
Abstract
Abstract
Introduction
Case 1
A 46-year-old para 5 whose last child was born 23 years ago presented with polymenorrhagia for the last 6 months. She had been suffering from non-insulin-dependent diabetes mellitus for the past 10 years and hypertension for the past 2 years, and was on regular treatment for these conditions. She recovered from a cerebrovascular accident involving the right cerebral hemisphere, which occurred 7 months previously. Her father was diabetic, and her mother had carcinoma of the stomach.
On examination, she was well built, weighing 63 kg, and had mild pallor. Her blood pressure was 130/80 mm Hg. She did not have significant lymphadenopathy, and her breasts and thyroid were normal. An abdominal examination revealed a right paramedian subumbilical vertical scar with a small incisional hernia due to a previous cesarean section. Per speculum examination revealed a small polyp of 2×3 cm at the endocervix, and there was bleeding through the cervical os. Bimanual pelvic examination showed a parous uterus without any palpable adnexal masses. A polypectomy was performed in the outpatient department. Histopathological examination of the polyp reported a low-grade ESS (Fig. 1).
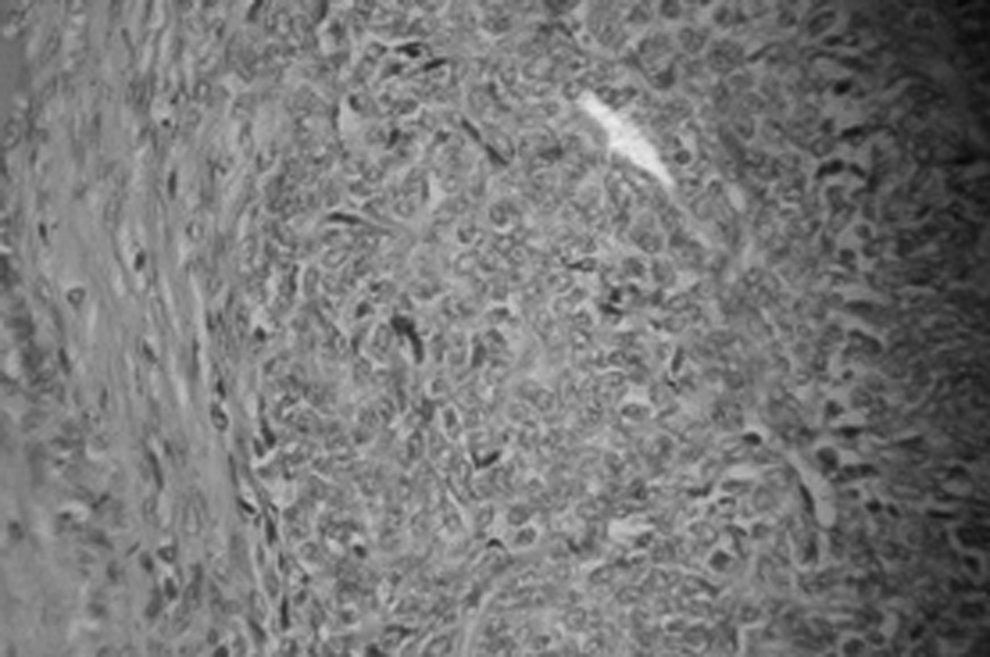
Histopathological picture showing sheets cells uniformly arranged, resembling proliferative phase endometrial stroma/low-grade endometrial stromal sarcoma.
Transvaginal ultrasonography did not show any mass in the endometrium, myometrium, or adnexa. The uterus measured 8×4 cm, the endometrial thickness was 10 mm, and ovaries could not be distinguished. The mode of therapy was discussed with the radiotherapists and oncologists, and the plan was to perform a total abdominal hysterectomy and bilateral salpingo-oophorectomy followed by radiotherapy and hormone therapy.
