
Abstract
Abstract
Introduction
Case 1
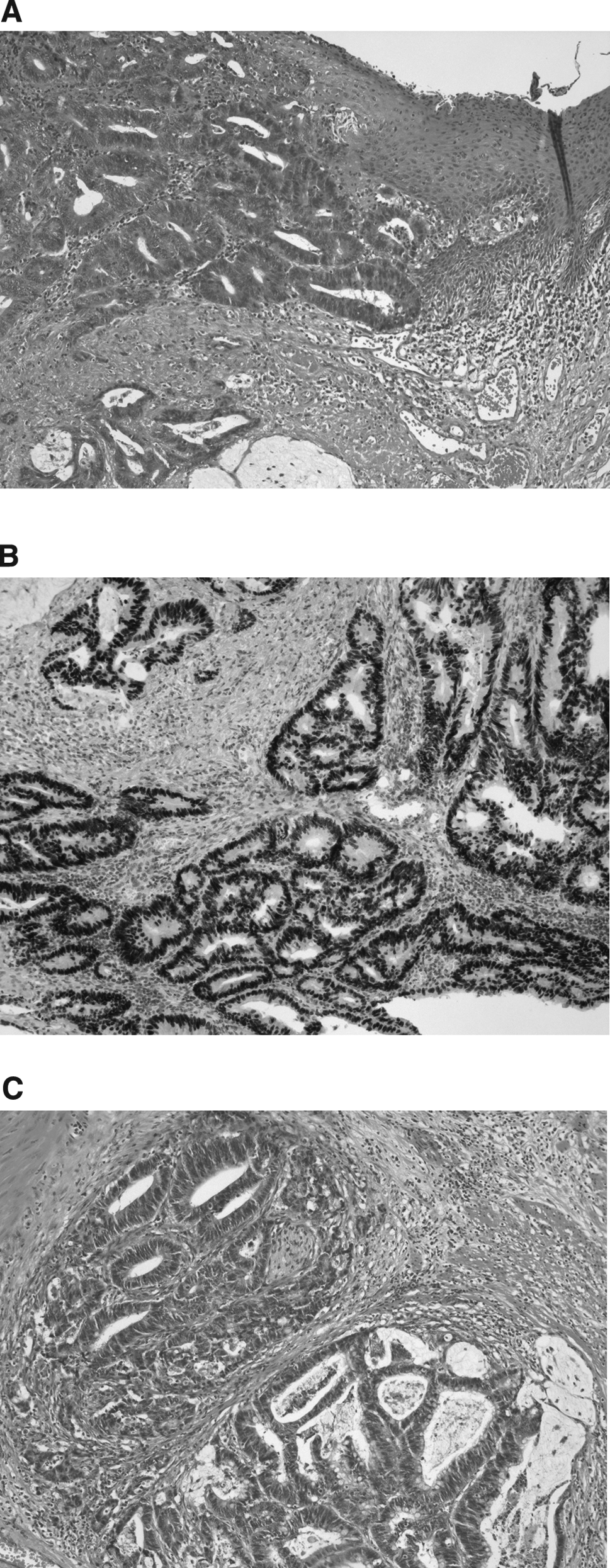
A 76-year-old woman with an unremarkable medical history was referred to the gynecologic oncology department because of an adenocarcinoma of her vulva. Inspection (Fig. 1) revealed a 2 cm lesion in the posterior vulva with a moist aspect. Gynecologic and rectal examinations were unremarkable. The biopsy showed an atypical glandular proliferation compatible with adenocarcinoma. The immunohistochemical profile showed positive keratin 20, CDX-2, pan-keratin, and focal p16. The tumor was negative for keratin 7, progesterone, and estrogen. The possibility of a metastasis from the colon was suggested. An MRI showed discrete thickening of the left rectal wall without enlarged lymph nodes. On sigmoidoscopy, a 4 cm large tumor was identified at 15–19 cm from the anus, and was biopsied. Histology showed adenocarcinoma similar to the vulvar lesion. An uncomplicated low anterior resection combined with a wide local excision of the vulvar tumor was performed. Histology confirmed the diagnosis of colorectal adenocarcinoma with metastasis in the vulva (Fig. 2A–C). Additional immunohistochemical and molecular analyses revealed identical aberrations in both tumors, indicating the clonal relationship between both lesions. The adenocarcinomas in both the colorectum and the vulva showed comparable strong nuclear p53 expression and in both lesions identical p53 and KRAS gene mutations were found. In addition, an identical loss of heterozygosity (LOH) pattern was found in both tumor locations with six polymorphic DNA microsatellite markers on four different chromosomes. The patient was followed-up for 1 year, and no evidence of disease was found.
