
Abstract
Abstract
Introduction
Case
A 27-year-old pregnant woman, at 28 4/7 weeks' gestation, complained of a right thigh skin lesion, 0.8 cm in size, which had been present for a year and a half. The patient had no personal or family history of melanoma. Her primary care physician performed a shave biopsy of the skin lesion, which revealed nodular malignant melanoma with Breslow's thickness of at least 1.83 mm. Histologic examination revealed no ulceration and tumor mitotic rate of 1/mm2. The lesion was classified as Clark's level IV. Additionally, no perineural or venous invasion was observed and the tumor infiltrating lymphocytes were characterized as focal and non-brisk. Lateral and deep margins were involved.
Upon physical examination, a 5-mm eschar on the right thigh was identified, with no satellitosis or in-transit metastases, and no regional lymphadenopathy. Chest radiographs revealed mild cardiomegaly and mild vascular congestion, and LDH levels were normal. Treatment pursuant to the National Comprehensive Cancer Network's (NCCN) guidelines was administered, including sentinel lymph node biopsy (SLNB) and wide local excision (WLE).
Lymphoscintigraphy was performed to locate the sentinel lymph nodes. Technetium-99m (99mTc) filtered sulfur colloid was injected intradermally around the previous biopsy site. Superomedial migration of the radiotracer was visualized by planar imaging. Focal areas of radiotracer uptake in the right groin compatible with inguinal lymph nodes were identified. Because the patient was pregnant, continuous fetal monitoring was performed while she was under general anesthesia. Two identified sentinel lymph nodes in the right groin were excised.
WLE of the lesion was performed with 2-cm margins, using an elliptical incision with a length to width ratio of 3:1. The incision was extended down to the fascia, and skin flaps were created in order to close the wound primarily in a layered fashion. Pathology submitted from the WLE specimen indicated no residual malignant melanoma and sentinel lymph nodes were negative for disease. According to NCCN guidelines, there was no role for adjuvant therapy for stage IB (T1b N0 M0) disease. The patient subsequently delivered a healthy, full-term fetus via cesarean section. Importantly, the placenta was submitted to pathology for examination to eliminate the possibility of metastasis, as melanoma is known to be the most common tumor to metastasize to this site. Gross and microscopic evaluation of the placenta revealed no melanocytotic proliferation. Annual clinical surveillance and follow-up was recommended because of the risk of local recurrence. At time of publication, both patient and child are healthy with no sequela of disease.
Discussion
Several reports have indicated that malignant melanoma during pregnancy may be associated with increased Breslow thickness compared to nonpregnant controls.4,5 This may be explained by the physiologic changes a woman can experience during pregnancy. Women can have a darkening of the skin on the face, abdomen, and other areas of the body during pregnancy, a condition known as “melasma”. In addition to melasma, nevi typically change during pregnancy; chloasma and changing nevi are accepted as physiologic 5 because of changes in hormones. Women are made aware of these hormonal effects, and may be less alarmed by nevi that seem to change in color or size during pregnancy. Therefore, a delay in diagnosis of malignant melanoma in pregnant women may account for increased Breslow thickness observed in this population. 6