Her hemogram, liver function tests, renal function tests, ECG, and chest x-ray were normal. Fundus examination showed nonproliferative diabetic retinopathy. Her blood sugar was controlled by adding an injection of human Mixtard® (Insulin Injection-Insugen, Biocon, Bangalore) to the oral hypoglycemic agents that she was already taking. On laparotomy, the uterus was bulky, the right tube and ovary were normal, the left ovary was absent, the left tube showed a 4×3 cm hydrosalpinx. There was also a 0.5 cm paraaortic node, which was insignificant. A total abdominal hysterectomy and right salpingo-oophorectomy and left salpingectomy was performed. The cut specimen showed a growth in the endometrium (Fig. 2). The postoperative period was normal. The histopathological examination did not reveal any evidence of ESS, and adenomatous hyperplasia was reported. The preoperative slides of the polyp were reviewed, and the opinion of all the consultants in the pathology department was that this was a case of low-grade ESS.

Picture of hysterectomy specimen of Case 1 showing thickened endometrium, which was reported as adenomatous hyperplasia.
Case 2
A 38-year-old para 3 who was tubectomized 12 years ago following the birth of her last child complained of pain in the lower abdomen and excessive bleeding per vaginum for the previous 4 months, prior to which she had been asymptomatic. Her flow lasted for 20 days and occurred once every 30 days. Her previous cycles had been regular, with the flow lasting for 3 days and occurring once every 30 days. There was no history of bleeding diathesis, and there was no family history to suggest malignancies.
Her general health was good, and she weighed 49 kg. There was no significant lymphadenopathy, and her breasts and thyroid were normal. Her respiratory and cardiovascular systems were also normal. Per abdominal examination revealed an irregular midline mass, 24 weeks in size, arising out of the pelvis, and another firm 8×10 cm mass in the right iliac fossa, felt separately from the midline mass. On per speculum examination, the cervix and vagina appeared healthy, and on per vaginal examination the uterus was found to be continuous with the abdominal mass, which was firm to hard and nodular, and the movements of the mass were transmitted to the cervix. A provisional clinical diagnosis of uterine fibroids was made, and she was investigated for take up for surgery. After 4 days, she attended the emergency department with sudden gross swelling of the right lower limb for 5 hours. She was examined by physicians, and the clinical impression was deep venous thrombosis (DVT) of the right lower limb. Emergency compression ultrasonogram (USG) showed a noncompressible right femoral vein and a compressible right popliteal vein. She was started on anticoagulants after admission to the medical ward. Repeat USG after 6 days showed a noncompressible right femoral vein, with evidence of echogenic fossi noted with a length of 3.7 cm extending into the right long saphenous vein. The right popliteal vein dilated and was partly compressible. The patient was started on warfarin, and a prothrombin time (PT INR) was maintained between 1.8 and 2 seconds. The patient was then discharged.
Two months later, a contrast enhanced computed tomogram (CECT) reported the following. The uterus measured 11.3×9.2 cm replaced by a large hyperdense lesion with multiple anechoeic areas within the necrotic fibroid. There was a 11.5×9.5 cm complex mixed echogenic cystic lesion with internal septations seen to the right side of the uterus and inseparable from it.
Compression USG after 3 months showed that the right femoral vein wall had thinned out and was not totally compressible; the right short saphenous vein was dilated, and the right popliteal vein was not fully compressible. She was hospitalized and heparin injection was started. A repeat Doppler after 3 weeks showed the bilateral femoro-popliteal veins to be compressible. Her hemogram showed a hemoglobin of 9 g/dL. Bleeding time was 2 minutes 5 seconds, clotting time was 6 minutes 40 seconds, and PT INR was 1.23. APTT (control 33.4 seconds, test 31.5 seconds) platelet count was 378,000/mm3, total WBC count was 8,000-N 78,L 32 and a peripheral smear showed normochromic normocytic RBC with mild anisocytosis. Her liver function tests and renal function tests were normal. HIV and Hbs Ag were negative. Her lipid profile showed a serum cholesterol of 151 mg/dL, triglycerides of 91 mg/dL, an HDL of 38 mg/dL an LDL of 100 mg/dL, and a VLDL of 18 mg/dL. Her CA-125 level was 10 IU/mL.
