
Abstract
Abstract
Introduction
LOD can produce high ovulation (>80%) and pregnancy (up to 60%) rates, 4 and it also corrects the underlying endocrine abnormalities associated with the disease, such as raised serum concentrations of luteinizing hormone (LH) and androgens.2,5–7 In addition, ovarian drilling may render the ovaries more sensitive to clomiphene citrate. 7
Although LOD is widely practiced by many gynecologists, there is a lack of consensus on how much energy should be used. It depends upon the number of punctures made, and the power setting and duration of each puncture. Currently, the choice of the number of punctures to be applied at LOD is empiric. Historically, the amount of ovarian tissue removed during bilateral ovarian wedge resection varied between one third and three quarters depending upon the size of the ovary.8–11 Some gynecologists apply the same principle to LOD by empirically making different numbers of punctures in each ovary depending upon its size; between 3 and 25 punctures have been reported with power settings between 30 and 400 W.1,5,6,12–16 As a general principle, increasing the amount of thermal energy delivered to the ovarian stroma may increase the efficacy of the procedure, but at the expense of increasing the risk of ovarian atrophy. 16
This study was designed to investigate the influence of the amount of thermal energy delivered to ovarian tissue on clinical outcome after laparoscopic ovarian drilling in women with PCOS, to achieve satisfactory results for the surgery with the least ovarian destruction.
Materials and Methods
Subjects
From January 2004 through September 2007 (∼4 years' duration), this randomized trial took place in the infertility unit of Al-Hammadi Specialized Hospital, Riyadh, Saudi Arabia. A total of 82 women with anovulatory infertility associated with PCOS, who had been clomiphene citrate resistant, underwent LOD to assess the optimal number of punctures to be applied to ovarian tissue. All subjects provided written informed consent. Subjects who fulfilled both inclusion and exclusion criteria were randomly assigned to one of the five treatment groups (1:1:1:1:1 