Surgical excision is the primary treatment for malignant melanoma; guidelines on excision of malignant melanoma include wide local excision with margins correlating to Breslow thickness. Discussion of sentinel lymph node biopsy should be considered on a individual basis, as per the NCCN National Guidelines, 7 because the most powerful prognostic factor related to recurrence and survival in patients with clinically localized melanoma is the status of the SLNB.3,8
Although controversy still exists, 9 SLNB is currently being used by many surgeons in pregnant women. There is apprehension with pregnant patients when it comes to the safety of treatment with SLNB. Most concerns center on the issue of possible injury to the fetus as a result of using radiotracer, and the associated radiation exposure. A consensus panel from 2005 recommended against SLNB in pregnant patients pending further investigation, whereas recommendations from an international expert panel meeting in 2006 conceded that pregnant patients could be offered SLNB using technetium after careful counseling regarding safety and efficacy. 10
SLNB is commonly performed with two tracer substances, blue dye and radioactive labeled sulfur colloid. 9 Isosulfan blue and methylene blue are both classified as pregnancy class C compounds. Currently, insufficient data exist on the safety of blue dyes for use in pregnancy, and therefore, they should not be used in this patient population. 11 Isosulfan blue carries a rare, but serious risk of anaphylactic reaction, which is further contraindication for its use.9,12,13 In lymphoscintigraphy, the colloidal tracer has >95% retention at the injection site 14 or in the sentinel node(s), which are then resected at the time of surgery. 15 . Gentilini and coworkers showed that 99mTc largely remains trapped in the injection site or within the lymphatic structures and only a small amount of the injected radiation is found circulating in the blood pool and urinary system. 16 All authors concluded that the level of exposure to radioactive material is insignificant for both the patient and the fetus. 14
Radiopharmaceuticals used for lymphatic mapping deliver whole fetal doses <5 mGy, and therefore carry negligible risk and are not contraindicated in pregnant patients.17–19 Potential absorbed radiation doses to the fetus have been calculated using various pharmacokinetic and biodistribution models for both 0.5 and 2.5 mCi of 99mTc doses, finding that maximum calculated doses were roughly 4.3 mGy, which is well below the 50 mGy threshold absorbed dose for adverse effects to the fetus. 20 The administered dose of radiation to the uterus has been demonstrated not to exceed 0.5 mGy and as such, is estimated to be harmless 10 (Fig. 1). Additionally, average measured uterine exposure has been shown to be significantly less than background radiation (∼14% of daily background radiation) 9 (Fig. 2). Research has shown that the risk for the induction of genetic defects as a result of radiation exposure is very low (0.0024%–0.0099% per mGy). 14 Furthermore, a study by Mondi et al demonstrated 9 of 9 pregnant patients who underwent SLNB in their first or second trimesters delivered at term, and there have been no birth defects or discernable malformations in any of the children to date. 10