A chest x-ray and ECG were normal. Laparotomy performed under general anesthesia showed 20 weeks in size uterus with a bilobed mass of 15×10 cm and 10×8 cm arising from its right side (Fig. 3). The right ovary could not be distinguished. The left ovary was normal. The right ovarian vessels and right uterine vessels were enlarged (Fig. 4), and their lumen contained white jelly-like material. Paraaortic nodes were enlarged to 2×2 cm and were hard on palpation. There were multiple small nodes in the root of the mesentery. Both ureters were dilated, the right more so than the left. There was no ascites. Total abdominal hysterectomy with bilateral salpingo-oophorectomy, along with infracolic omentectomy and biopsy of the paraaortic lymph nodes, was performed. The intraoperative diagnosis was uterine sarcoma. She received two units of fresh frozen plasma and one unit of packed cells. Her postoperative course was normal. Heparin was stopped and warfarin was started on the 5th postoperative day. Her histopathological examination reported low-grade ESS; Vimentin, CD 10, PR positive by immunohistochemistry. The tumor had infiltrated the cervix, right fallopian tube, right broad ligament, and the thick-walled blood vessels in the right broad ligament and right-sided parametrium. There were multiple tumor emboli in the lymphatics. The right ovary could not be distinguished. The left tube and ovary were normal. Paraaortic nodes showed reactive changes. The omentum was normal. The patient was readmitted after 3 weeks when the histopathological report was ready, and she was evaluated for radiotherapy and chemotherapy. However, she absconded 3 days after admission.

Case shows a uterine tumor in the center and a bilobed tumor arising from the right side of the uterus with omental adhesions.

Case 2. The artery forceps point to the enlarged infundibulopelvic vessels.
Discussion
Low-grade ESS is defined as an infiltrative stromal tumor with less than 10 mitoses per 10 high-power fields. These low-grade ESS are termed simply as endometrial stromal sarcomas. Endometrial sarcomas without definite evidence of stromal phenotype are designated as poorly differentiated endometrial sarcomas and are invariably high grade. 2 They have worm-like extensions that usually grow and extend into large vascular spaces. They are very slow growing tumors, but distant as well as local metastasis is reported even after 10 years. 3
It is difficult to make a diagnosis preoperatively based on clinical presentation, and only histopathological examination confirms the diagnosis. 4 In our first case, the preoperative diagnosis was possible because of the biopsy of the polyp. Most patients are in the perimenopausal age group and present with abnormal uterine bleeding and pain or are diagnosed with uterine fibroids.1,3,4 These features were observed in both of our cases.
Diagnostic difficulties occur at surgery and also during histopathological examination.2,4 This was especially true in the second case, as at surgery we thought this may be a case of intravenous leiomyomatosis because we could see white, gelatinous worm-like extensions in the ovarian and other pelvic veins. Low-grade ESS extending intravenously up to the right atrium of the heart was reported by Gabal et al. 5
This intravenous extension must have been misdiagnosed as DVT in our second case. The histopathological examination needed to be confirmed with immunohistochemical studies. Most of the ESS stained positive for CD 10, ER, PR, and bcl-2, and none of them expressed epithelial membrane antigen or CD 34. 6
The prognosis is usually very good ranging from 62% 7 to 93%. 1 Early tumor stage, low myometrial invasion, and low mitotic counts are good prognostic factors associated with long-term survival.1,7
Conclusions
The first case is atypical in the sense that the diagnosis could not be established after hysterectomy. In this case, the polyp alone could have undergone sarcomatous change. The second patient is also atypical in that the intravenous extension of the stromal sarcoma was diagnosed as DVT.
Footnotes
Disclosure Statement
No competing financial interests exist.