
Abstract
Abstract
Introduction
Case
A 32-year-old multiparous women who was tubectomized 4 years ago was referred to our Institute as a case of uterine fibroids, with an ultrasound report suggestive of a subserous fibroid 15.5×13.5 cm in size showing mixed echogenicity and degenerative changes. She had complained of continuous pain in her abdomen for the previous 2 months without any other associated symptoms. Her menstrual cycles were regular, the flow lasting for 3 days and occurring every 30 days, and her last menstrual period was 1 month prior.
On general examination, she was of average built and had no pallor or lymphadenopathy. Examination of other systems was normal. Per abdominal examination showed a firm mobile non-tender mass 24 weeks in size arising out of her pelvis. Per speculum examination revealed a normal cervix and vagina, and on per vaginal examination, the uterus was found to be irregularly enlarged to 24 weeks with the movements of the abdominal mass transmitted to the cervix. Her Pap smear report was normal. A provisional clinical diagnosis of uterine fibroids was made, and she was taken up for surgical management. At laparotomy, there was a highly friable and vascular 30×16 cm mass present on the superior surface of the bladder and uterus, distending the uterovesical fold. The mass was enucleated piecemeal; rather, it came out piecemeal spontaneously after opening the peritoneum of the superior surface of the bladder. There was a large raw area in between the anterior surface of the lower part of the uterus and the posterosuperior surface of the bladder (Fig. 1). Both tubes and ovaries were normal. There was no free fluid. A urologist's opinion was sought on table to rule out the possibility of a soft tissue tumor arising from the bladder. Other abdominal organs were explored and were found to be normal. Frozen section biopsy reported a spindle cell tumor of smooth muscle origin with high cellularity, suggesting malignancy. A provisional surgical diagnosis of leimyosarcoma from the soft tissue was made. She received two units of blood transfusion intraoperatively and another unit of packed cells and fresh frozen plasma postoperatively. Her postoperative course was normal. The histopathological indicated an extraskeletal PNET (Fig. 2). Tumor cells showed areas of necrosis with a mitotic rate of 12/10 HPF and positive for PAS and IHC, Vimentin, and CD99. They were negative for SMA, Desmin, EMA, Cytokeratin, S100, Neuron specific enolase, CD117, mekin A, and HMB 45. Bone marrow aspiration biopsy performed 6 weeks after surgery was reported to be normal. She was started on VAC+Ifosfamide and a contrast enhanced computed tomogram (CECT) of the abdomen performed 2 months after surgery revealed a 4.2×3.3 cm enhancing thin-walled hypodense lesion near the left adnexa with a loculated collection of fluid of 4.8×2.4 cm along the anterior border of the left psoas muscle. There was no focal lesion in the uterus and cervix, and other pelvic organs and bones were normal. It was planned to give four cycles of VAC+Ifosfamide followed by radiotherapy. A CECT thorax performed 4 months later was normal. However, the patient was lost to follow-up after three cycles of chemotherapy. She returned 6 months later, presenting with distension of the abdomen, pain in the abdomen, breathlessness, and a loss of appetite for the previous 2 weeks. Her general health was poor. She had moderate pallor and no lymphadenopathy. Her abdomen was distended with a mass 18 weeks in size occupying the left lumbar region and left iliac fossa with free fluid.
