
Abstract
Abstract
Introduction
Case
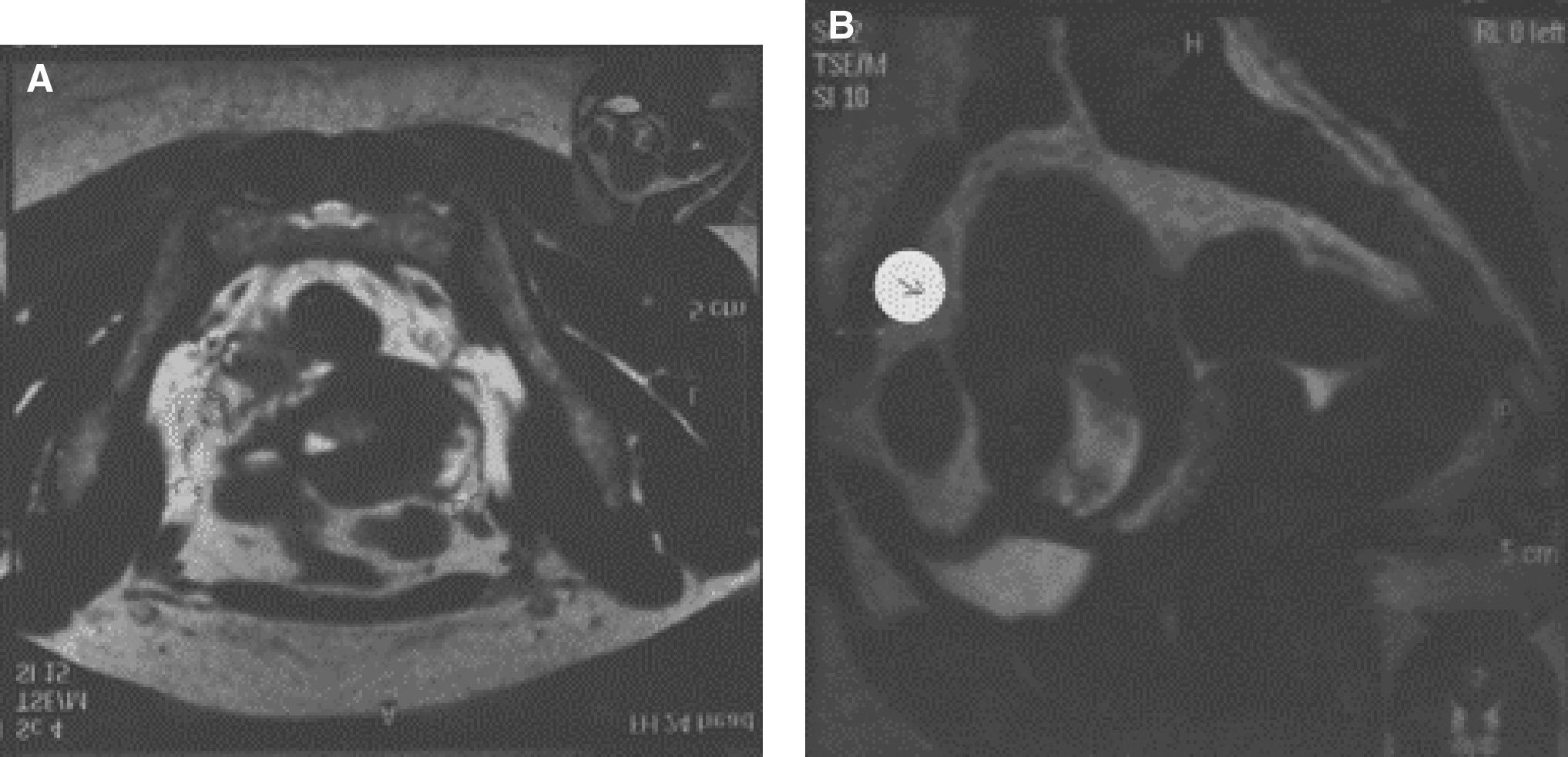
A 31-year-old woman, gravida 6 para 4+1, had one early miscarriage managed by a conservative medical treatment and previous four lower-segment cesarean section deliveries. She had a history of two intrauterine device (IUD) applications, and her fourth pregnancy occurred with the IUD in place. After 6 weeks of amenorrhea, the patient experienced vaginal bleeding for which she sought medical advice at a private medical center. She was diagnosed with incomplete abortion, and uterine evacuation was performed on the same day. After the evacuation, the bleeding stopped, but the lower abdominal pain persisted. She was treated with antibiotics and analgesics for 1 week. She was referred to this clinic when she developed low-grade fever, dysuria, and dyschezia in addition to the prior persistent lower abdominal pain. Clinical examination revealed a young, woman of average build. Her vital signs were stable. Abdominal examination reveal marked tenderness that was more prominent at the site of the cesarean sections scar. Pelvic examination was very painful. A small cystic bulge was palpable on the lower anterior wall of a retroverted bulky uterus. Transvaginal ultrasongraphy revealed that there was an eccentric 7 weeks' gestational sac with fetal pole and no visible cardiac pulsation. The gestational sac was situated low toward the isthmic region of the uterus, but it seemed to be imbedded within the myometrium rather than the endometrial cavity, which was clearly seen to be empty except from some clotted blood. The cervix was closed and its endocervical canal was clear (Fig. 1). Color Doppler (shown in black and white) showed markedly increased peritrophoblastic flow around the gestational sac (Fig. 2), which raised the possibility of cesarean section scar ectopic pregnancy. MRI was performed by saggital and axial T2W1, which revealed a well-defined cystic mass measuring ∼2×1.5 cm, seen within the lower segment of the anterior uterine wall over the isthmic region. The anterior myometrium was thinned and bulged out (Fig. 3a). An abnormal linear hyperintense signal ∼20 mm in length and 4 mm in width was seen crossing the lower anterior myometrium anteroposteriorly on sagittal T2W1 view denoting dehiscence of the cesarean scar (Fig. 3b). The patient refused medical management with methotrexate, but she accepted surgical management, and opted for laparotomy for excision of the scar pregnancy. Intraoperative findings