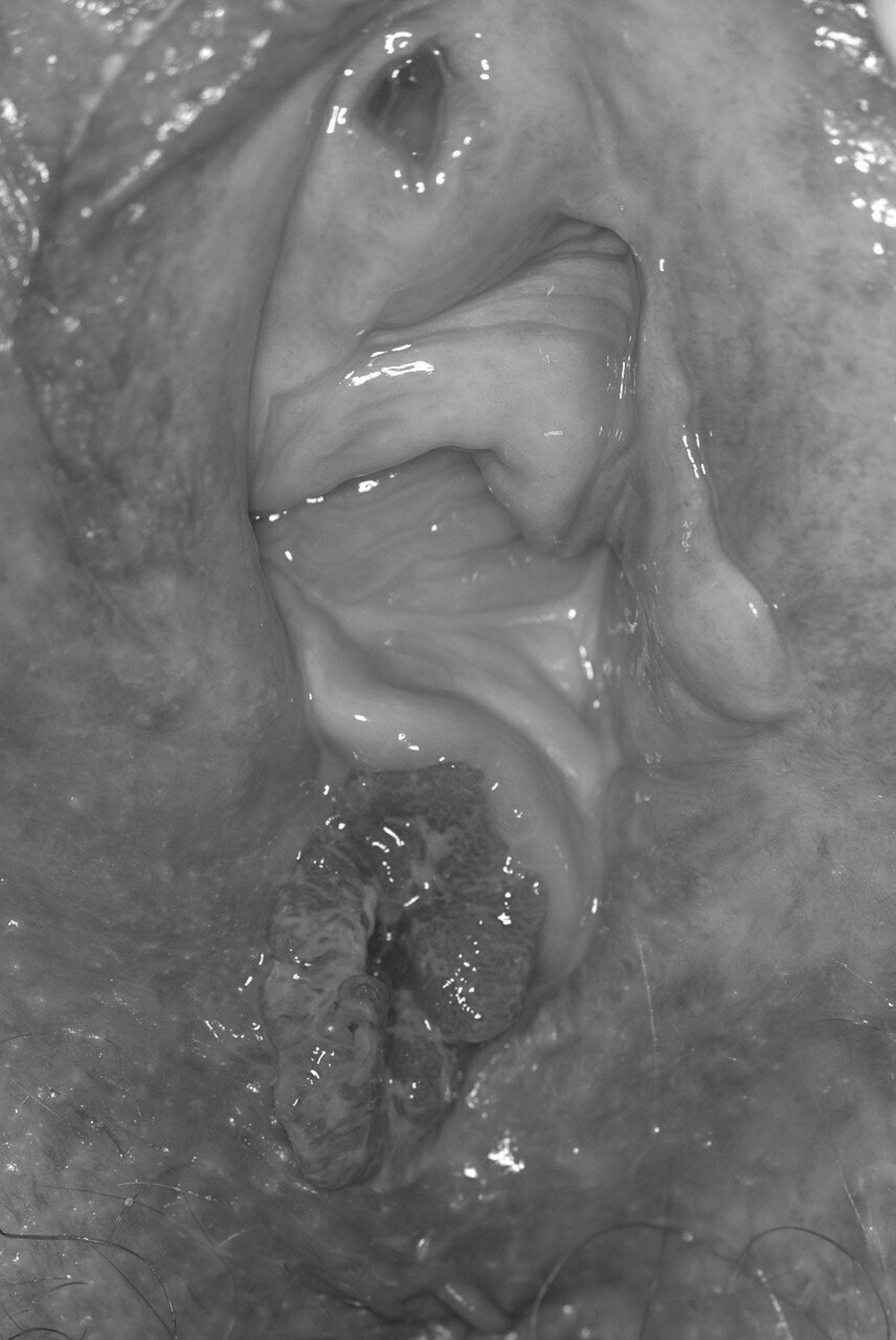
Metastasis of rectal carcinoma in the vulva.
