
Abstract
Abstract
Introduction
Huge uterine fibroids are frequently multiple, usually between 5 and 30 in an individual, but there could be as many as 200 loci within the uterus. However, huge uterine fibroids are common in gynecologic practice in Sub-Saharan Africa, including Nigeria. This is because of the low level of education, poor availability of modern medical facilities for early diagnosis, superstitious cultural beliefs about the possible causes of such an abdominal swelling, and fear of and aversion to surgery even when the fibroids are detected early. The implication of all these facts is that women with uterine fibroids in this environment are more likely to present late with huge masses, severe pain caused by degenerative changes, and respiratory distress caused by impaired movement of the diaphragm, particularly if the fibroid co-exists with pregnancy. Younger women with smaller fibroids are likely to report earlier when their social health is threatened by infertility.
Leiomyoma is a relatively avascular tumor, the blood usually coming from the pseudocapsules (of myometrial tissue) and abnormal venous plexus surrounding them. The rare exceptions are telangiectatic or lymphangiectatic leiomyoma, where numerous blood and lymphatic vessels, respectively, supply the tumors.
The case reported here highlights one of the unusual presentations of leiomyoma in gynecologic practice in this environment. Emergency interventions are more likely to be encountered here because of late presentations; with a background of ignorance, low education, aversion for surgery, and patients' possible fear of losing their uteri to surgery.
Emergency interventions for uterine fibroid are more likely to be required in this environment because of late presentations: these involve blood transfusions to correct severe anemic symptoms, infected fibroid, and acute torsion, intestinal obstructions caused by a pedunculated or parasitic fibroid. 5
Case
A 41-year-old married nulliparous woman with a previous miscarriage presented in the Accident and Emergency Unit of at Obafemi Awolowo University Teaching Hospitals Complex at 11:15
There was no history of trauma or assault, or of sexual intercourse in the preceding 24 hours. She had no passage of vesicles.
Her menstrual cycle had been regular in the previous 6 months and she had no pregnancy symptoms. She had been diagnosed 17 years earlier with uterine fibroids, and had also been infertile since then.
On examination, she was conscious and restless. There was marked pallor with cold clammy extremities, a pulse rate of 136 beats per minute, and a systolic blood pressure of 80 mm Hg, an unrecordable diastolic blood pressure, a temperature of 350C, and a respiratory rate of 34 cycles per minute.
Her abdomen was grossly distended and moved minimally with respiration. There was generalized tenderness with guarding and rigidity. The liver, spleen, and kidney were difficult to palpate; a 32-week-size hard pelvic–abdominal mass was palpable, but severe tenderness limited accurate determination of its details.
Pelvic examination revealed normal external genitalia with minimal vaginal bleeding; the vagina and cervix looked normal. Cervical motion tenderness was positive on both sides. The pouch of Douglas was full.
A urine pregnancy test was negative; ultrasound scanning was deferred because of the unstable nature of the patient.
A diagnosis of hemorrhagic shock caused by intra-abdominal bleeding was made. The differential diagnosis included acute ruptured ectopic pregnancy, rupture of an ovarian cyst, and perforated typhoid. The patient's blood group was B Rh-positive, packed cell volume was 12%, and HIV screening and hepatitis B antigen screening were negative. Urinalysis was normal. Electrolyte and urea were within normal limits.
The patient was resuscitated with 1 L of normal saline and 1 unit of whole blood. She was put under general anesthesia and an exploratory laparotomy was performed.
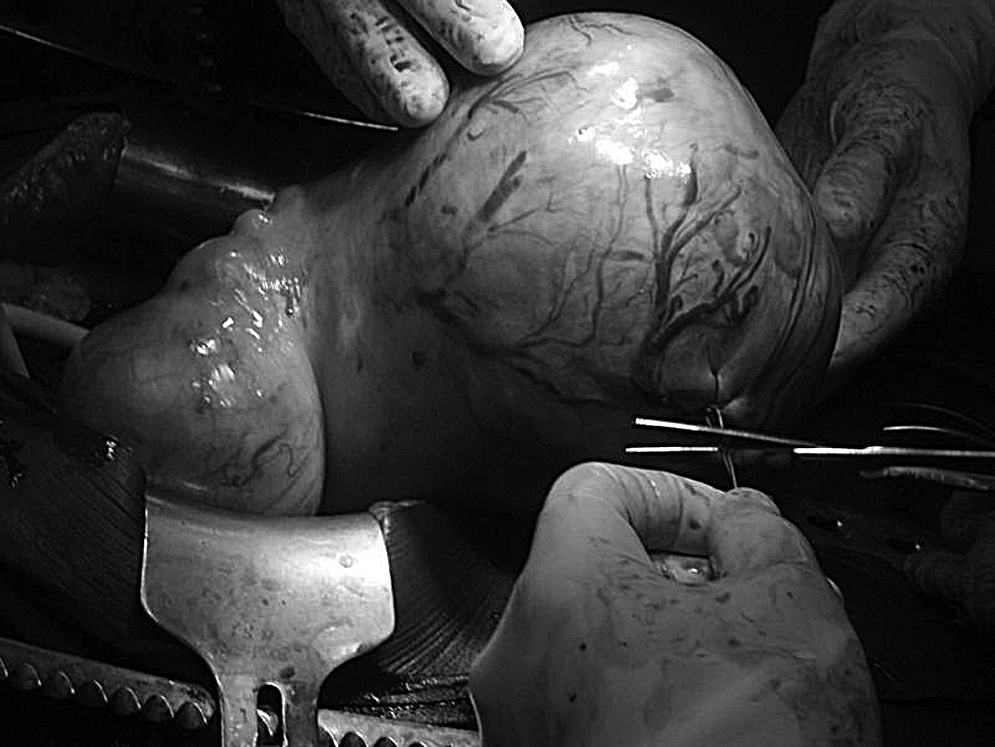
At surgery, 2 L of hemoperitoneum were found, as was an ∼30-week-size multilobular uterine fibroid. There were many dilated superficial vessels seen running over the subserosal fibroids – one of which was bleeding actively (Fig. 1). Hemostatic sutures were applied to control the bleeding (Fig. 2) and the blood was vacuumed out.

