
Abstract
Abstract
Introduction
Materials and Methods
Patient selection
Reproductive-age women desiring permanent sterilization without a history of prior tubal surgery were approached for this trial. Study approval was granted by the Institutional Ethics Committee of the Women's Specialty Center in Dallas, TX. Patients of reproductive age desiring permanent sterilization presenting from March 2007 to December 2009 were offered an Essure® (Conceptus, Inc.) hysteroscopic tubal occlusion in-office under deep lower uterine (paracervical) block. Those accepting the Essure procedure were recruited for study participation. After successful bilateral microinsert placement, patients participating in the study returned for in-office transvaginal sonography (pro-bono) at 10–12 weeks postinsertion for microinsert localization. After the sonographic evaluation, study patients were then referred within the following 1–2 weeks for radiologist performance of the Essure HSG confirmation test per the FDA's requirement. Nonqualifications for Essure placement included 4 : (1) history of prior tubal surgery; (2) a stated allergy to nickel/contrast media; and (3) patients who were <6 weeks postpartum.
All patients were pretreated with 10 days of oral medroxyprogesterone acetate (1 pill twice a day) for the immediate 10 days preceding the Essure (ESS 305) procedure date. The procedure was performed on day 10. Patients who were taking Depo Provera were not given the oral premedication. Patients taking oral/transdermal/transvaginal contraception were advised to stop their current contraception at the time of oral premedication with medroxyprogesterone acetate and to use spermicidal agents with condoms for the 10 days of premedication. All patients had a urine pregnancy test immediately before the Essure attempt. Those with active vaginal bleeding on the day of procedure were rescheduled for the attempt.
