
Abstract
Abstract
Introduction
Objectives
Conservative (hormonal) treatment of early stage endometrial cancer has been advocated as an alternative method of treatment in exceptional cases for young women who wish to preserve their fertility. The objectives of this review are (1) to determine the effectiveness and safety of conservative therapy for stage I grade 1 and 2 endometrial cancer, and (2) to formulate a protocol to save fertility in young patients with endometrial cancer.
Materials and Methods
We searched Pubmed for publications from January 1968 to November 2008. Publications included retrospective studies, case reports, multicenter Phase II study, and literature reviews describing conservative treatment for women with type I endometrial cancer. Because of a lack of prospective studies, we collected all data available on the subject. Two investigators abstracted the data. Studies that were not available online were hand searched.
Results
Literature on conservative treatment of endometrial cancer in women who want to preserve fertility is inconclusive with regard to the best treatment modality. There are many case reports, retrospective observational studies, some prospective studies, and many reviews.
Jadoul 1 reported 38 patients being treated with progestogens; Rackow 2 studied 90 patients. Gotlieb, 3 Ramirez, 4 and Boing 20065 have written the most complete and clear reviews. Chiva has used most of this information and completed it with the last available data and described 133 patients. 6
We offer the most recent and complete review of the available literature. Receptor status and methods of therapy were previously not described as clearly as they are in this review. Table 1 shows all case reports and prospective observational studies published from 1986 to the end of 2008.
No., number; pts., patients; Gr., grade; mo, month; MPA, medroxyprogesterone acetate; MA, megestrol acetate; OH-prog, hydroxyprogesterone caproate; NA, norethisterone acetate; DH, dihydrosterone; NE, norethindrone; a, adenocanthoma; LTFU, lost to follow up.
Number of patients
We found 55 studies describing conservative treatment of endometrial cancer. We checked for double registration, and 245 patients remained. The median age of the patients is 30.3 years.
Grading
Two hundred and thirty-two patients with stage I endometrial cancer had grade 1 disease, and 16 patients had grade 2 or more. Grading was unknown for five patients.
Treatment
Patients were treated with medroxyprogesterone acetate (MPA), megestrol acetate (MA), hydroxyprogesterone caproate (OH-prog), norethisterone acetate (NA), dihydrosterone (DH), and norethindrone (NE). Three of 245 patients did not receive any treatment for their disease. Most patients were treated with MPA varying from 5 to 800 mg per day.
The duration of the treatment varied between 1 and 37 months. The mean duration was 7 months. One hundred and ninety-three out of 245 patients responded to therapy.
Histology results for 143 patients were grade 1, five were grade 2, one was grade 3, and 21 were either grade 1 or 2, not specified by the authors.
Receptor status
Progesterone receptor status was only known in 86 of 245 patients. Seventy-seven (90%) were progesterone receptor positive. Nine patients were receptor negative. Receptor status for all other cases was unknown.
Follow-up
The mean follow-up was 47 months. One hundred and twenty-seven pregnancies and 109 living births were described. Six studies did not mention pregnancy rates, and the rest of the studies were incomplete. It was not stated if all patients wished to conceive. Not all of the studies report all pregnancies (including miscarriages).
Three patients died after being treated conservatively: two died of ovarian cancer and one died of liver cirrhosis. A description of the mortality is provided.
Recurrence
Fifty-nine out of 193 patients had recurrent disease after first responding (partially or completely) to the treatment. Recurrence was noted by hysteroscopy and biopsy or mini-curettage.
Of all 59 patients with recurrences after complete or partial response, 45 hysterectomies with bilateral salpingo-oophorectomy were performed. Eleven patients were retreated with progestatives and responded completely to treatment. One study describing three patients did not give any further information about their pathology results.
Of the 45 patients who underwent hysterectomy, no evidence of disease was seen in three patients. Definitive pathology results were not described for 11 patients with recurrence. One patient had hyperplasia with atypical cells. Thirty-three patients were diagnosed with endometrial cancer, as detailed in Table 2.