Bleeding site from ruptured vessel on a huge fibroid.
Ligated vessel before myomectomy was done.
Visual inspection and manual exploration of the abdominal cavity were performed.
Using an 18 FG Foley's catheter, a tourniquet was applied to the uterus at the level of the isthmus until it blanched. Myomectomy was then performed following the usual surgical procedures; there was no need to encroach into the endometrial cavity, as no submucous fibroid was palpated. The patient received an additional 1 unit of blood intraoperatively.
She received the third unit of blood in the recovery room and an additional unit on the first postoperative day. She had an uneventful postoperative recovery. Cefuroxime and metronidazole were given as postoperative antibiotics. The patient was discharged home on the ninth day with packed cell volume of 32%.
She was followed up in the General Gynecology Clinic. She has had 3 visits, her recent packed volume was 38%, and the abdominal scar had healed well. Histology report confirmed leiomyoma uteri with no evidence of malignancy.
Discussion
Hemoperitoneum in women of reproductive age is commonly caused by ruptured ectopic pregnancy. Other causes include ruptured corpus luteum, adnexal torsion, perforated typhoid, and peptic ulcer diseases, and, in Nigeria, unsafe abortion procedures and ruptured gravid uterus. Uterine fibroid is the most common tumor in females and the most common in the human body. It affects ∼30%–50% of women>30 years of age. 6
Although uterine fibroid is common in women, acute intra-abdominal bleeding from its vascular supply is very rare, 7 the first case being reported by Karl von Rokitansky in 1861, 8 with<100 cases to date. 9 In a review of 53 cases by Buttery, 10 only in 4 instances was the preoperative diagnosis made, and 3 deaths were noted in this series. In all these 3 cases, the patient were pregnant and no surgical intervention was attempted. In the case presented here, the diagnosis was not made until laparotomy. This supports the fact that urgent surgical intervention is both diagnostic and therapeutic.
Management of this problem includes hemostatic sutures, myomectomy, or hysterectomy to control hemorrhage. 11 The more tedious option of myomectomy was preferred to hysterectomy in this patient because consent for such radical surgery was not given, the patient had cultural beliefs and practices that favored preservation of menstrual function until natural menopause, and there was likelihood of better psychological well-being, as she had not had a child.12,13
A number of precipitating factors that can cause rupture of superficial veins traversing a fibroid were highlighted by Deopuria. 11 These include venous congestion during pregnancy, menstruation (as was noticed in this case), straining at stool, lifting a heavy object, uterine manipulation, and coitus. Large fibroids of ≥10 cm in diameter and those located in the posterior uterine wall are at higher risk from traumatic ruptures as they impinge on the sacral promontory. The bleeding is usually venous in origin and can be severe enough to be life threatening (as seen in this case) or can be fatal. Adequate facilities for blood transfusion and general anesthesia with a cuffed endotracheal tube were vital to the success of surgery in this patient with an unprepared stomach (i.e., no preoperative fasting to prevent food from being in the stomach, thus increasing the danger of aspiration during anesthesia).
Conclusions
Spontaneous rupture of a vessel over a fibroid is a rare cause of hemoperitoneum. This condition can be life threatening and should be borne in mind in any woman with fibroid presenting with an acute abdomen and signs of blood loss. Emergency laparotomy is recommended to arrest hemorrhage and establish the diagnosis.
Footnotes
Acknowledgments
The authors thank Uchenna Onwudiegwu of the department of obstetrics and gynaecology, Obafemi Awolowo University, Ile-Ife for helping to revise the original manuscript of this case report.
Disclosure Statement
No competing financial conflicts exist.