
Abstract
Abstract
Introduction
ND, not described; SSI, Surgical site infection; Pre, preoperative; Intra, intraoperative.
Case
A 41-year-old nulliparous female was referred to Yoshida General Hospital with a 9-year history of increasing abdominal girth. In addition, she had become almost totally immobilized for 1 month and could not stand from the supine position because of worsening dyspnea. She was 151 cm tall and weighed 92.6 kg. Physical examination revealed gross abdominal distension and abdominal surface collateral veins. The laboratory data showed that CA-125 was elevated up to 150.3 U/mL. The chest radiograph showed bilateral diaphragmatic elevation and diminished lung fields (Fig. 1). Computed tomography (CT) showed a large, multilocular, cystic tumor that occupied the entire abdomen (Fig. 2). On abdominal and transvaginal ultrasonography (US), the multilocular tumor seemed to be derived from the ovary, and a solid protruding structure was detected in the cyst (Fig. 3). The patient could not be placed in the supine position because of aggravation of dyspnea (Fig. 4). Therefore, she was anesthetized in a reverse Trendelenburg position with a left lateral tilt, to decrease the pressure on the lungs, improve oxygenation, and prevent supine hypotension. On laparotomy, an attempt was made to remove the mass as a whole, to avoid rupture causing malignant cell spillage into the abdominal cavity, but there were too many dense peritoneal adhesions. Intraoperative drainage was then performed over 2 hours to shrink the tumor, while intensely monitoring the patient's vital signs; the total drainage amount was 41 L. Subsequently, tumor removal, hysterectomy, and bilateral salpingo-oophorectomy were performed successfully. The cyst had a diameter of 45 cm and weighed 3.5 kg (Fig. 5). On pathology, a single-layer columnar epithelium with mucin-containing cytoplasm and uniform basally arranged nuclei was seen (Fig. 6). The final pathologic diagnosis of the giant tumor was mucinous cystadenoma. The patient was finally discharged from the hospital 2 months after the surgery without any complications, when she was capable of walking on her own. The rehabilitation period was prolonged because she had been unable to walk for so long. Her body mass index (BMI) on discharge was 19 kg/m2.

Chest radiograph demonstrates bilateral diaphragmatic elevation with diminished lung fields.
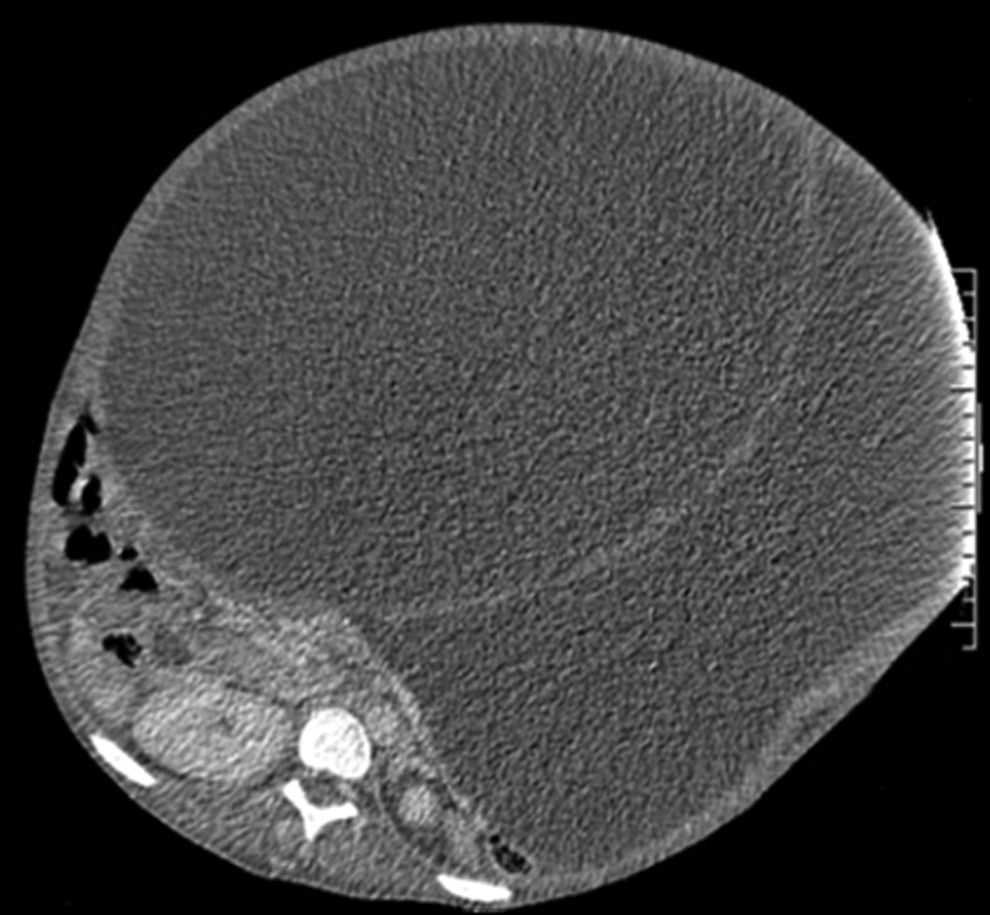
Computed tomography scan shows a huge multilocular cystic mass that occupies the entire peritoneal cavity.
