
Abstract
Abstract
Introduction
In addition to secondary infertility, frequent symptoms reported by women with this clinical profile include menstrual irregularities, pelvic pain, and expulsion of bone fragments during menstruation. 3
Case
The case of a 32-year-old woman with a 4-year history of secondary infertility who also reported nonspecific abdominal discomfort and polymenorrhea, is presented. Her obstetrical history included nine pregnancies, of which one was a eutocic birth at age 19 and eight were therapeutic abortions through dilation and curettage (D & C). At least two of the abortions were performed in the second trimester.
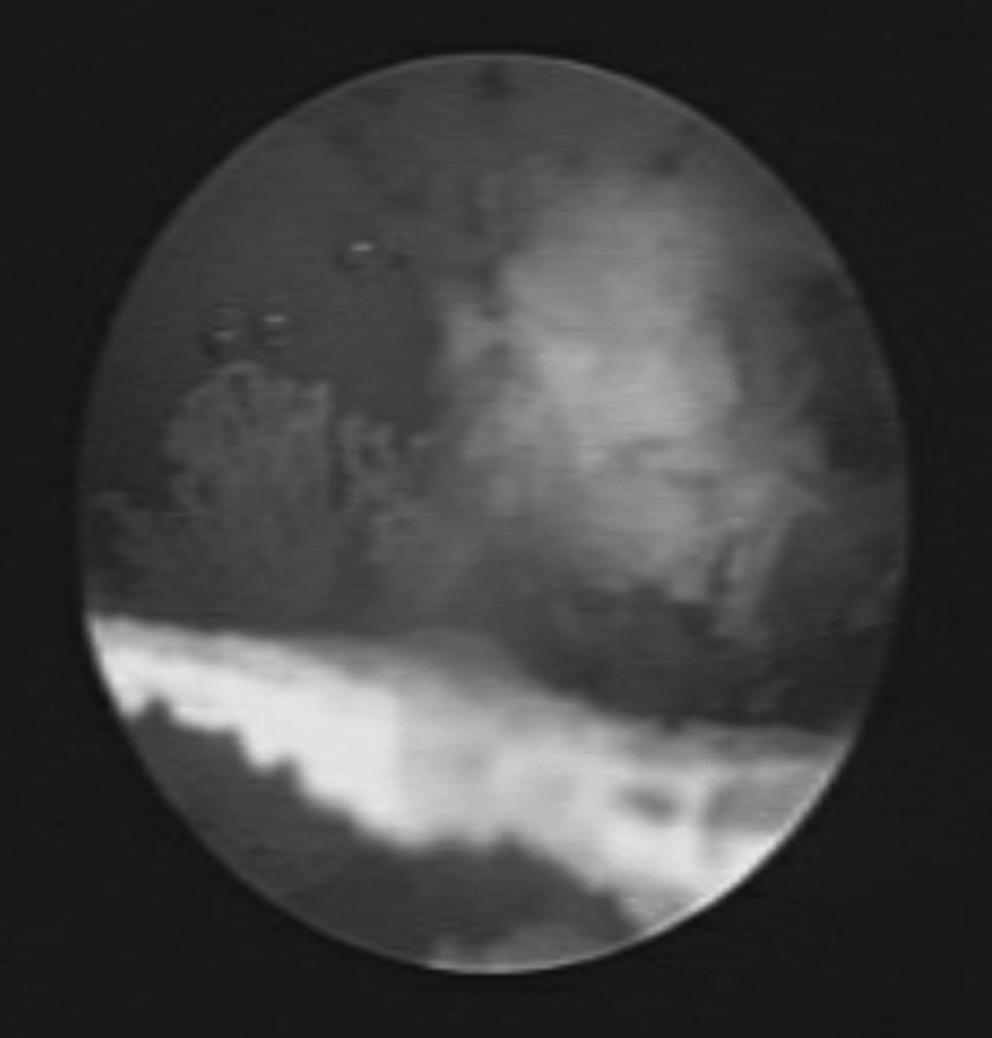
During a transvaginal ultrasound performed in the medical examination prior to the in-depth infertility study, two hyperrefringent linear formations were observed occupying the entire endometrial cavity (Fig. 1). The uterus and adjoining organs were normal.

