analysis showed a strong positive membranous CA-125 reaction. In addition, cytokeratine 7 and WT1 were positive, suggesting a cancer of ovarian origin. An estrogen-receptor assay showed variable positive staining of the nuclei. A D2-40 test showed a relatively strong reaction around the clusters with cancer cells but not in the individual cancer cells. Calretinin and keratin 20 were negative. At this stage of evaluation, no quantitative molecular biology tests were requested.
For the samples from patients 2, 3, and 4, all diagnostic information that was anticipated and needed was obtained. This means that not only was differentiation achieved between malignancies and benign tissues but that all tests, including pathology, immunohistochemistry, and molecular biology, could be performed on tissues obtained if needed. In other words, there appeared to be no difference between the Spirotome ENDO samples and samples obtained from open surgery. The size of the samples from the Spirotome ENDO typically are 20 mm long and 4 mm in diameter. These dimensions are particularly useful for rapid fixation in formaldehyde or salt solutions and offer better specimen quality for laboratory exploration, because they have been taken by the surgeon in the center of the clinically relevant area.
Discussion
D&F tissue acquisition instruments as an adjunct to laparoscopic exploration of the abdomen perform well with regard to efficacy and safety. Efficacy relates to sample size and purity. Samples should provide information that is comparable to those from diagnostic surgery. In addition, mirror samples should guarantee that the pathologist receives the same quality and type of samples as the molecular biology laboratory.
Mirror sample(s) for the pathology laboratory are immersed in formaldehyde, which is traditional for the ISALA Klinieken.Other types of fixation solutions might be applicable, depending upon institutional policies. The mirror sample for quantitative molecular biology can be immersed in RNAlater, 10 an ammonium-sulfate-based salt solution that makes complicated rapid freezing, liquid nitrogen, and/or dry ice unnecessary for RNA based polymerase chain reaction and microarray analyses. Fresh tissues for molecular biology remain without degradation in this solution for days, and this allows uncomplicated transport to the laboratory. Alternatively, the samples might be stored in a standard freezer (−20°C) for long periods; an unproblematic way to create tissue banks.
Pathologic examination of the tissues confirmed the quality of the samples. Complete histologic diagnosis was achieved on each sample. Although no molecular biology data are described in this feasibility study, the representativeness and volume of the samples guaranteed useful molecular data, as has been observed in similar studies in other organs. 6
The safety of the Spirotome has already been demonstrated to be excellent in breast, lymph node, thoracic wall, abdominal wall, liver, and head and neck biopsies. The experience in this study seems to confirm previous data. There were no complications. Bleeding was almost nonexistent, and any bleeding that did occur was quite manageable through electrocoagulation. A learning curve for this technology has to be considered, as new laparoscopists might feel uncomfortable with new instruments. However, five biopsies, on average, should be sufficient training for most operators. 2
Conclusions
This feasibility experimental study demonstrates that laparoscopic exploration of the abdomen with D&F biopsy tools is quite possible, and encouraging. The technology could offer important new opportunities for patients with abdominal diseases for which no therapeutic, as opposed to diagnostic, surgery is considered and for which deep biopsies are requested for pathology and molecular biology. More clinical comparative trials between open surgery and Spirotome ENDO assisted laparoscopy are justified to confirm these promising preliminary data.
Footnotes
Acknowledgments
The author thanks the operating theater staff and pathology department for help in this feasibility study, and the patients who accepted evaluation of the new technology during stressful moments. The author also thanks Richard Harries, MD (Diana, Princess of Wales Hospital, Northern Lincolnshire, and Goole Hospitals NHS Trust, Scartho Road, Grimbsy, United Kingdom), for critically reviewing the manuscript.
Disclosure Statement
No competing financial conflicts exist.
*
Campo R, Gordts S, for the European Academy for Gynaecological Surgery. Use of the Spirotome Endo in hysteroscopic applications. Manuscript submitted Eur J Gyn Surg.