On the day of the procedure, patients received preoperative toradol (60 mg, (divided 30 mg IM/30 mg SL) and acetamenophen/hydrocodone (5/500 1 p.o. × 1). All medications were given within 30 minutes of the procedure. A deep parametrial block was used, consisting of 30 mL of 1% mepivacaine without epinephrine, mixed with 20 mL of injectable saline. Ten milliliters (10 mL) were injected at each of the 4/8/2/10 o'clock positions at the cervicovaginal reflection. A 1.5″ needle was used connected to a 6″ needle extender and a 10-mL syringe.
A Wolf hysteroscope (5.5-mm outer sheath diameter, 30°) was used. It was connected to a video display monitor, and lactated Ringer's solution was the hysteroscopic distension medium used. The Essure microinserts were applied in compliance with the user guide recommendations. 4
Contraception was ensured for the first 12 weeks.
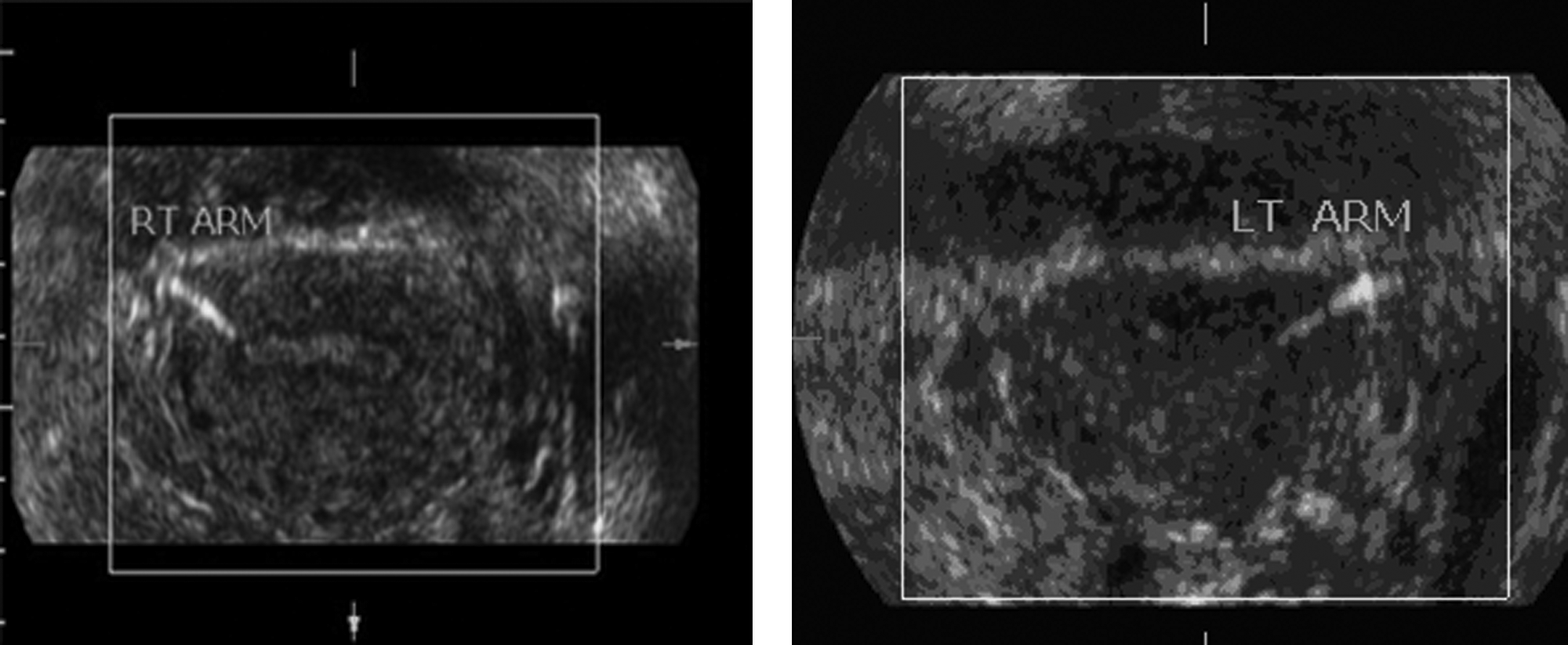
At the time of ultrasound examination (with Phillips TV 7.5 MHz device), a fundal transverse image depicting each microinsert arm was also captured (Fig. 1). The “desired” setup of each microinsert was to have the proximal end of the arm abutting the endometrial lining with the distal arm length transversing the myometrial thickness. This was thought to ensure insert location across the uterotubal junction. Patients whose placements sonographically did not meet that criteron, but who had both implants still clearly within the tubal region, were classed as having an “other” location. A magnification view of each insert at each cornua was then captured (Fig. 2). Patients with only one microinsert identified sonographically were to have a scout X-ray before HSG completion if two inserts had, in fact, been placed initially. All sonogram patients then were referred to have Essure confirmation tests to be completed by a trained radiologist at an outlying community diagnostics center. HSGs were to be interpreted as per preexisting Essure confirmation test guidelines 5 (Fig. 3).

Right and left inserts noted at each cornual area, with the proximal end abutting the endometrial lining, and with insert length transversing the myometrial thickness.
Magnification views of each insert arm per cornual region.
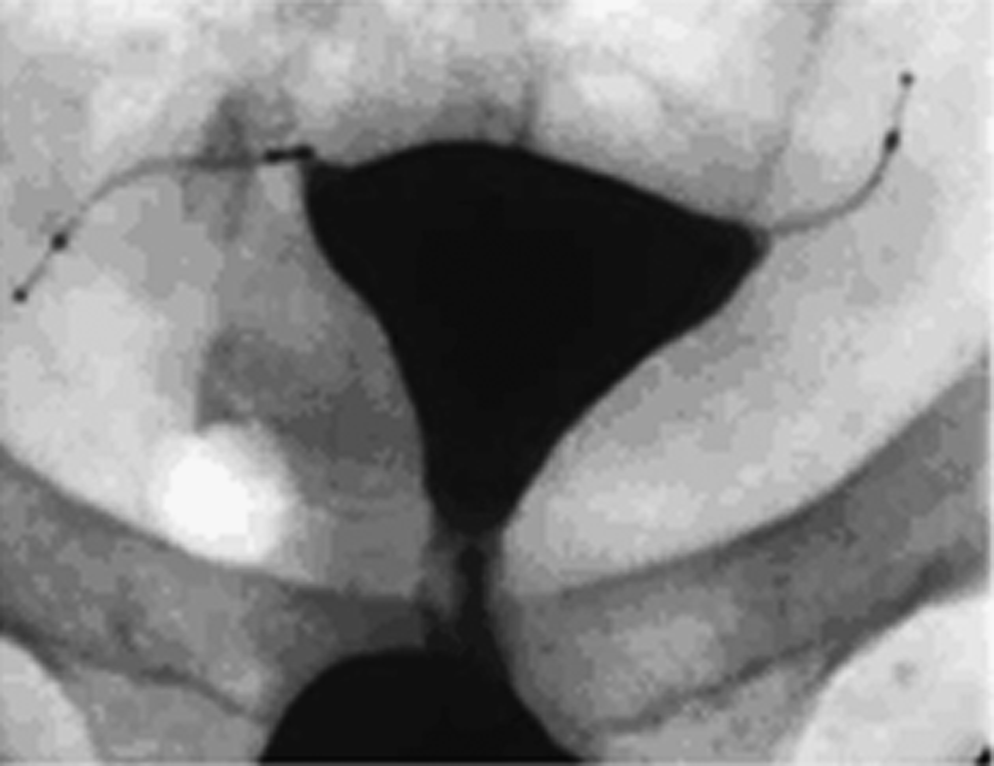
Total uterine fill hysterosalpinography, demonstrating the ideal insert location and cornual region occlusion.