ratio). Each randomization number corresponded with one of the five possible interventions, and labeling was done by personnel not involved in the trial. There were 17 cases in groups 3 and 4, and 16 cases in groups 1, 2, and 5.The data used in this study were collected from 76 subjects after exclusion of 6 subjects who missed follow-up (3 cases in group 1, 1 case in group 2, and 2 cases in group 5, Fig. 1).
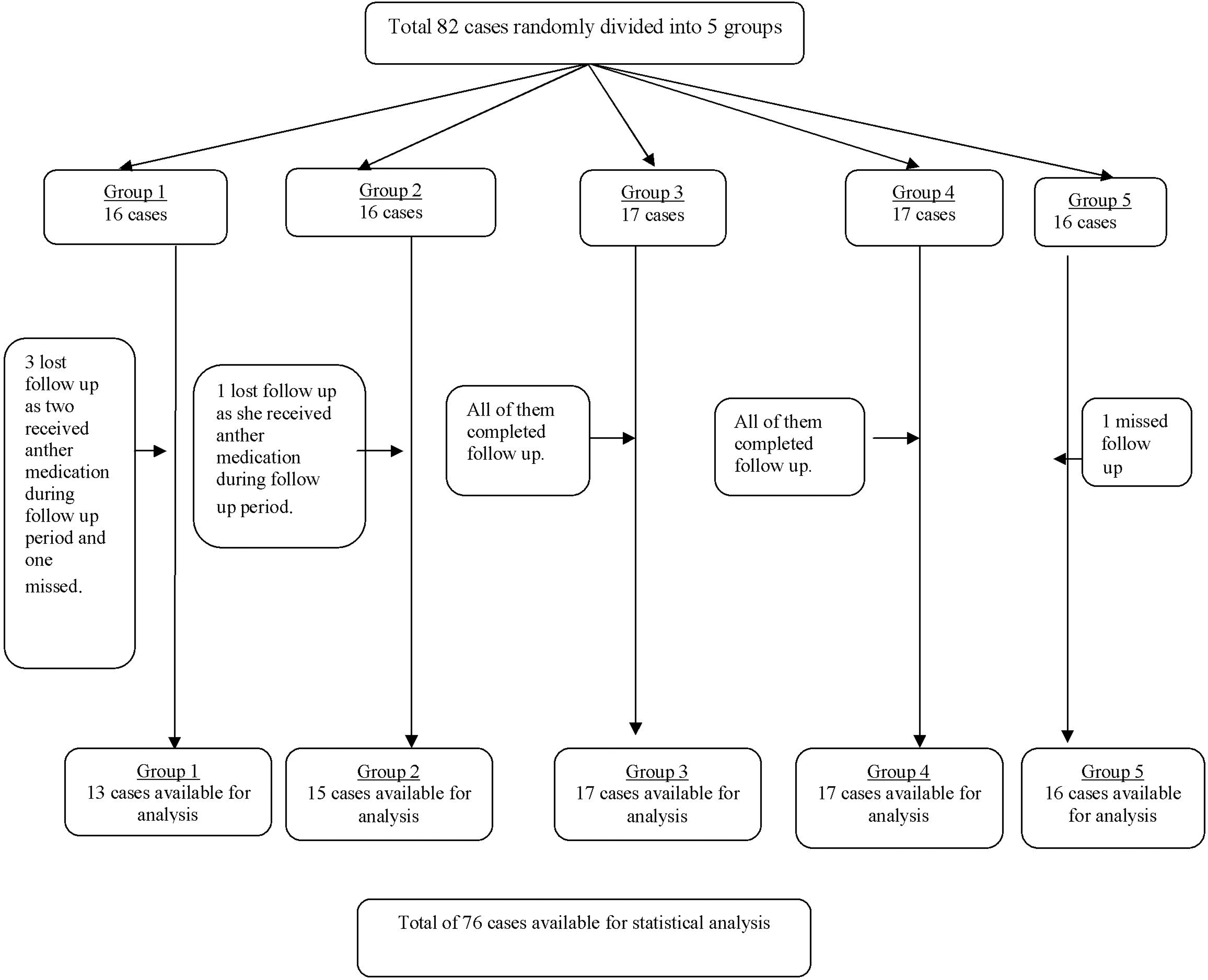
Flow of participants through the trial.
Clomiphene citrate resistance was defined as the absence of developing follicles after ovarian stimulation with 150 mg clomiphene citrate/day given for 5 days beginning with the 2nd day of the menstrual cycle, or failure of conception after responding to induction. Patients were stimulated with clomiphene for a minimum of three and a maximum of six cycles. In the current study, clomiphene citrate failed to induce ovulation in 67 women; the remaining 9 patients ovulated but failed to conceive after clomiphene citrate treatment for 6 months.
PCOS was diagnosed according to the revised European Society of Human Reproduction and Embryology (ESHRE) and American Society for Reproductive Medicine (ASRM) criteria of 2004, which were based on the Rotterdam criteria: the presence of two out of three diagnostic criteria of the Rotterdam consensus being present for each patient, namely, 1) oligomenorrhea or amenorrhea; 2) hyperandrogenism (clinical and/or biochemical); or 3) polycystic ovaries on ultrasound, with the exclusion of other etiologies.17–19
Ovulatory dysfunction was defined as:17,18 oligomenorrhea (menstrual bleeding that occurs at intervals of >35 days to 6 months, with <9 menstrual periods per year) or secondary amenorrhea (an absence of menstrual periods for 6 months).
Polycystic ovarian morphology by ultrasound was defined as:19,20≥12 follicles in at least one ovary measuring 2–9 mm in diameter, or a total ovarian volume of >10 cm. 3 The ovarian volume was calculated using the formula for a prolate ellipsoid: 0.523×length×width×thickness, according to the method of Sample et al. 21 Ultrasound volume is presented as the mean volume of both ovaries.
