
Abstract
Abstract
Introduction
Torsion of the fallopian tube is a rare entity, and it usually presents as an acute condition. Fallopian-tube torsion most often occurs along with ovarian-cyst torsion. The etiology of isolated torsion includes hydrosalpinx, after sterilization operation, tumors of the fallopian tube, and hematosalpinx. Torsion is a mechanical event because of extrinsic and intrinsic factors operating together to cause it.2,3
This case is reported here because of the rarity of torsion, and because of the clinical features with which it mimicked bilateral ovarian neoplasm.
Case
A 13-year-old adolescent girl who attained had menarche 6 months previously was referred to the Jawaharlal Institute of Postgraduate Medical Education and Research as a case of ovarian neoplasm. She complained of lower abdominal pain of 1 month's duration and of a dull backache of 7 months' duration. She did not give any history of vomiting or fainting. Her cycles had been bimonthly, with the flow lasting for 3 days. There was no family history of ovarian or gastrointestinal malignancy. She had had a magnetic resonance imagine (MRI) of the spine 5 months earlier (for the complaint of back pain), which had showed posterolateral protrusion of the L4–L5 and L5–S1 intervertebral discs, with narrowing of the bilateral foramen. Both ovaries were reported to be multicystic.
On general examination, the patient weighed 45 kg had no palor or lymphadenopathy. She was anxious, with a pulse rate of 90 beats per minute. Findings from other systemic examinations were normal. Abdominal examination did not reveal any mass or tenderness. Her hymen was intact, and a rectal examination revealed a 5×6–cm cystic mass, which was felt anterior to the rectum, which was tender on palpation.
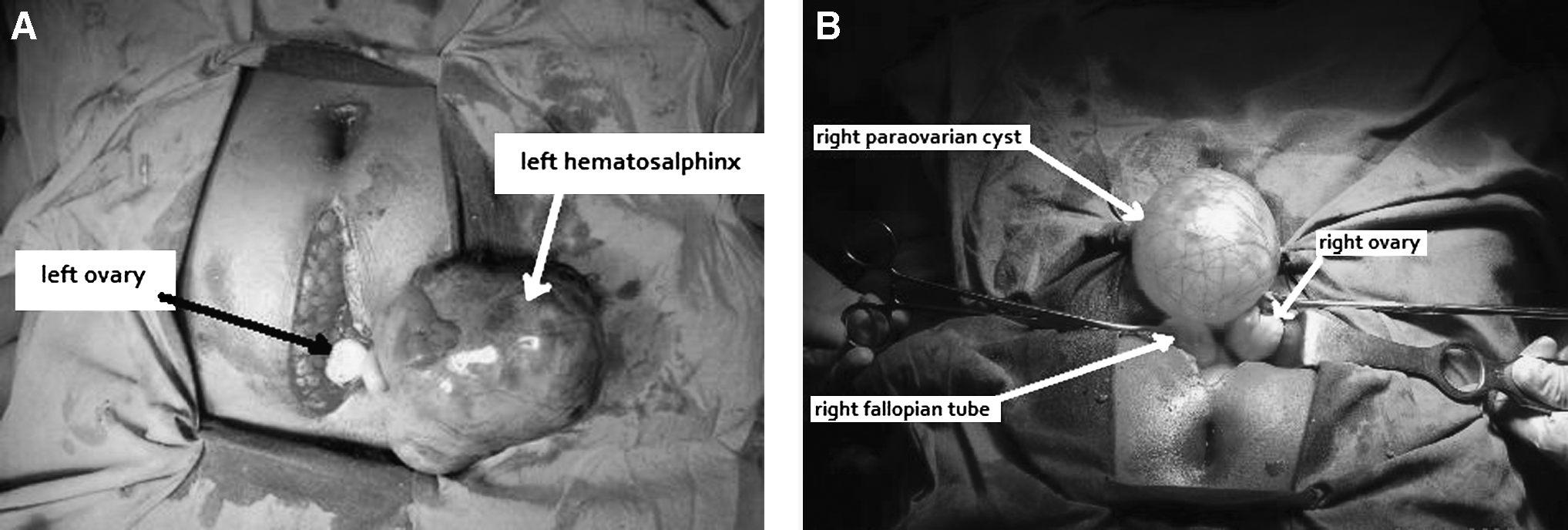
Transabdominal sonography (TAS) showed the uterus to be of normal size, and there were bilateral adnexal masses; the left measured 7.43×5.41 cm with mixed echogenicity, with a cyst wall thickness of 3.2 mm on average. The right adnexal mass was completely anechoeic and measured 7.3×6 cm. There was no free fluid, and her liver and both kidneys were normal. A complete hemogram was normal except for the erythrocyte sedimentation rate (ESR), which was 55 mm. Results of liver function tests, renal function tests, and thyroid function tests were normal. A Mantoux test was negative and a chest radiograph did not reveal any abnormality. Hydatid serology was negative. Tumor markers revealed a CA-125 level of 14.2 U/mL, a lactate dehydrogenase (LDH) level of 152 U/L, and α-fetoprotein level of 0.95 ng/mL. Laparotomy was performed as per the hospital protocol (to avoid laparoscopy because of suspicion of malignancy) after obtaining informed consent from the patient's parents and making arrangements for frozen section. There was no ascites, and, surprisingly, both ovaries were normal. The left tube showed a 10×8 cm mass with variable consistency, which had undergone torsion several times (Fig. 1 A). On the right side, there was a paraovarian cyst of 10×10 cm (Fig. 1B). The twisted tubal mass was excised and sent for frozen section, which did not show any malignancy. Right-sided paraovarian cystectomy was performed. The histopathologic examination results showed a left hematosalpinx and a right-sided paraovarian cyst as a serous cysadenoma.