Main outcome evaluated
The main outcome that was examined was the ability of 2-dimensional transvaginal sonography at 10–12 weeks to verify proper Essure device localization/occlusion, compared with standard HSG at 12 weeks postprocedure. Secondary outcomes sought were rate of bilateral placements, HSG follow-up by 12 weeks, and clinical pregnancy rate.
All data were collected and tested via standard statistical software (SPSS, Chicago, IL) for sensitivity, specificity, and positive and negative predictive values.
Results
During the study period, 163 patients met eligibility criteria for participation. See Figure 4 for patient triage and study breakdown. A total of 158 (97%) had successful bilateral placement, with 94% completed upon the first attempt. Upon placement, 150/158 (95%) had 3–8 visible coils trailing into the uterine cavity per the manufacturer's guidelines. Of the remaining 8 patients, 4 patients had two visible coils, 2 had nine coils, and 2 patients had only one visible coil at placement.
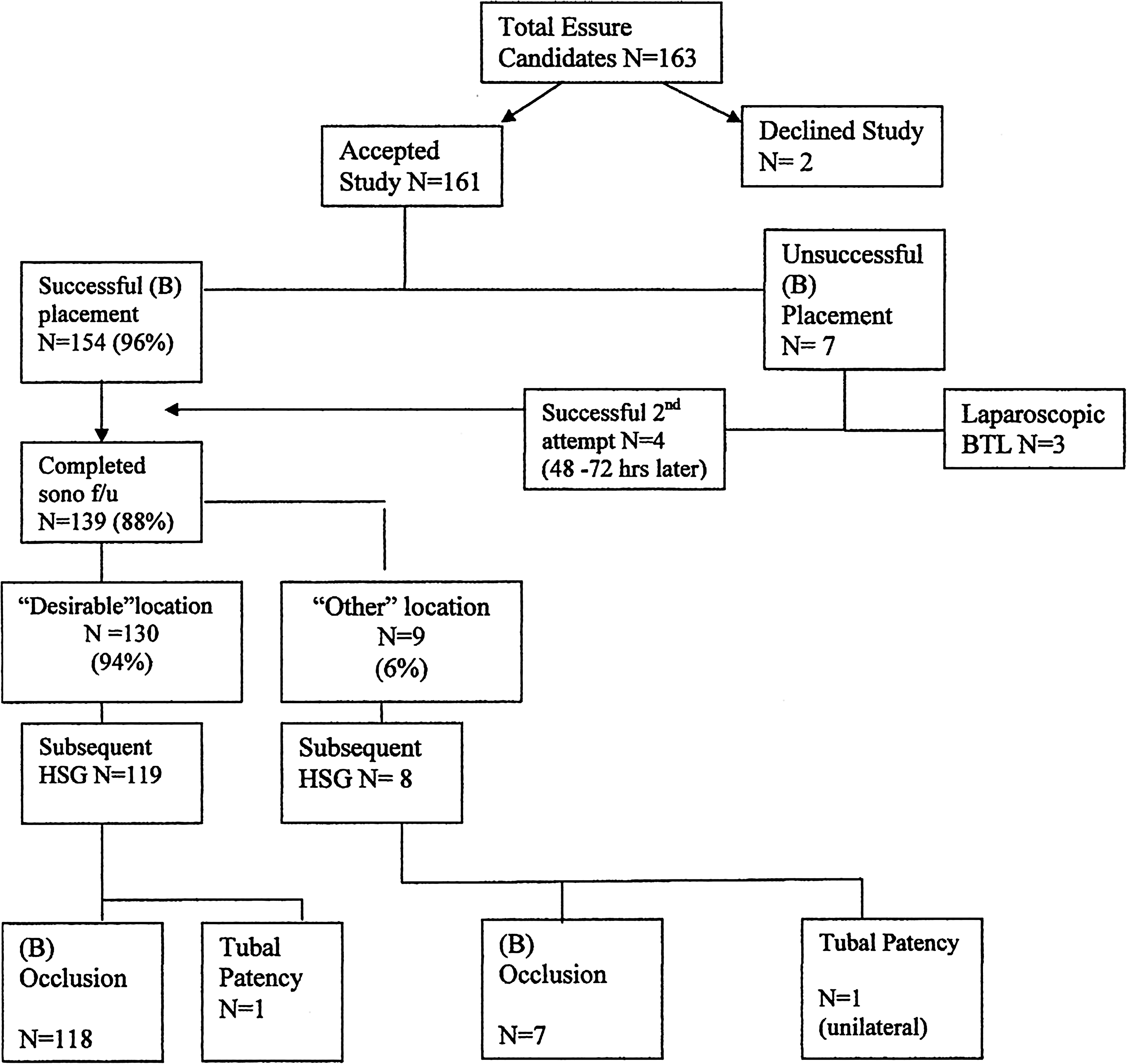
Patient triage and study breakdown. HSG, hysterosalpinograpy; sono, sonogram; f/u, follow-up.
Eighty-eight percent (88%; n = 139) of patients with bilateral placements underwent sonographic study with 94% of this cohort having “desirable” placement per sonographic markers described previously. The remaining 6% (n = 9) with “other” placement all had sonographic visualization of the inserts bilaterally with the proximal tip of the insert at the midlevel myometrial thickness (not abutting the endometrial area but prior to the serosal edge). None of these visualized inserts were found originating beyond the uterine serosal edge.
Of patients who completed the ultrasound evaluation (n = 139), 127 (91%) underwent HSG confirmation, with 98% having successful bilateral occlusion. Only 2% (n = 2) had unilateral occlusion at 12 weeks. Both of these 2 patients were found to have bilateral occlusion at a 6-month HSG confirmation test. See Table 1 for summary. The 12 patients who did not undergo subsequent HSG were lost to follow-up. The overall HSG completion rate in the study cohort was 78% (127/163).
Sensitivity = a/a + c = 94%.
Specificity = d/d + b = 50%.
PPV = a/a + b = 99.2%.
NPP = d/c + d = 12.5%.
HSG, hysterosalpinography; PPV, positive predictive value; NPP, negative predictive value.