Androgen excess or hyperandrogenism: this clinically manifests as excess terminal body hair in a male distribution pattern (hirsutism). Some patients have acne and/or male-pattern hair loss (androgenic alopecia). Hirsutism was evaluated using the modified Ferriman–Gallway; mFG 22 score; if the mFG score was ≥8. Androgen excess can be tested by checking for testosterone and androstenedione levels on the early follicular phase (defined as days 2–5 of the menstrual cycle). In women with severe oligomenorrhea or amenorrhea, a random blood sample was accepted. For the purpose of this study, subjects were deemed hyperandrogenaemic if the level of total testosterone was ≥2–5 nmol/L, free androgen index (FAI) was >4, or androstenedione was ≥10 nmol/L.22–25 FAI is calculated using the formula testosterone × 100/sex hormone-binding globulin (SHBG).18,22,25
Conditions that should be ruled out include: 21-hydroxylase-deficient nonclassic adrenal hyperplasia (NCAH), Cushing's syndrome, and androgen-secreting neoplasms by appropriate testing, if suspected clinically.19,25,26 There are also a number of other disorders that may result in ovulatory dysfunction, including hyperprolactinemia and thyroid abnormalities. 26
An LH:follicle stimulating hormone (LH:FSH) ratio>2 may be helpful, but has limited sensitivity and is no longer a necessary part of the diagnosis of PCOS. 27 Hyperinsulinemia is common; however, it is not essential for a diagnosis of PCOS. 28 Hyperinsulinemia has not formed part of any of the recognized definitions to date, and the task force found no evidence to suggest that it should be otherwise; 18 therefore, a test for this was not performed in the current study.
The other exclusion criteria included:
• Other known causes of infertility including male factor infertility or known tubal disease • The presence of a persistent ovarian cyst ≥12 mm as documented by ultrasound because of the bias in ovarian assessment.
Laparoscopic ovarian diathermy
The techniques of LOD used were those that have been previously published by Li et al., 4 and Amer et al. 6 The same operator performed all laparoscopic procedures. Three-puncture laparoscopy was performed with the patient under general anesthesia. After executing a pneumoperitoneum using a Verres needle, a 10-mm videolaparoscope was inserted umbilically, followed by the lateral insertion of two 5-mm ancillary trocars in the left and right iliac fossa. A careful inspection of the pelvic cavity was performed in each patient. Through one of the two lower abdominal 5-mm punctures, a non-toothed grasping forceps was then used to grasp the utero-ovarian ligament and to lift the ovary away from the bowel. The third entry was used to introduce the diathermy needle. A specially designed monopolar electrocautery probe (Karl Storz GmbH and Co. KG, Tuttlingen, Germany) was used to penetrate the ovarian capsule at a number of points with the aid of a short burst of monopolar diathermy. The probe has a distal stainless steel needle measuring 8 mm in length and 2 mm in diameter projecting from an insulated solid cone. The probe was applied to the surface of the ovary at a right angle to avoid slippage and to minimize surface damage after setting the electrosurgical device (ErbotomACC450, Erbe GmbH, Tubingen, Germany). A monopolar coagulating current at a 30 W power setting was used to make a puncture in the ovarian tissue. As the needle was pushed into the ovarian capsule, electricity was activated for 5 seconds. A total of two to eight punctures were made in each ovary depending upon its study group. The ovary was then cooled down by irrigation using Ringer's solution before releasing the ligament. At the end of the procedure, ∼200 mL of Ringer's solution was left in the pelvis.
Amount of thermal energy: a standardized monopolar coagulation current set at 30 W was applied for duration of 5 seconds per puncture, giving a total thermal energy of 150 J (30×5) per puncture.
Postoperative monitoring
Following ovarian diathermy, women were asked to keep a record of their menstrual cycle for 6 months. If the patient started a menstrual period within 6 weeks of the surgery, a blood sample was taken on day 2 of that cycle for measurement of serum concentrations of LH, FSH, testosterone, androstenedione and SHBG. If spontaneous menstruation did not occur during the 6 weeks following surgery, a random blood sample was taken to measure all the abovementioned hormones.
Reproductive outcomes
The rates of conversion of oligo/amenorrhoea to regular cycles, spontaneous ovulation, and conception after LOD using different doses of thermal energy (numbers of punctures) were detected. Ovulation rate was calculated as the percentage of ovulatory cycles relative to total cycles. Pregnancy rate was defined as the percentage of pregnancies relative to total cycles.
The ovulatory cycles were evaluated using transvaginal ultrasound (TV-USG). The scans were performed every 3 days, starting on day 7 after intervention (during the first month from surgery), and subsequently on day 2 after the onset of menses. When the follicular dimensions achieved at least 16 mm, the TV-USG was performed daily. The day of ovulation was retrospectively defined with the observation of decreased follicular dimensions and of liquid in the cul-de-sac, and confirmed by a plasma progesterone level ≥30 nmol/L on day 21 of the cycle. A rising β-human chorionic gonadotropin level and the sonographic evidence of intrauterine gestational sac were considered criteria to define a pregnancy.