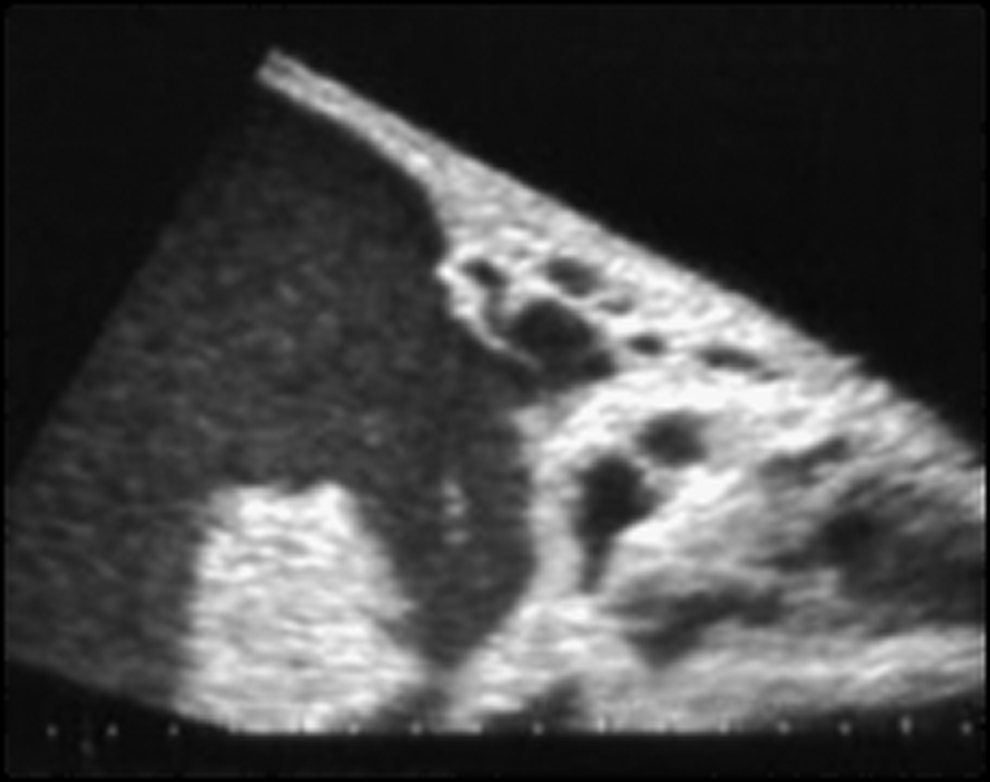
Transabdominal ultrasound shows the tumor with a protruding structure in the cystic wall.

The patient at operation, showing the markedly distended abdomen with greatly dilated subcutaneous veins.

The removed ovarian cyst measured 45 cm in diameter.
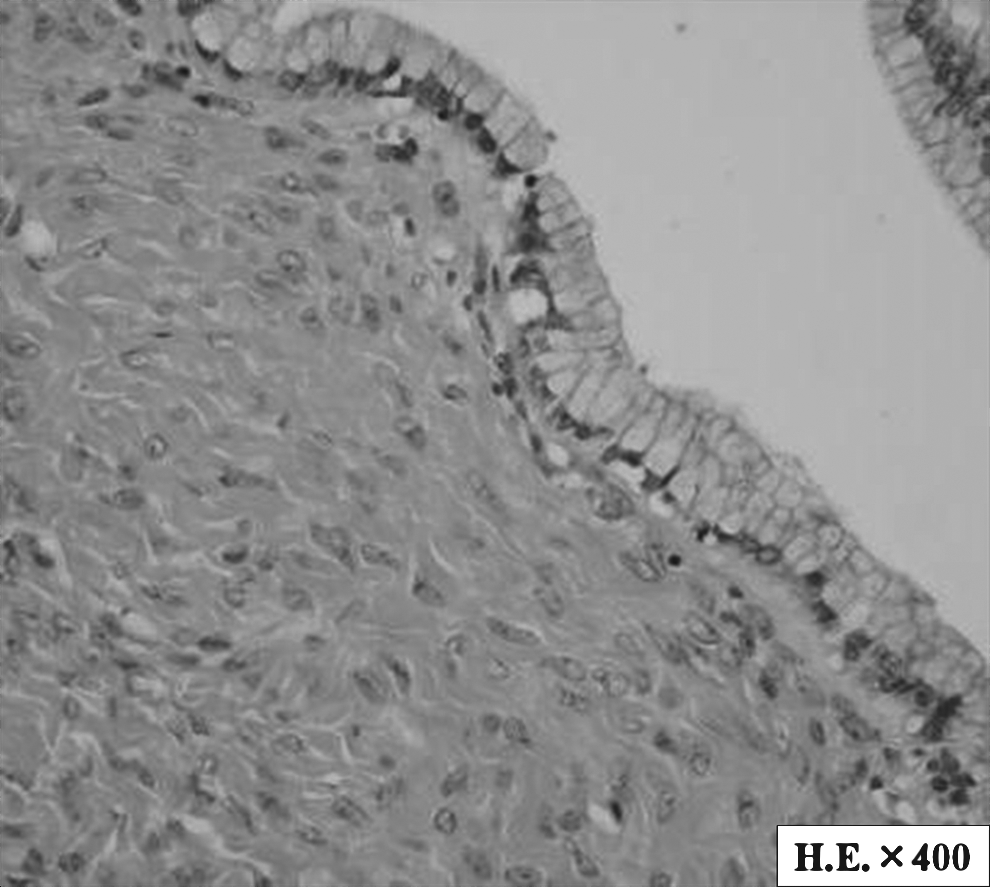
Microscopic pathology of the tumor showing a single layer of columnar epithelium with mucin-containing cytoplasm and uniform, basally arranged nuclei (hematoxylin/eosin).