Two-dimensional transvaginal ultrasound image. Longitudinal uterine cross-section with bone fragments.
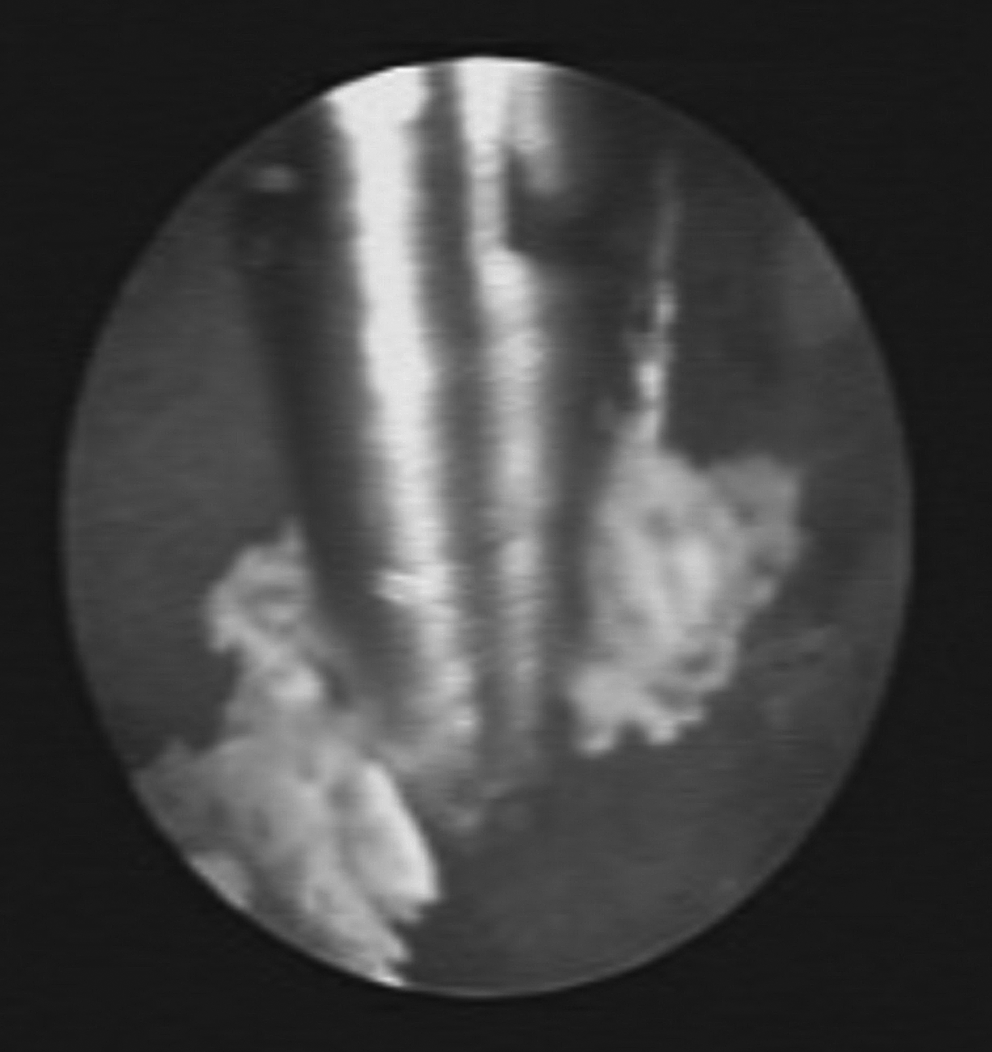
With a suspected diagnosis of retained fetal bone, diagnostic hysteroscopy was performed with a BETTOCCHI® hysteroscope and saline solution as a distension medium. The presence of three bone fragments occupying the base and midline up to the endocervical canal was confirmed. These were found to lie free in the cavity; the endometrium itself presented no abnormalities (Figs. 2 and 3). Complete removal of each of the fragments was performed with forceps (Fig. 4). The patient required no surgical hysteroscopy or any other invasive technique.