Analysis of the data
Patients (76 cases) available for statistical analysis were divided into five groups according to the number of punctures made in their ovaries during LOD as follows: group 1 (n=13) treated with two punctures per ovary=300 J; group 2 (n=15) three punctures=450 J; group 3 (n=17) four punctures=600 J; group 4 (n=17) five punctures=750 J; and group 5 (n=16) six to eight punctures ≥900 J. The clinical and biochemical data before and after LOD were documented. The age of the patients and other demographic details including body mass index (BMI), primary or secondary infertility, and the duration of infertility were also documented. The data were entered into the Statistical Package for Social Science (SPSS) for Windows, version 11 (SPSS Inc., Chicago, IL). Appropriate statistical tests including multiple comparison using ANOVA and z-test were performed, wherever appropriate, among the five groups. Data are expressed as mean ± SD. Significance of the test was performed at the 5% level (p<0.05).
Results
The demographic, clinical and endocrinologic characteristics of the 76 women who underwent LOD are shown in Tables 1 and 2. The characteristics of each group are shown separately. ANOVA showed no significant difference among the five groups pre-LOD.
Shows characteristics of women with polycystic ovarian syndrome who underwent laparoscopic ovarian diathermy: comparison between women treated with different doses of thermal energy (numbers of punctures). Values are given as mean (standard deviation) and number of observations as n (%). The results shown are those obtained before the operation.
Shows characteristics of women with polycystic ovarian syndrome who underwent laparoscopic ovarian diathermy: comparison between women treated with different doses of thermal energy (numbers of punctures). Values are given as mean (standard deviation) and number of observations as n (%). The results shown are those obtained before the operation.
LH, leutinizing hormone; IU, international units; FSH; follicle stimulating hormone; SHBG, sex hormone binding globulin; FAI, free androgen index.
Reproductive performance
Table 3 shows the proportion of women with regular menstrual cycles, the rate of spontaneous ovulation, and the conception rates during the 6 months after surgery, achieved using different doses of thermal energy. The proportion of women with regular menstrual cycles after LOD in group 1 (30%) was significantly lower (p<0.05) than in the other groups (50%–82%), and the incidence of ovulation in group 1 (23%) was significantly lower (p<0.05) than in the other groups (42%–64%). Table 3 also shows that the pregnancy rate in group 1 (15%) was significantly lower (p<0.05) than in the other groups (28%–53%).
>*p<0.5=significant.
Comparison between percentile changes of groups performed through z-test.
LOD, laparoscopic ovarian diathermy; CI, confidence interval.
Endocrine changes
The endocrine changes after ovarian diathermy, using different amounts of thermal energy, are shown in Tables 4 and 5.
Values expressed in mean±SD. z-test was used to compare mean values. Comparison between the groups performed through analysis of variance.
p=significant.
LOD, laparoscopic ovarian diathermy; LH, leutinizing hormone; IU, international units; FSH, follicle-stimulating hormone.
Values expressed in mean±SD. Comparison of means by paired Student's t-test.
p<0.05=significant.
LOD, laparoscopic ovarian diathermy; SHBG, sex-hormone binding globulin; FAI, free androgen index.
Table 4 shows a statistically significant (p<0.05) reduction of serum concentration of LH and the LH:FSH ratio in all groups after LOD compared with preoperative concentrations. The serum levels of FSH after LOD showed insignificant changes in groups 1–4, but a statistical significance increase (p<0.05) in women treated with the highest dose (group 5). ANOVA of all studied groups after LOD showed that the reduction in LH levels and the LH:FSH ratio was highest in group 5, who received six punctures per ovary or more (p<0.05). There were no significant changes in the serum FSH levels after ovarian diathermy except in the women in group 5 (p<0.05).
The results in Table 5 show a statistically significant (p<0.05) reduction in FAI and the serum concentrations of testosterone and androstenedione after LOD in groups 2–5. However, these reductions did not reach statistical significance in group 1.The changes in the serum concentrations of SHBG were variable and statistically insignificant. On the other hand, the reductions of FAI and the serum concentrations of testosterone and androstenedione after LOD were increasingly in women receiving higher doses of thermal energy (from 300 J to ≥900 J). It may, therefore, be concluded that the effect of LOD on androgen levels is influenced by the amount of energy delivered to the ovary, and a small amount may not significantly reduce these levels. This may support the hypothesis that LOD works by the destruction of androgen-producing tissue in the ovary.6,16
Discussion
In this study, the influence of the amount of thermal energy applied at LOD on the clinical and biochemical outcome in 76 women with PCOS divided into 5 groups, has been investigated. The amounts of thermal energy per ovary used in each group were as follows: group 1=300 J; group 2=450 J; group 3=600 J; group 4=750 J; group 5=900–1200 J, using a needle measuring 8 mm in length and 2 mm in diameter at a 30 W power for 5 seconds. A total of two to eight punctures were made in each ovary depending upon its study group.
