
Abstract
Abstract
Introduction
Case Report
A 42-year-old woman presented in the emergency department with sudden pain in her abdomen and vomiting. Ultrasonographic examination showed large, predominantly cystic, bilateral adnexal masses, measuring 7.1×6.1 cm and 6.4×5.8 cm, with a highly echogenic component. Both ovaries were not separately defined. The possibility of a bilateral dermoid cyst was suggested by the radiologist.
The patient underwent exploratory laparotomy with a hysterectomy and bilateral salpingo-oophorectomy. The patient's postoperative course was uneventful, and she was discharged from the hospital on day 5 after surgery. The left ovarian mass measured 8×6×3.5 cm and the left ovarian mass measured 7.2×6.5×5.0 cm. The outer surface was tan and smooth. Cut sections of both ovaries were partly solid and partly cystic. Multiloculated cysts filled with cheeselike material and hairs were seen. Slides were prepared, stained with hematoxylin-eosin, and seen under the light microscope.
Sections from the cystic areas showed a lining of keratinizing stratified squamous epithelium, including sebaceous glands, sweat glands, and hair. Neural tissue, respiratory and gastric epithelium, fat, bone, and thyroid follicles were also identified.
One of the sections taken from the solid area in the left-sided dermoid showed glands arranged in lobular architecture (Figs. 1 and 2). They were lined by dual cell lining, showing well-differentiated central, larger, mature cells with vacuolated cytoplasm, and peripheral, smaller, less-differentiated, basaloid or germinative cells. A diagnosis of sebaceous adenoma arising in mature cystic teratoma was made.

Section shows pseudostratified respiratory epithelium, adipose tissue, and lobules of sebaceous glands (hematoxylin and eosin, original magnification ×100).
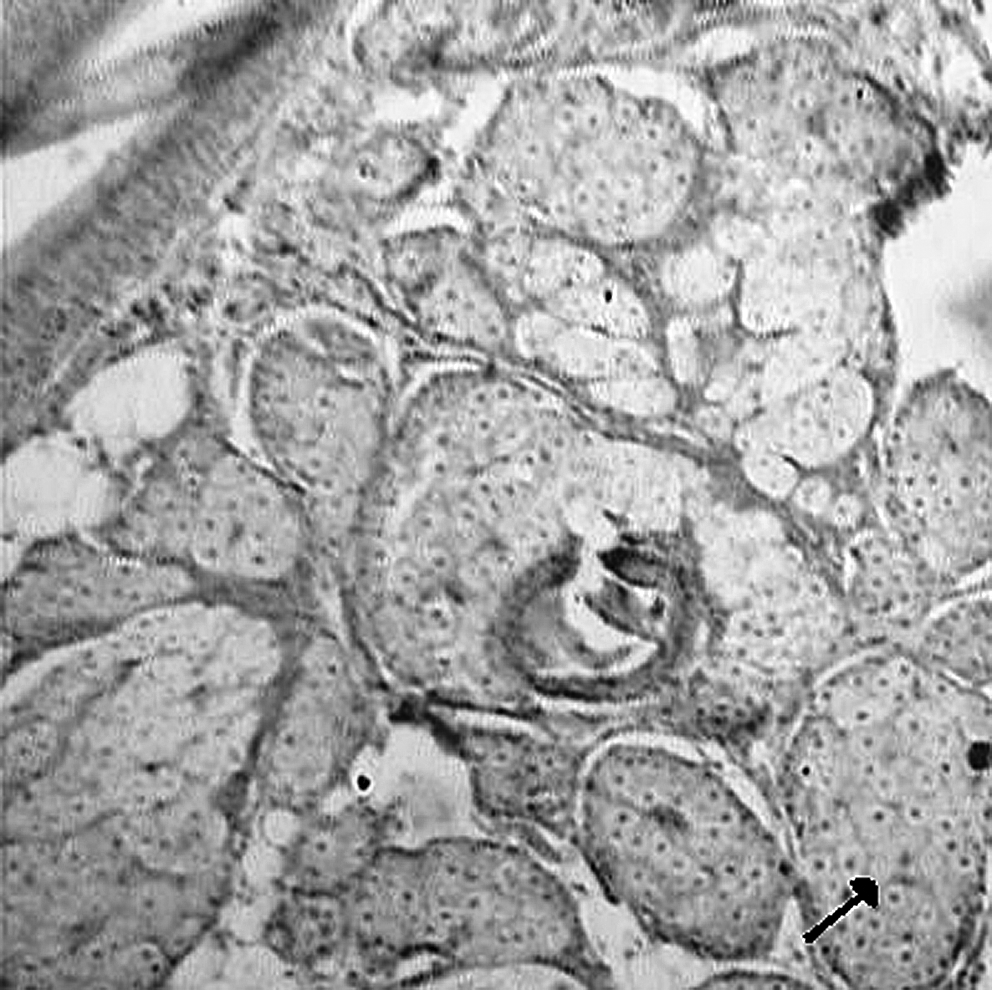
The glands contain large vacuolated cells in the center and basaloid type cells at the periphery (hematoxylin and eosin, original magnification ×100).
Discussion
Monodermal neoplasias are uncommon in mature cystic teratomas, probably occurring in ∼2% of all cases. The most common malignant change in cystic teratoma is squamous-cell carcinoma, followed by carcinoid tumor and adenocarcinoma.
1
Benign tumors have also been described, and sebaceous adenoma is one of them. It is a very rare entity. Its morphologic appearance and clinical behavior is similar to the homonymous somatic tumor
To date, only 4 cases of sebaceous adenoma in dermoid cysts have been reported. Unlike the patient in this current report, each of the other patients had a unilateral dermoid cyst, which is, in fact, a common occurrence; the incidence of bilateral dermoid cysts is 10%–15%.3,4 All of the cysts were indolent. None of them recurred or metastasized.
Dermoid cysts with epithelial neoplasms are rarely found in young women. Over three quarters of the patients are >40 years of age, with the average age being 50, as also was seen in the patient described here. 5
Because of rarity of this lesion, it may be missed by a pathologist. It is also important to distinguish it from sebaceous carcinoma, as the two entities have different clinical characteristics and development. The distinguishing features are absence of cytological atypia, capsular and vascular invasion, necrosis, and hemorrhage. 5 The presence of a sebaceous carcinoma usually indicates a poor prognosis for a patient. To avoid missing the diagnosis, any thick area in the wall of a dermoid cyst must be selected and sectioned for histologic analysis. 5
Conclusions
In conclusion, sebaceous adenoma is an extremely rare occurrence in benign cystic teratoma. Its development and clinical outcome is that of a benign tumor. Surgery is curative, and further treatment is not required.
Footnotes
Disclosure Statement
No competing financial conflicts exist.