Case 2
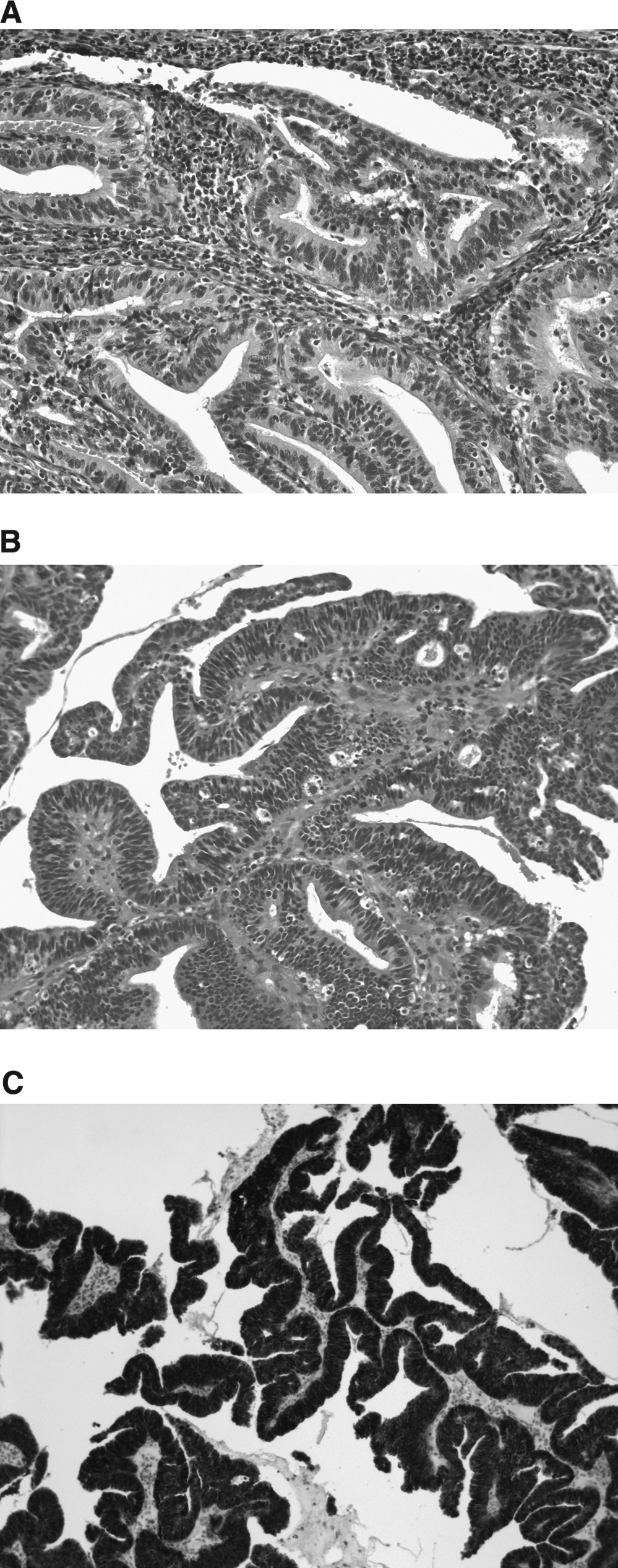
A 45-year-old woman with a history of breast cancer (T2N1MX grade 3) experienced continuous vaginal blood loss. A 2.5 cm polyp-like tumor was found on the cervix. Biopsy showed an invasive adenocarcinoma compatible with adenocarcinoma of the cervix. The tumor was staged Figo IB1. A radical hysterectomy with lymph node dissection was performed. Histology showed a moderately differentiated adenocarcinoma of the cervix with an 8-mm tumor-free vaginal cuff. None of 37 lymph nodes showed metastasis. During follow-up, 8 months after the radical hysterectomy, a small polypoid growth was found in the urethral meatus (Fig. 3). Biopsy of this tumor (Fig. 4A–C) was compatible with the cervical adenocarcinoma. The distal urethra was resected with a tumor-free zone of 3.5 mm. A year after the distal urethrectomy, no evidence of disease was found.

A 2-mm size lesion in the meatus of the urethra is just visible 264×300 mm.
Results
In Case 1 at the 2-year follow-up, no evidence of disease was found. In Case 2, a year after the distal urethrectomy, no evidence of disease was found.
Discussion
When confronted with adenocarcinoma of the vulva, it is important to differentiate between metastasis and primary vulvar adenocarcinoma.
Primary adenocarcinomas of the vulva are rare.2,3 In a series, published in 1973 by Dehner, of 262 primary and secondary vulvar malignancies, only 4 (2%) were primary adenocarcinoma 4 and 22 were metastasis (8%). Of these 22 metastatic vulvar lesions, 73% derived from the genital tract and 18 % derived from the urinary tract. The metastasis originated from the cervix (n=10, 1/10 adenocarcinoma), endometrium (n=4), ovary (n=1), vagina (n=1), urethra (n=2), kidney (n=2) and breast (n=1) and 1 malignant lymphoma.