Hysteroscopy image. Bone fragments in the uterine cavity.

Hysteroscopy image. Detail of one of the bone fragments.
Hysteroscopy image. Removal of bone fragments.
Histological analysis confirmed the existence of membranous bone measuring 2×0.5 cm in its entirety.
Results
The patient had a spontaneous pregnancy 3 months after the hysteroscopy.
Discussion
Intrauterine bone fragments are an extremely rare finding. The incidence is calculated to be ∼ 0.15% on the basis of 2000 diagnostic hysteroscopies performed on women with menstrual irregularities; in all cases in which bone fragments were found, the women had a history of abortion. 4
Fetal bones retained in the uterus may lead to infertility by means of a foreign body mechanism similar to that of intrauterine contraceptive devices. Moreover, they can interfere with blastocyst implantation by inducing an inflammatory reaction and increasing endometrial prostaglandins.2,5
Two possible explanations for the presence of bone tissue within the uterus are the retention of fetal bone and osseous metaplasia of endometrial stroma. The former tends to be associated with second trimester abortions in which the fetus is already capable of endochondral ossification, making it possible to retain fetal bone in the uterus, even after dilatation and curettage. 6
In incomplete first trimester abortions, however, bone fragments can also be found because of the dystrophic calcification of the fetal remnants or the osseous metaplasia of endometrial stroma cells, both of which are secondary to the chronic inflammation accompanying these processes. The calcifications are similar to those found in myomatose nodules or abscesses. 5 Osseous metaplasia may be distinguished from retained fetal bones by the absence of distinct fetal bones, surrounding tissue reaction, and endochondral ossification. 6
In this case study, two findings pointed to retained fetal bone as the etiologic factor: (1) the histology of the extracted fragments, which indicated the presence of membranous bone found only in the skull; and (2) the appearance of the uterine cavity as observed through hysteroscopy, in which free, noncoralliform fragments were observed.
Transvaginal ultrasound is a good method for performing initial diagnoses and constitutes the best imaging technique in these cases. Although it does not allow for differentiation between retained fetal material and osseous metaplasia, it is highly sensitive and specific in detecting endometrial pathologies. 2 The majority of cases were diagnosed with this technique as opposed to hysterosalpingography (HSG), which is much less sensitive. 3
Moreover, hysteroscopy is the method of choice in these cases because it permits both diagnosis and treatment through removal of bone fragments in the same medical procedure, which can more often than not be performed as an outpatient procedure. 2
Initially, this patient underwent a transvaginal ultrasound. Upon seeing the results and suspecting the presence of retained fetal bone in the uterus, medical staff performed a diagnostic hysteroscopy, both as a diagnostic and therapeutic procedure. This obviated the need for any other diagnostic tests or therapy for the patient's secondary infertility.
Removal of bone fragments is usually associated with a significant decrease in both the volume of menstrual blood and prostaglandin levels. 6 It is also linked to rapid restoration of fertility in ∼ 79% of the cases. 7
In this case study, removal of the retained bone fragments resulted in the end of the patient's abdominal pain and polymenorrhea. The patient became pregnant 3 months after the hysteroscopy.
Conclusions
In summary, a thorough investigation of the endometrium is essential when initiating treatment for secondary infertility, especially in patients with a history of late- term abortions. The ease of diagnosis and treatment that this procedure provides justifies its inclusion in established protocols in order to avoid the necessity of other diagnostic tests in such cases.
Footnotes
Disclosure Statement
No competing financial conflicts exist.