Radiation delivered to the fetus during diagnostic testing and required absorbed radiation for adverse effects. mGy, milligray (unit of kinetic energy transferred to matter); CXR, chest X-ray; UGI, upper gastrointestinal fluoroscopy; KUB, abdominal X-ray; SLN; sentinel lymph node; BE, barium enema; CT A/P, computed tomography of abdomen and pelvis.
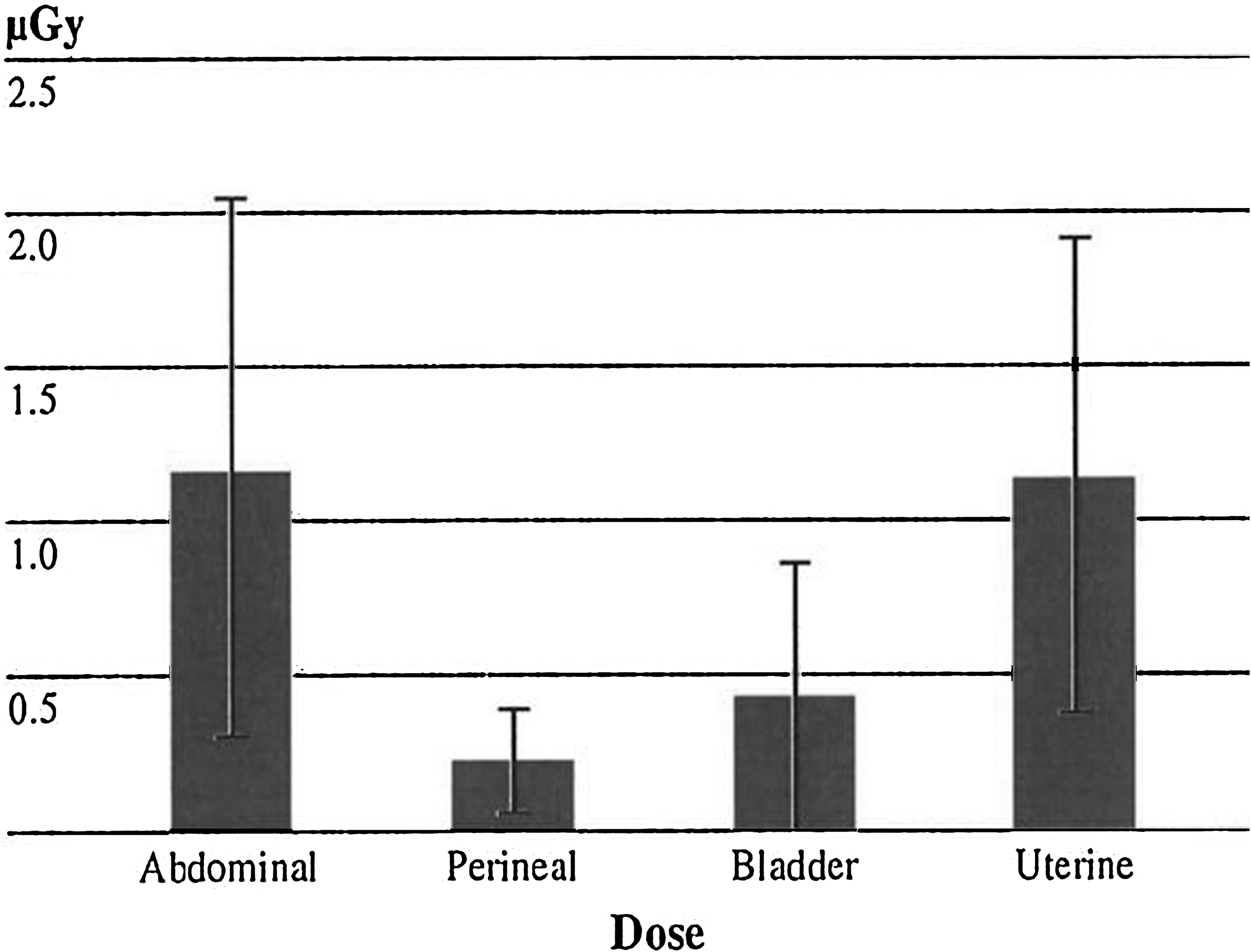
Daily background radiation delivered to female anatomy. Radiation measurements at selected sites: Radiation dose in μGy to abdominal, perineal, bladder, and uterine areas. Top of graph represents daily background radiation (8.2 μGy). Error bars show standard deviation.
The diagnosis and treatment of malignant melanoma in pregnancy does not differ from the diagnosis and treatment of nonpregnant patients. 21 The key to treatment, as always, is prompt biopsy and diagnosis. This will help to decrease the possibility of metastases, especially to the placenta (and possibly the fetus) in pregnant women. Placental involvement does not necessarily mean that the newborn will develop melanoma.8,22 To date, 20 cases of malignant melanoma metastatic to the placenta, based on gross or microscopic examination, have been reported. 5 Most cases of placental metastases from melanoma occurred with maternal metastases to other viscera (stage IV);2,8,23,24 even then metastases to the fetus are rare. 5 The probability of fetal metastases when the mother is diagnosed with malignant melanoma during pregnancy is dependent upon her stage of the disease. 5 Literature reveals that only 22%–25% of infants with placental metastatic melanoma go on to develop the disease. Those statistics aside, maternally derived melanoma metastases in the infant are almost always manifested at the time of delivery and are almost invariably fatal.22,25
Conclusions
The management of malignant melanoma in pregnancy requires a strong multidisciplinary approach. Wide local excision of the malignant lesion and SLNB using 99mTc without blue dyes, in the setting of safe anesthesia practices in pregnancy,26–28 can safely be used in the diagnosis and treatment of pregnant women with malignant melanoma. Many well-controlled studies have provided strong evidence that the clinical course, prognosis, and overall survival of pregnant women with localized malignant melanoma (American Joint Committee on Cancer stage I or II) are similar to those in nonpregnant women.3,5 If left untreated, malignant melanoma in pregnancy can result in metastatic disease to the placenta and fetus. This is a rare, yet very serious manifestation. However, a gross and microscopic examination of the placenta from malignant melanoma should be performed, with the pathologist alerted to maternal history, as this is not standard in the course of placental histopathology. Finally, because the overwhelming majority (>75%) of melanoma recurrences occur within 2 to 3 years after treatment of the primary lesion, many women are encouraged to avoid becoming pregnant for that period of time postoperatively, 29 although many recent reports have indicated that this may not be necessary.
Footnotes
Acknowledgments
The authors thank Roberta E. Redfern, PhD, for editorial assistance in the preparation of this article.
Disclosure Statement
No competing financial conflicts exist.