Discussion
Recent advances in the healthcare system and patient education have decreased the frequency of giant ovarian tumors. Giant ovarian tumors are benign tumors, mainly serous or mucinous cystadenomas, but some cases of low–malignancy-potential tumors and adenocarcinomas have been reported.2–7 The largest ovarian tumor, reported in 1970, weighed 149 kg. 1 There have been 22 resected giant ovarian tumor cases of >40 kg since then (Table 1).2–23 Special attention must be directed to their perioperative management, especially during cyst drainage, to avoid associated complications.
Table 1 shows the details of the reported perioperative management, complications, and clinicopathologic data of patients with giant ovarian tumors weighing>40 kg. The tumor weights ranged from 47 to 134.7 kg, with a mean weight of 71.4 kg. The histopathologic diagnoses were benign tumors in 16 cases (72.7%) and malignant tumors, including low-potential malignant tumors and mucinous cystadenocarcinomas, in 6 cases (27.2%). The highest intraoperative bleeding amount was 18,900 mL, which caused disseminated intravascular coagulation and death. 7 Complications associated with cyst drainage were: massive bleeding in 9 cases (36.3%);4,5,7,10–15 repeat surgery resulting from peritonitis and massive bleeding in 2 cases (9.0%);9,10 re-expansion pulmonary edema, which needed intensive monitoring of respiratory management, in 1 case (4.5%); 9 and pulmonary dysfunction, such as pneumonia and atelectasis, in 2 cases (9%).6,12
The main advantage of drainage is to shrink the cyst to a more manageable size, facilitating subsequent surgery. This makes it safe to perform the operation by widening the working space. Einenkel et al. reviewed the literature about whether and when to perform drainage, and concluded that it was better to avoid drainage, because of the risk of cell spillage that would worsen the prognosis. 8 However, late recurrence caused by disseminated carcinoma cells has not been reported so far. Furthermore, the advantage of preoperative drainage is prevention of pulmonary edema and improvement of the pulmonary and circulatory systems through slow reduction in tumor size. One must be careful when using long-term tube drainage to avoid problems such as infection, peritoneal dissemination, and sudden massive body fluid loss from the drainage hole. High pressure inside the tumor would make it especially difficult to stop the discharge once it begins.
Intraoperative drainage was useful to prevent massive bleeding and cell spillage into the peritoneum in the present case. Dense adhesions, the size of the tumor, and the associated small working space make it difficult to stop bleeding once it starts. Preoperative drainage was performed safely in all cases, but there was concern about the possibility of infection, as well as pulmonary and circulatory dysfunction caused by tube movement, in the present case. The reported complications did not differ depending on whether pre- or intraoperative drainage or their combination was performed. The important point is to ensure the availability of sufficient blood for transfusions in case of bleeding, and to monitor the pulmonary and circulatory systems carefully in the perioperative period.
Various complications associated with drainage have been reported. Re-expansion pulmonary edema has been described in association with cyst drainage.9,11 The patient should be protected against pulmonary edema because of rapid re-expansion of collapsed lungs and fluid shifting during surgery. Pulmonary edema may also occur after removal of the tumor because of the sudden re-expansion of a chronically collapsed lung as a result of compression by the elevated abdomen. Once this occurs, it sometimes requires ventilation.
The safe management of such cases requires a multidisciplinary team approach to manage the many challenges that may occur as a result of potential severe cardiovascular and respiratory complications. 8 The massive tumor makes it difficult to induce general anesthesia, because the enlarged abdomen decreases the lungs and compresses the circulatory system.
Conclusions
In conclusion, there is a lack of evidence on how to manage such giant tumors in the perioperative period. The advantages and disadvantages of pre- or intraoperative cyst drainage need to be acknowledged to help decide whether to perform pre- or intraoperative drainage. Providing intensive care to monitor the pulmonary and circulatory systems is important, because of the enormous effect of the tumor itself, which can result in their dysfunction before and after surgery. In the present case, intraoperative drainage and tumor resection were safely performed without complications.
Footnotes
Disclosure Statement
No competing financial conflicts exist.