Results
She came for follow-up after 6 weeks and was happy to confirm the benign nature of the condition as was noted in the histopathologic report.
Discussion
Diagnosis of adnexal mass poses a great problem because a wide variety of conditions affect the adnexa, and the diagnostic dilemma increases when they occur in premenarchal, adolescent, and postmenopausal women, and when these masses are complex or have solid components seen on ultrasound. This was the reason for suspecting malignancy in the above case even though tumor markers were negative. Adnexal torsion usually presents with acute clinical features; a chronic presentation is a rare occurrence, and the symptoms are nonspecific. Isolated torsion of the fallopian tube is seen only in 5% of cases. Mostly, torsion involves the ovary and the fallopian tube, and the preoperative diagnosis is made in 71% of cases by ultrasound. 4 In the present case, neither ovary was visualized distinctly from the masses on ultrasoound; hence, the adnexal masses were presumed to be of ovarian origin. This patient presented with chronic symptoms, and her ovaries were not adherent to her fallopian tubes or the paraovarian mass.
Sonographic features of adnexal torsion usually show a cystic or complex mass with some amount of free fluid in the pelvis, 4 and this finding was absent in the present case. However, the presence of free fluid with a complex or solid mass will point to a greater possibility of malignancy. 5 Hematosalpinx is also associated with pelvic fluid, and the mass is round and usually echogenic; however, it can have a homogenous or heterogenous echotexture. 6 These sonographic findings can be mimicked by other masses, such as a tubo-ovarian abscess, tubal neoplasm, or pedunculated fibroid.
The incidence of paraovarian cysts is ∼10%. These are also rare in the adolescent age group; they present usually in the third and fourth decade of life. Torsion of a paraovarian cyst along with torsion of the fallopian tube in a 15-year-old girl was reported by Dahiya and colleagues in one case and by Szczepanik and Wittich in another case.7,8 A computed tomography scan with a pelvic ultrasound was found to be helpful in the second case to arrive at a preoperative diagnosis of nonovarian origin of the adnexal mass. Paraovarian cysts predominantly arise from tissues of the broad ligament and can be reported in histopathologic assessments as papillary serous cystadenomas as one of their transformations. In the present case, it was reported as a serous cystadenoma. Laparoscopic surgery is considered to be the “gold standard” for patients with adnexal masses, and adnexal-sparing surgery should be practiced whenever possible.9,10 A combined approach (laparoscopy and laparotomy when necessary) is recommended in adolescents with adnexal masses, as most of them are benign. 11 This approach could have been thought of in the present case, as the tumor markers were negative. It was not adopted because bilaterality indicated a greater possibility of ovarian malignancy. A preoperative MRI of the pelvis would have helped to make an accurate preoperative diagnosis.
Conclusions
Diagnostic laparoscopy should always be considered in an adolescent with an adnexal mass, before subjecting her to a laparotomy, even when the mass is bilateral, so as to avoid laparotomy. When the tumor markers are negative and the mass is within the pelvis, this approach will avoid anxiety for the patient, and will provide more satisfaction with, and confidence in, the treating surgeon. Tubal origin of the adnexal mass also should be considered, although it is rare in adolescents.
Footnotes
Disclosure Statement
No competing financial conflicts exist.