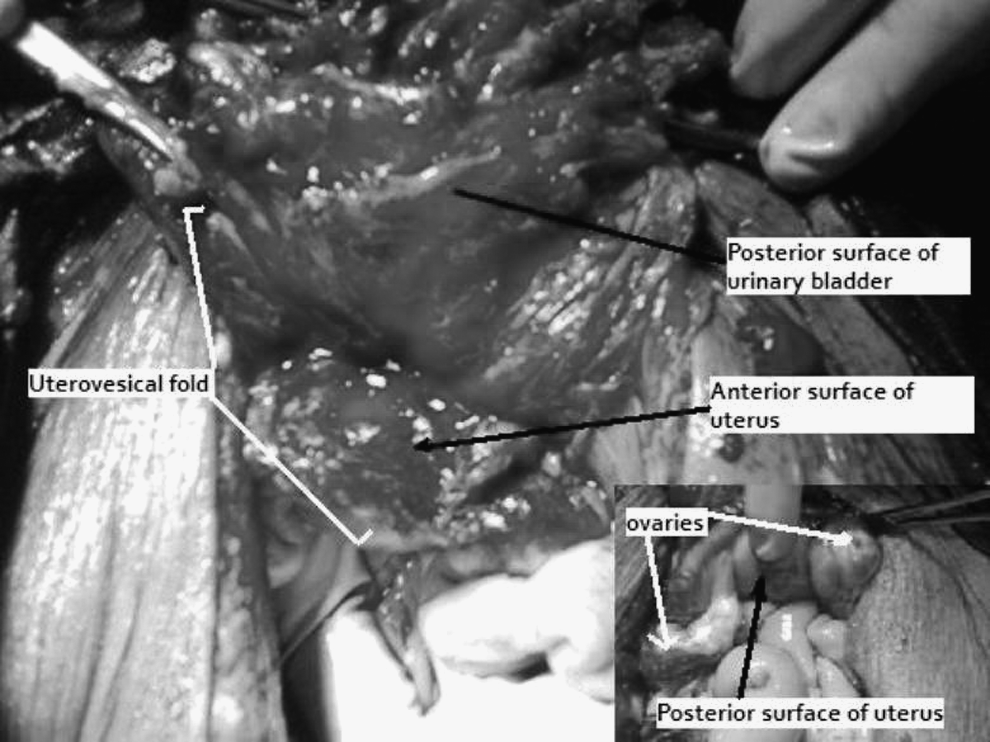
Operative picture showing the raw area between the anterior surface of the uterus and the postero-superior surface of the bladder after piecemeal removal of the tumor mass. The insert shows the normal posterior surface of the uterus and ovaries.
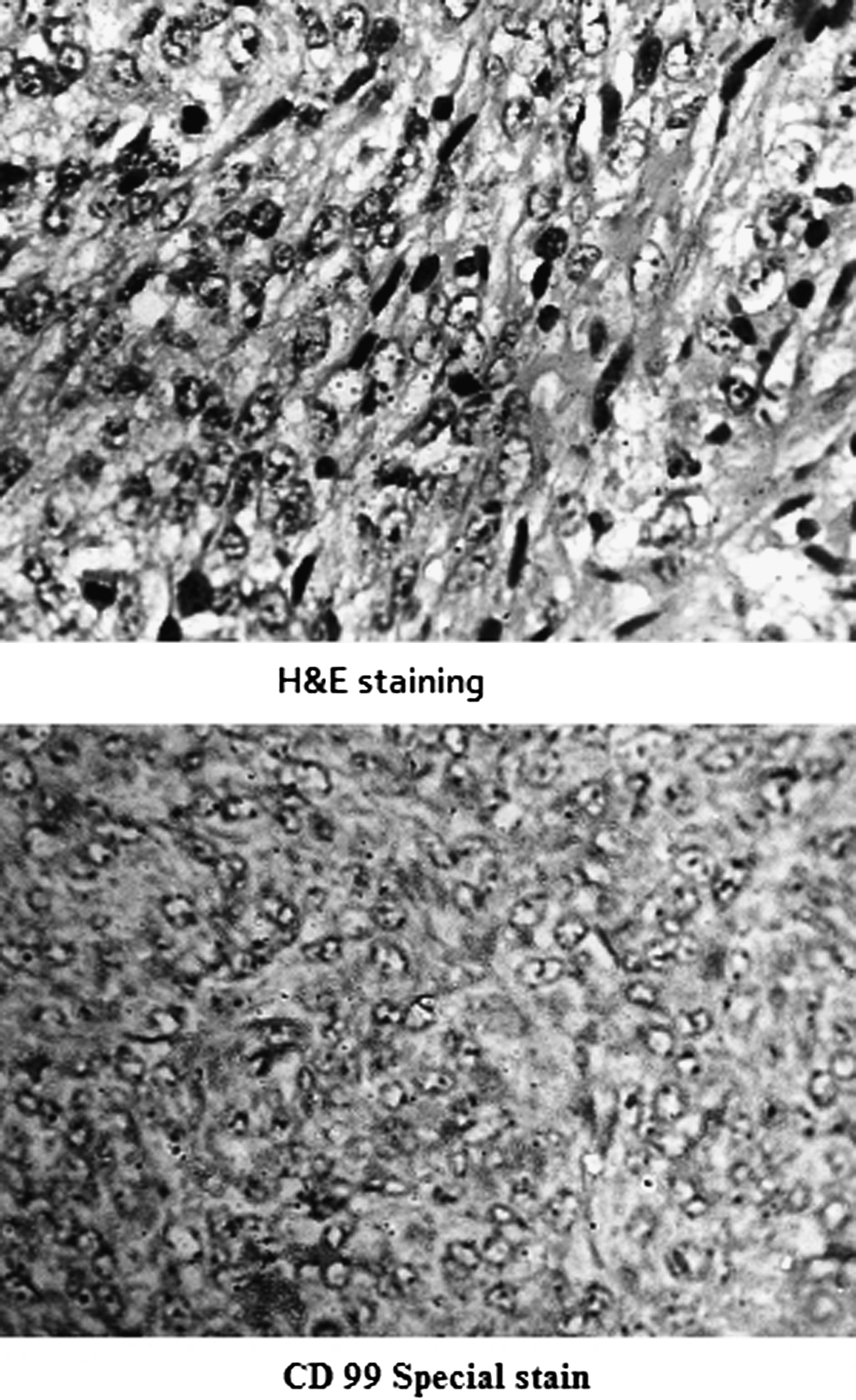
Hematoxylin and eosin staining of the tumor showing round to spindle-shaped cells with mitotic figures and the CD99 stain positivity of the cytoplasm confirming the diagnosis of a primitive neuroectodermal tumor.
Ultrasonogram (USG) of the abdomen (Fig. 3) showed echogenic ascites and a large mass of varying echogenecity. Her hemogram revealed a hemoglobin of 7.8 g/dL with microcytic hypochromic anemia and a platelet count of 1,5,000/mm3. Her blood urea was 115 mg/dL and S. creatinine was 2.9 mg/dL; total bilirubin was 3.8 mg/dL, and direct bilirubin was 1.5 mg%, AST-140 IU; ALT 40 IU and Alkaline Phosphatase was 120 IU. Her chest x-ray was normal. Dehydration was corrected, and she was transfused with one unit of packed cells. The prognosis was explained and further therapy was planned, but the patient left against medical advice.
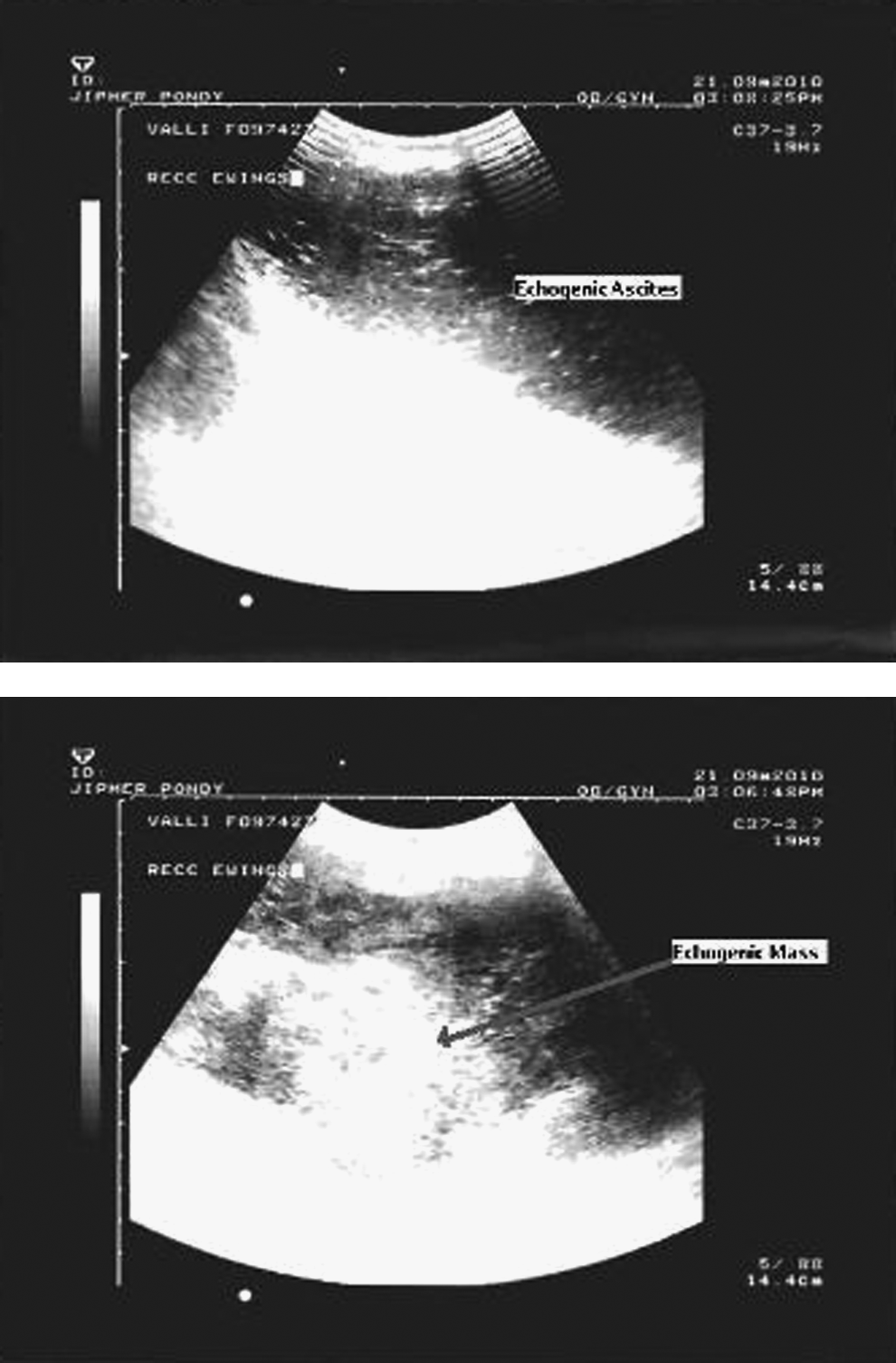