No microinsert expulsions or suspected uterine perforations were encountered up to the 3-month follow-up period. As of June 2010, no clinical pregnancies were noted in the 127 members of the evaluable cohort who had undergone both sonographic and radiologic confirmation testing.
The sensitivity of 2-dimensional pelvic ultrasound in predicting tubal occlusion, compared with standard HSG, was 94%, with a positive predictive value of 99%; specificity was 50%, with a negative predictive value of 12.5%.
Discussion
In November 2002, the Essure microinsert (Conceptus, Inc.) became the first hysteroscopically placed permanent female birth control device to be approved by the FDA. As part of the FDA approval of the Essure microinsert, HSG is required for each patient 3 months after microinsert placement. The traditional radiographic HSG is the only imaging method currently approved by the FDA to assess tubal patency in patients with the Essure device, although countries other than the United States have accepted either plain pelvic film or sonogram visualization as a substitute confirmation test. The main advantage of HSG lies in its ability to document microinsert location and tubal occlusion. 6
The current trial sought to evaluate the ability of 2-dimensional pelvic sonography to predict tubal occlusion (by location verification), compared with the gold standard HSG. This article is not the first to describe the use of pelvic sonography for Essure localization as a surrogate for occlusion. In an Australian study, in cases with successful bilateral placements, office ultrasound alone confirmed proper device location at the 3-month visit in 94% of cases. Further imaging was only required in 6% of patients as a result of inability to visualize the inserts appropriately. 7 However, the researchers in that study did not compare their findings against HSG for radiographic demonstration of tubal occlusion. Alternatively, contract infusion sonography (CIS) has been compared with subsequent HSG for tubal assessment. In that pilot study, CIS had comparable accuracy to HSG in the post-Essure setting, although that study was limited by its small sample size (N = 17). 8 Interestingly, tubal occlusion was noted on both CIS and HSG in 82% of patients before 12 weeks.