Primary adenocarcinoma of the vulva can derive from invasive Paget's disease, or from a Bartholin's or vulvar apocrine gland.
Extramammary Paget's disease is an intraepithelial proliferation of atypical cylinder cells. In Paget's disease, the lesions are often multifocal and are slightly raised erythematous-white plaques with sharp edges. 5 The most common complaint is pruritis. These lesions can develop into invasive adenocarcinoma through invasion of the underlying dermis. However, Pagets' disease can also represent an extension of malignant cells from an underlying adenocarcinoma. Approximately 20%–30% of patients with Paget's disease5,6 have another primary carcinoma (colorectal tract cancer [CRC], breast, bladder, urethra, cervix, or ovary) 6 and patients should be screened for this. Adenocarcinoma arising from Paget's disease accounts for <1% of all vulvar cancers.
Malignancies in Bartholin's gland are likewise uncommon,7–9 and adenocarcinoma and squamous cells carcinomas are found in an equal proportion (40%–45 %). Clinically, it is difficult to distinguish malignant disease from a benign Bartholin's gland cyst; therefore, the malignant nature is often only recognized during surgery, or after failure of treatment. 9 Vulvar apocrine adenocarcinoma derives from anogenital glands and can resemble breast cancer histologically, often being positive for estrogen and progesterone receptors. These tumors metastasize to the groin lymph nodes. Therapy is surgical excision and lymph node dissection of the groin.9–11
Metastases in the vulva can derive from the genital tract: endometrial, 12 cervical, 13 and ovarian 14 or may be of extragenital origin: breast,15,16 urogenital, 4 and CRC.17–21 In patients with a known malignancy, new lesions on the vulva should be biopsied to exclude vulvar metastases of the primary tumor. LOH analyses can be used to confirm whether a lesion is a metastasis: similar aberration profiles of two tumors from 1 patient, suggest that one is a metastasis from the other. Different DNA aberration profiles suggest dissimilar primary tumors. 22
In this article, 2 cases with metastatic adenocarcinoma in the vulvar region are described. These 2 cases illustrate that a vulvar metastasis of adenocarcinoma could be the result of a known or unknown primary tumor. It is important to differentiate between primary and metastatic tumors in order not to overlook a potentially curable primary tumor.
In the first case that is described in this article, the vulvar tumor differed clinically from a squamous cell carcinoma, because the lesion had a moist aspect, and was flat and polypoid Histology, including immunohistochemical staining, showed a pattern compatible with CRC. In the literature, several case reports describe perianal and vulvar recurrence after surgery for CRC.18,21,22 The underlying mechanism is thought to be spread of tumor cells via the stapling device in the abraded skin around the anus. Treatment is wide local excision.17–19 Literature review revealed 4 cases of vulvar20,23 metastasis of CRC, not associated with skin abrasion: in two cases the CRC metastasis was localized in the clitoris and in 2 cases in the vulva, and 1 was associated with Crohn's disease. 21
The second patient described here had a metastasis of her adenocarcinoma of the cervix at the vulvar–urethral junction. Although seldom described in the literature, Imachi et al. 13 described that 7 of 1190 (0.6 %) patients with cervical cancer developed vulvar metastases. Two of the 7 patients had adenocarcinoma. Five out of the 7 patients had other distant metastases. Treatment reported was surgical resection followed by radiotherapy in 2 patients, radiotherapy only in 2 patients, and chemotherapy in 1 patient. Two patients did not receive treatment for their vulvar lesion.
One possible explanation for vulvar metastases is the altered lymphatic spread after a pelvic lymph node dissection. 24 It is, however, unlikely that the metastases in case 2 were lymphogenic; all previously removed lymph nodes were negative, and lymph vascular space involvement was not present in the original tumor. A possible explanation for the metastasis on the vulva–urethra junction in this patient could be perioperative damage to the mucosal membrane of the urethra by the bladder catheter, and contamination and subsequent implantation of carcinoma during hysterectomy.
Conclusions
When an adenocarcinoma of the vulva is diagnosed, it is important to differentiate between primary (including lesions linked to apocrine glands, Paget's disease, and adenocarcinoma of Bartholin's gland) and metastatic disease. Biopsies should be taken in a patient with a known malignancy who develops a vulvar lesion to rule out vulvar metastasis. Clinicians should be aware that in a patient in whom adenocarcinoma of the vulva is diagnosed, a urogenital, breast, or colorectal primary tumor might be present.
Footnotes
Disclosure Statement
No competing financial conflicts exist.