confirmed the preoperative clinical diagnosis. The lower uterine segment was thinned and bulged over the sac, and the scar was dehiscent. No invasion of trophoplastic tissue to the urinary bladder was detected, and the endometrial cavity was opened and curettage was performed. The surgery was accomplished without complications. Postoperatively, the patient remained afebrile, and the recovery was uneventful.

Transvaginal ultrasongraphy showing an eccentric 7 weeks' gestational sac with fetal pole could be detected with no cardiac pulsation in the isthmic region within the myometrium, which is seen all around. Note that the endometrial cavity and the endocervical canal are empty.

Color Doppler showed markedly increased peritrophoblastic flow around the sac. Shown in black and white.
Discussion
A cesarean section scar pregnancy is considered to be more life-threatening than placenta previa or accreta because of its invasion of the myometruim in the first trimester. 3 It has a high risk of bleeding and rupture, which may necessitate hysterectomy. However, it appears to be very rare, although the reports of such pregnancies have grown in the last few years, possibly as a result of increasing number of cesarean sections, new reproductive techniques, and improved diagnosis and methods of early detection. The diagnostic criteria for such pregnancy are: 1) an eccentric gestational sac within the anterior myometrium at the site of cesarean section scar; 2) empty uterine cavity and cervical canal; 3) thinned or absent myometrium at the scar between sac and bladder; 4) color Doppler shows marked peritrophoblastic flow around the sac. 4 Successful medical treatment has generally used local and/or systemic methotrexate, because of its reported efficacy in tubal pregnancies; however, it is associated with prolonged vaginal bleeding that can last for months, and there is also a risk of infection and sepsis. It can be combined with a feticidal agent such as potassium chloride.
Conclusions
Cesarean section scar pregnancy is considered to be an extremely rare condition. Transvaginal ultrasongraphy is the initial step in its diagnosis; however, Doppler ultrasongraphy and MRI are crucial tools for confirmation of the diagnosis. In order to avoid the associated morbidity and mortality of this rare condition, surgical intervention should be considered as first- line therapy. It offers the patient a good outcome and recovery.
Footnotes
Disclosure Statement
No competing financial conflicts exist.