Ultrasonogram (trans-abdominal sonography) showing the recurrence of the tumor after three cycles of chemotherapy, with echogenic ascites with highly echogenic tumor without any distinct capsule.
Discussion
Extraosseous PNET typically involves the soft tissues of the chest wall, pelvis, paravertebral region, abdominal wall, retroperitoneal region, and extremities of children, adolescents, and young adults, but it seldom occurs in the female genital tract. 1 The presenting symptoms of genital tract Ewing's sarcoma usually include mass, pain in the abdomen, and menorrhagia when it involves the uterus 2 and dysparunea when it involves the rectovaginal septum and vagina.3,4
A case of vaginal PNET that metastasized to scalp, skull, and dura was reported by Yip et al. 1 Another reported case of a small (5×6 cm) vaginal PNET was successfully treated by wide local excision and total abdominal hysterectomy, chemotherapy, and radiotherapy. 3 The first report of Ewing's sarcoma involving rectovaginal septum was reported in 20024 and that of the cervix in 1998. 5
Of the retroperitoneal soft tissue sarcomas, liposarcomas were found to be the commonest followed by leiomyosarcomas, and the majority (62%) were found to be low grade. But recurrence was observed to be common after local excision. 6 The present case was thought to be leiomyosarcoma of retroperitoneal tissue of the uterovesical fold and a second surgery was planned after definitive diagnosis and possible chemotherapy. Ewing's sarcoma is an aggressive tumor, 2 but survival was found to be better with multimodality treatment.3,4,7.Ifosfamide and Adriamycin premedicated by Granisetron were found to be safe, even during pregnancy. 8 The present case received Vincristin, Adriamycin, and Cyclophosfamide and Ifosfamide and did not suffer any side-effects until the third cycle. Local tumor control can be achieved after administration of a total dose of 60 Gy in 30 fractions by external beam 60 Cobalt radiotherapy. 9 This patient was uneducated (illiterate), and after feeling the well-being during therapy, she thought she was cured and defaulted on the therapy. She returned of her own accord only after developing distension of abdomen. However, after explaining the prognosis, she refused any kind of therapy.
Conclusions
Extraosseous Ewing's sarcoma is a very aggressive tumor, and when it occurs in the uterovesical fold, it may be misdiagnosed clinically and sonologically as a uterine fibroid because of its consistency.
Footnotes
Disclosure Statement
No competing financial interests exist.