There are a number of difficulties in comparing the experience of various authors, because of variation in the techniques used in LOD, including: 1) using different instruments (needles, scissors, biopsy forceps, etc.) to deliver the energy to the ovary; 2) applying different amounts of energy to the ovary (measured in joules, equivalent to power in watts multiplied by the duration of electricity applied in second per puncture); and 3) distribution of the thermal energy, either localized to a few holes or more widely spread over many holes with varying depths of penetration. It is important that the comparison between different studies should take into consideration the total amount of thermal energy delivered to each ovary, not just the number of holes made in the ovary and the depth of penetration of energy.
Gjonnaess 1 correlated the ovulation rates after LOD to different numbers of cauterized points. He used a significantly greater amount of thermal energy; five or more punctures were made in each ovary at 200–300 W for 2–4 seconds each puncture (energy on average=250 W×3 sec×≥5=≥ 3750 J per ovary), using a pair of biopsy or sterilization forceps, applied the thermal energy to the ovarian surface, and the depth of penetration was between 2 and 4 mm, that is, superficial. Using the same technique as Gjonnaess, 1 Dabirashrafi and colleagues 29 reported mild-to-moderate adhesion formation in 20% of cases. Naether and colleagues 11 did 5–20 points per ovary, with 400 W for ∼1 second, and they found that the rate of adhesion was 19.3%, and that this was reduced to 16.6% by peritoneal lavage with saline. 11 Naether and coworkers30,31 reported that the greater the amount of damage to the surface of the ovary, the greater the risk of periovarian adhesion formation; this led Armar to develop a strategy of minimizing the number of diathermy points. 32 Armar et al. 2 found that four diathermy punctures (8 mm deep) per ovary at 40 W for 4 seconds per puncture were sufficient to achieve good results, and that no improvement was achieved when applying more holes. The amount of thermal energy delivered to each ovary was 40 W×4 sec×4=640 J, which is significantly lower than that used by Gjonnaess. 1 Armar and Lachelin 32 reported that the smaller the number of diathermy points used, the lower the rate of significant adhesion formation was.
The depth of penetration in this study was up to 8 mm using a specially designed ovarian diathermy needle; the same was done by Armar et al., 2 Felemban et al., 5 and Amer et al.6,16 The amount of thermal energy used to produce a good result ranged from nearly 450 up to 1200 J per ovary, which was significantly lower and deeper than that applied by Gjonnaess. 1 It is therefore possible to conclude that with deeper penetration during LOD, the amount of thermal energy can be reduced without compromising the outcome. Furthermore, achieving good results with deep penetration using low energy supports the hypothesis that LOD works by destroying androgen-producing ovarian stroma.
This study showed that the response to LOD is governed by a dose–response relationship; restoration of menstrual regularity, ovulation rate, and conception rate. Results indicate that 300 J/ovary could be the threshold dose, that is, the lowest dose at which a response could be seen, and 450 J/ovary may be the plateau dose, that is, the lowest dose at which all subjects will respond as nearly the same rates occurred with doses between 400 J and 750 J, but higher doses (≥900 J) showed a lower success rate.
Amer et al. 6 concluded that three punctures (450 J) per ovary seemed to be the plateau dose for LOD. Making seven or more punctures (≥1050 J) per ovary appears to deliver an excessive amount of thermal energy to the ovary; this offers no advantage over the lower doses of energy in terms of success rates, and may potentially cause excessive ovarian damage. Again, Amer et al. 16 reported that the response to LOD is governed by a dose–response relationship. They concluded that four punctures per ovary using a power setting of 30 W for a duration of 5 seconds per puncture (i.e., 600 J per ovary) appear to be sufficient to produce an optimal response (67% spontaneous ovulation rate and 67% conception rate). Reducing the thermal energy below that level reduces the chances of spontaneous ovulation and conception. Malkaw and Qublan 33 studied two groups of patients with clomiphene-citrate-resistant PCOS who had laparoscopic ovarian drilling: group 1 had 5 punctures per ovary, and group 2 had 10 punctures per ovary. The authors concluded that 5, instead of 10, punctures per ovary are sufficient to improve the clinical and reproductive outcome.
