
Abstract
Abstract
Introduction
Case
A 49-year-old, multiparous woman applied to the outpatient clinic with complaints of lower abdominal and vaginal fullness; occasional pelvic pain; a yellow-pink vaginal discharge; and urinary symptoms, such as intermittent voiding, postvoid dripping, and dysuria for several months. She had been menopausal since age 47 and had never used hormone replacement therapy. Her past medical history was not significant for any condition. A speculum examination revealed a solid, globular, yellowish mass, approximately 10 cm in diameter, with an inflamed and ulcerated surface, filling the vaginal space. A foul-smelling purulent discharge was present. The cervix could not be visualized. Pelvic ultrasound showed a 13 × 7–cm solid mass in the vagina. The tumor markers, including CA 125, CA 19-9, and AFP, were all within normal ranges. Removal of the mass was recommended, but hysterectomy was preferred by the patient after she completed a detailed informed consent form.
With a presumptive diagnosis of a submucous leiomyoma, an exploratory laparotomy was performed. Laparotomy revealed a barrel-like bulging extending from the uterine isthmus to the vagina and a dimple at the uterine fundus, probably representing traction of the leiomyoma. Both ovaries, other pelvic and abdominal structures, and peritoneal surfaces were all grossly normal. Total hysterectomy and bilateral salpingo-oopherectomy operations were performed in a manner similar to that of a standard hysterectomy until the phase of uterine arterial dissection. However, following ligation and dissection of her uterine arteries, a circumferential incision was performed at the level of the uterine isthmus, and the mass was delivered from the vagina with rotational movements and totally removed, together with the uterine corpus (Fig. 1). During this procedure, it was observed that this patient's uterine cervix was completely dilated in a manner that appeared to be similar to the cervical changes observed during labor, and the vaginal fornixes were completely dialated. Following this, the sacrouterine and cardinal ligaments were dissected, and an approximately 3-cm tissue part, which was thought to originate from the cervical stump, was removed via a circular incision, and the vaginal cuff was closed accordingly. Gross examination of the surgical specimen revealed a solid mass, approximately 15 cm in its long diameter, originating from the uterine fundus with a thick peduncule (Fig. 2). Histopathologic evaluation of the mass confirmed that the mass was a leiomyoma with degeneration and inflammation. The patient's postoperative course was uneventful and she was discharged without complications on the third postoperative day.
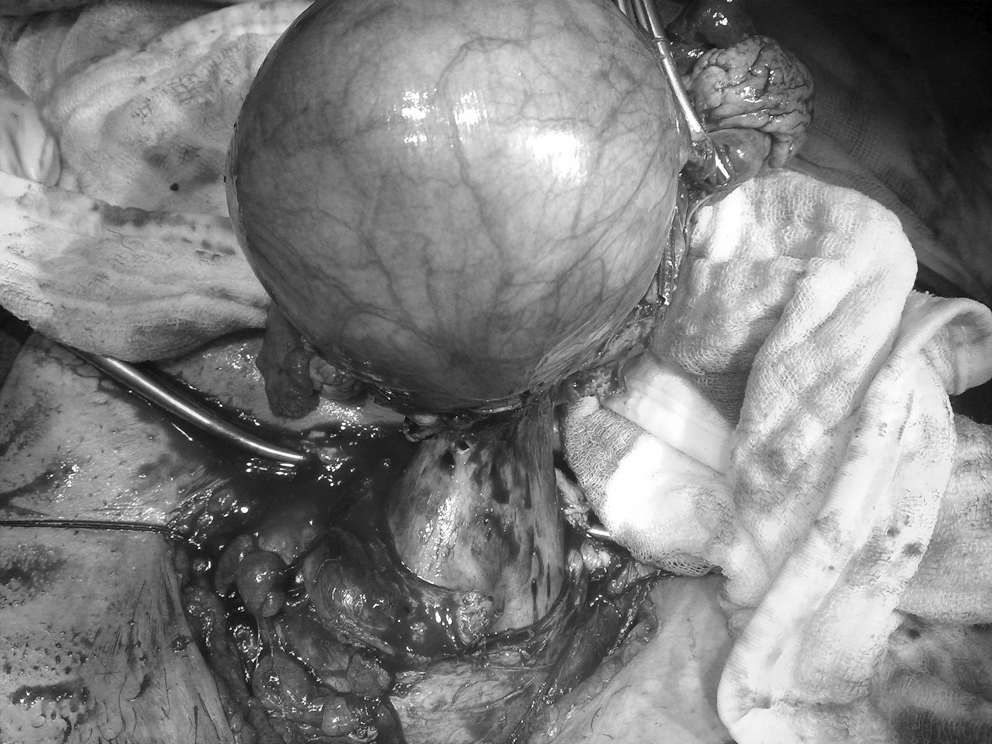
Intraoperative view—delivering the mass with the uterine corpus.

Surgical specimen—the removed mass with the uterus.
Discussion
Classification of submucous myomas is based on the degree of the myoma within the cavity. According to this classification, a pedunculated submucous myoma is classified as type 0 submucous fibroid tumor. 2 Vaginal myomectomy is generally recommended as the most appropriate initial treatment for relatively small, prolapsed, pedunculated, submucous myomas. Suggested vaginal myomectomy techniques for treatment of pedunculated leiomyomas include hysteroscopic resection of the peduncle, nonhysterescopic cutting or twisting of the peduncle, and morcellation or vaporization of the myoma nodule.3,4 In the series of Golan et al., consisting of 46 patients with a preoperative diagnosis of pedunculated myoma, vaginal myomectomy success was reported to be high (95%). The researchers concluded that vaginal myomectomy is the treatment of choice for prolapsed, pedunculated, submucous myomas as the operation is short, simple, definitive, and, in most cases, carries minimal morbidity risk for the patient. 1
However, vaginal myomectomy would not be an easy operation for addressing a thick, pedunculated, very large myoma, as in the present case illustrated. The primary obstacles of such an operation would be heavy bleeding from the myoma, inadequate space for working, and a remnant myoma node. 3 Nonetheless, in young patients, Kanaoka et al. defined an intranodal morcellation technique utilizing a loop electrosurgical excision procedure for such prolapsing, pedunculated submucous myomas, which are very large in size. 5 Together with this, abdominal approach would be an easier technique if the preferred operation is a hysterectomy. In the present patient, the technique used involved abdominally delivering the myoma, which was removed with the uterus, and, as the mass dilated the cervix completely, the procedure was applied more easily. However, in cases with larger masses and/or when cervical dilation is not sufficient, separating the peduncle from the mass and removal via the vaginal route can be preferred.
Conclusions
In conclusion, abdominal hysterectomy would be a reasonable option with a lower complication rate. This technique is also easier for addressing thick, pedunculated, very large, protruding submucous myomas filling the vaginas of menopausal patients.
Footnotes
Disclosure Statement
No competing financial interests exist.