Other published data has indicated that “the rate of cornual obstruction at 3 months is high enough that plain film radiography can be substituted for HSG to determine if the coils have been retained {in an appropriate position}” 9 Investigators from The Netherlands calculated the sensitivity and specificity of pelvic sonography in predicting tubal occlusion compared with pelvic X-ray; values were 100% and 95%, respectively. This led to the researchers' conclusion that “hysterosalpingography at the 3 month follow up after successful placement of the Essure micro-insert can be replaced by transvaginal ultrasonography.” 10 As reflected in that article, “although X-ray seems to be a sensitive test in detecting the microinserts, limited information is obtained about the soft tissue surrounding it. … Ultrasound has the ability to locate the device and visualize its relationship with the surrounding tissue.” 10 Therein, lies one main advantage of utilizing ultrasound as a confirmation test. In addition, ultrasound has the potential to be performed in the physicians' own office, avoids ionizing radiation, precludes exposure to contrast dye, and, above all, avoids the potential discomfort of HSG. More importantly, variable rates of follow-up for post-Essure HSG have been reported in the literature. In three studies specifically examining rates of adherence with HSG, rates varied from 86.4% to as low as 12.7%.11–14 Compliance in the post-Essure follow-up may be enhanced by offering office-based ultrasound as a more minimally invasive alternative to standard HSG.
The results of the current study demonstrate sonography's sensitivity of 94% with a positive predictive value of 99%. Interestingly, in the “other” placement group of n = 9, 7 of the 8 patients who had follow-up HSG (88%) had documented occlusions. This results in a specificity of 50%, and a negative predictive value of 12% for sonography. All patients in this “other” placement group could otherwise be considered “adequate” placement/location, as the manufacture's confirmation criteria (based on HSG) accepts insert location of 30 mm distal to the uterotubal junction.1,2 In the current trial, patient's whose insertions did not abut the endometrial lining were labeled as having “nonideal” placements in order to investigate that placement as a potential factor leading to patency. This, in fact, was not found, based on follow-up HSG. Again, this is likely the result of the very conservative inclusion of patients under the “other” location in this trial. In this cohort, no patient had sonographic evidence of the insert located any further than mid-myometrial thickness from the endometrial lining (none originated beyond the serosa). The bilateral placement rate (97%) and 2% initial patency paralleled the FDA's trial results for the Essure device (a 96.9% placement rate for ESS 305 and a 3.5% initial tubal patency rate at 3 months). 15
This study has several strengths. First, it provides an adoptable in-office protocol that may serve as a substitute for X-ray confirmation. In addition, the current study builds on—and validates further—other cited literature confirming the ability of ultrasonography to serve as a post-Essure confirmation test. By providing additional literature on this modality, the possibility of a future FDA label change allowing sonography as a confirmation test of choice cannot be underestimated. Currently, this is the case in countries outside the United States in clinical practice. It is a strength of this study that, of the 139 patients who underwent sonographic study, 91% were “matched” to subsequent HSG for validation. Although, overall, 78% of patients treated underwent HSG (a moderate range for post-Essure follow up based on literature), the fact that 22% of the patients did not undergo final radiologic confirmation underscores the need to develop a more patient friendly—and attractive—post-Essure confirmation tool. Office ultrasonography may best serve that purpose. The main limitation is that this study was not designed or powered to evaluate the efficacy of sonography over HSG, although following the cohort for clinical pregnancies—and finding none—contributes to the study's validity. Instead, this study serves to provide a descriptive account of a potential protocol easily adoptable by most gynecologists.
Conclusions
In summary, the rate of cornual obstruction at 3 months is high enough that the protocol described in this article has clinical utility. If microinsert location is found sonographically to be beyond the uterine serosa, one may proceed with HSG confirmation and defer it if location is as described here. In closing, transvaginal ultrasound is an acceptable method of confirming proper location of the Essure sterilization system at 10–12 weeks postinsertion and has reproducible value as a surrogate HSG confirmation test.
Footnotes
Disclosure Statement
Hector O. Chapa, MD, serves as a medical consultant to Conceptus, Inc. and serves on the Conceptus Physician's Advisory Panel. No funding was given for the production or assimilation of this study material. The remaining authors have no competing financial interests.