
Abstract
Abstract
Introduction
Case
A 17-year-old primigravida was referred to Jawaharlal Institute of Postgraduate Medical Education and Research as a case of miscarriage at 19+3 weeks' gestation following failed attempts at evacuation. She gave a history of lower abdominal pain, and after an ultrasound, a diagnosis of miscarriage was made. There was no history of bleeding per vaginum. The patient had undergone dilatation and evacuation twice, the first was followed by bougie and misoprostol. On examination, her general condition was satisfactory and bimanual pelvic examination revealed a 14–16 week sized nontender mass, which appeared to be mobile with the uterus. Her blood tests were normal. Ultrasonographic examination showed an extrauterine dead fetus corresponding to 13+3 weeks' gestation, surrounded by localized fluid collection (Fig. 1) and a 6×5 cm mass by the right side of the fetus suggestive of placenta, with minimal free fluid in the abdomen. The preoperative diagnosis was a secondary abdominal pregnancy and laparotomy was planned.

Ultrasound showing an extrauterine dead fetus corresponding to 13+3 weeks' gestation, surrounded by localized fluid collection.
Laparotomy revealed a ruptured noncommunicating rudimentary horn pregnancy and 200 mL hemoperitoneum. Gestational sac of 8 cm size with a 15 g macerated fetus was lying inside the peritoneal cavity adherent to the bowel and omentum. The fetus was removed with the placenta and the ruptured rudimentary horn was excised (Fig. 2). Both ovaries were normal.
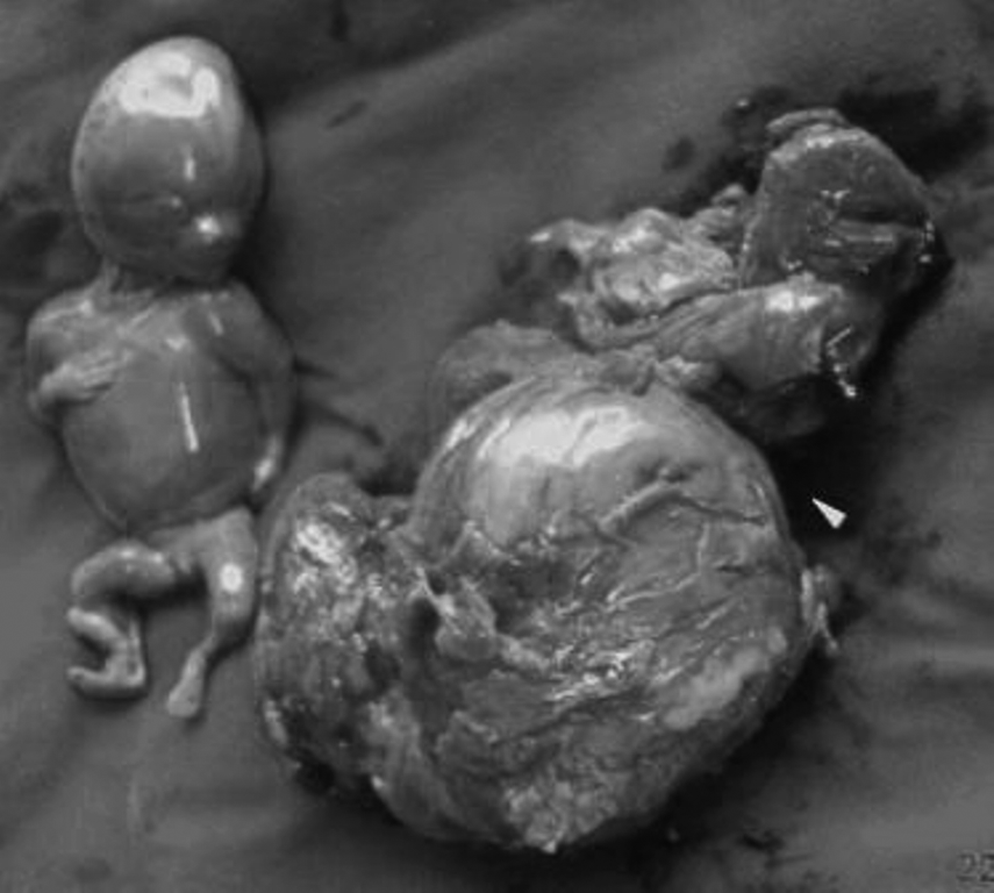
Gross morphology of fetus and excised ruptured rudimentary horn (arrowhead).
Results
The patient's postoperative period was uneventful. Ultrasound revealed no renal tract anomalies. Histopathology revealed infarcted villi with decidua and underlying muscular tissue with chronic inflammation.
Discussion
Most of the patients with ruptured rudimentary horn present with acute abdomen, and the main complication is hemorrhage, which can be life threatening. This patient was clinically stable at presentation. In 90% of cases, rudimentary horn pregnancies rupture most commonly before 20 weeks' gestation, and 10% of pregnancies may proceed to term with 2% fetal salvage rate. 5
Though uterine anomalies can be suspected on bimanual or ultrasonographic examination, these can be diagnosed in only 14% cases before they become symptomatic.3,6 In a review of 266 rudimentary horn presentations (210 gynecologic and 156 obstetric), sensitivity of ultrasound as a diagnostic tool was shown to be 26%. 6 Diagnosis by imaging studies is difficult, and <5% of cases have been diagnosed preoperatively. 7 Ultrasonographic criteria for early sonographic diagnosis include: 1) a pseudopattern of an asymmetrical bicornuate uterus, 2) absent visual continuity between the cervical canal and the lumen of the rudimentary horn, and 3) the presence of myometrial tissue surrounding the gestational sac. 3 Magnetic resonance imaging might also be helpful in suspected cases of rudimentary horn pregnancy, as it localizes the area of implantation of the placenta and its vascular supply because of its high resolution. 8 These patients should also be screened for renal tract anomalies, the incidence of which varies from 1.8 to 37.6%. 9
Use of labor induction agents for termination of pregnancy in a rudimentary horn is unsuccessful and can even lead to rupture of the horn, as reported by Samuels, which is similar to the patient described here. 10 Treatment is excision of the rudimentary horn either by laparoscopy, if facilities are available, or laparotomy. 11 The delay in treatment in this case was the result of the initial ultrasound diagnosis having been wrong. Hence a careful examination of the uterine contour is advocated in every case, to avoid a misdiagnosis of this rare catastrophic condition.
Conclusions
An unusual clinical presentation, such as in this case, should alert the obstetrician to consider the possibility of an ectopic pregnancy. A detailed ultrasound will definitely help in making a preoperative diagnosis, so that prompt treatment may be initiated.
Footnotes
Disclosure Statement
No competing financial conflicts exist.