Dabirashrafi reported a case of severe ovarian atrophy following LOD in which eight punctures were created at 400 W for 5 seconds per each puncture, equivalent to 16000 J. 15 It is therefore possible that application of excessive amounts of thermal energy to the ovary during LOD will produce irreversible damage to the ovary, leading to ovarian failure. FSH is considered to be a reasonable marker of ovarian reserve and function. 16 In the current study, it is of interest that the application of six or more punctures (≥900 J) per ovary resulted in a 40% increase in the FSH levels after LOD, compared with a nonsignificant variable change in the other groups with less thermal doses. It seems possible that the application of six or more punctures per ovary represents an excessive amount of thermal energy and should therefore be discouraged. This concept is in accordance with the recommendation of older studies.5,6,15,16,29,30
The results of current study showed a statistically significant reduction of the serum concentration of LH, LH:FSH ratio, and androgens in all groups. There were no significant changes in the serum FSH levels after ovarian diathermy except in women treated with ≥900 J/ovary. The magnitude of reduction of LH and androgens show that dose dependency increased with increased thermal energy, with the highest reduction being achieved with more than six punctures per ovary (≥900 J/ovary). The reduction of androgens and LH observed after LOD in this study, which is consistent with several other previous studies,1,2,5,6,16,33–36 supports the hypothesis that LOD exerts its effects through the destruction of androgen-producing tissue in the ovaries. The decreased androgen concentrations may result in a fall in estrone (E1) that may result in decreased positive feedback on LH and decreased negative feedback on FSH at the level of the pituitary. This effect, coupled with a decrease in local androgen concentrations, would convert the intrafollicular environment from being androgen dominant to one that is estrogenic. This may remove an intraovarian block to follicular growth, allowing follicular recruitment and development to proceed to subsequent ovulation.6,16,36 It has also been hypothesized that the response of the ovary to injury during LOD leads to a local cascade of growth factors (such as insulin-like growth factor 1 [IGF-1]), which sensitize the ovary to circulating FSH resulting in the stimulation of follicular growth. 36 The concentrations of anti-Müllerian hormone (AMH) in PCOS patients are significantly higher than in subjects with regular ovulatory cycles. This indicates that there is an intrinsic abnormality in the ovarian follicles themselves in PCOS. 37 AMH is unlikely to be the sole cause of anovulation. 38 Amer et al. 39 reported that, following LOD, the serum AMH concentration significantly decreased and remained low at 3- and 6-month follow-up.
However, caution should be exercised in the interpretation of these results, as the number of punctures applied to ovaries was determined by chance and was independent of ovarian size or endocrine milieu; because of the lower LH levels, hyperandrogenism and smaller ovarian volumes may indicate a milder form of the syndrome and this might have an impact on increasing the amount of thermal ovarian destruction. There is a need in the near future for a prospective study to estimate the optimal amount of thermal energy required for LOD, and to correlate the clinical outcome with ovarian volume and serum concentration of gonadotrophins, androgen, and AMH.
Conclusions
This study analyzed the influence of the amount of thermal energy, through number of punctures made at LOD, on the clinical outcome in terms of restoration of menstrual regularity, ovulation rate, and conception rate. Energy was delivered to the ovary as deep penetration with the specially designed diathermy needle using a power setting of 30 W for duration of 5 seconds per puncture. The application of two holes per ovary (300 J) was found to produce significantly poorer results than those in the other groups who received up to 750 J. Three punctures (450 J) per ovary seemed to be the plateau dose for LOD. Four or five punctures (600 or 750 J) per ovary appear to be sufficient to produce an optimal response. Making six or more punctures (≥900 J) per ovary appears to deliver an excessive amount of thermal energy to the ovary without advantage over the lower doses in terms of success rates, and may potentially cause excessive ovarian damage.
Footnotes
Disclosure Statement
No competing financial conflicts exist.