Details
Mortality
The first death was described by Ota. 7 A patient died after not responding to conservative treatment, choosing abdominal hysterectomy without bilateral salpingo-oophorectomy. She was treated with 600 mg MPA. Twenty months after initial surgery, a site of recurrence was found in one of the ovaries. Surgery was performed where bilateral salpingo-oophorectomy, pelvic lymphadenectomy, and omentectomy was performed. She was treated with chemotherapy. The patient died 71 months after primary treatment with MPA.
The second death is discussed by Ushijima. 8 After 26 weeks, the patient was in complete remission. She was treated with 600 mg MPA and 81 mg aspirin a day. She had three more treatments with MPA for repeated recurrences. Two years after initial MPA treatment, she got peritoneal carcinomatosis and grade 2 endometrioid adenocarcinoma in her ovary. She died 4 months after surgery. It is speculated that it must have been a secondary primary malignancy (endometrial cancer and ovarian cancer) because no signs of endometrial malignancy were found at hysteroscopy 3 months before development of peritoneal lesions.
The third patient died of liver cirrhosis not expected to be due to this treatment, and one patient had progressive disease but showed no evidence of disease after hysterectomy and bilateral salpingo-oophorectomy. 9
Receptor status
Only 18 studies described the receptor status; 37 did not. In the prospective studies of Yang, 10 Minaguchi, 9 and Yamazawa, 11 the receptor status was known. Yang treated six patients with 160 mg MA per day. Four patients showed response, but two had recurrent disease. The two non-responders and the two patients with recurrent disease underwent a hysterectomy and bilateral salpingo-oophorectomy. Histological findings were twice stage IIa, twice stage Ic, and once grade 2 endometrial cancer. All four specimens showed ovarian cancer. Two samples were proven to be a second primary tumor, but the other two were inconclusive.
The two responders were receptor positive, and two other patients were receptor positive: one had recurrence and one failed any response. The two patients with a negative receptor status were a non-responder and a patient with recurrence.
Minaguchi treated 19 patients with 400–600 mg MPA per day for 2–12 months. 9 Seventeen patients were receptor progesterone receptor positive, one negative and one inconclusive. Fifteen patients responded, and five had recurrent disease, all of whom were receptor positive.
Yamazawa included nine patients, all grade 1, with 400 mg MPA, for at least 6 months. 11 All patients showed response—seven complete responses and two partial responses. Progesterone receptor was positive in the complete response group and negative in the specimen of the two patients with partial response. One patient underwent an additional 9-month treatment with chemotherapy after not showing remission after 6 months. Two patients with recurrent disease were treated surgically and both showed grade 1 ovarian cancer.
Side effects therapy
Ushijima et al. treated their patients with 81 mg aspirin in addition to 600 mg MPA per day to avoid thrombo-emobilic complications that can be theoretically expected. 8 No study proves a significant higher chance of thrombo-embolic or cardiovascular problems with varying amounts of progesterone. Only two authors described a side effect of progesterone. Park described a weight gain of 15 kg during treatment with 600 mg MA (2 months), 400 mg MA (1 month), and 320 mg MA (3 months). 12
Complaints of nausea made one patient choose to stop the treatment in Randall's study. 13 This patient was not treated maximally with medication to diminish the emesis.
Discussion
Two hundred and forty-five patients were treated conservatively with progestogens. Mostly they were treated with MPA. The recurrence rate was high: 31% of all 193 patients (partially) responded to the treatment. However, the mortality rate was low—3 out of 245 patients—and no patient died of endometrial cancer.
We conclude that there is still insufficient evidence to compare the conservative treatment of endometrial cancer with the gold standard. At the same time, there is an increasing demand for conservative treatment of many cancers. Patients demand a better quality of life by keeping the possibility of being able to conceive.
The aim of the study was to provide a protocol for gynecologists to treat their patients uniformly and to clarify the conservative treatment of endometrial cancer. In addition, data were collected prospectively to improve the effectiveness and safety of this method further.
The Safety of Noninvasive Staging
Surgical–pathological staging is the gold standard. FIGO staging for endometrial cancer is done by observing myometrial invasion of the endometrium, intra-peritoneal growth, and adnexal metastatis. In our protocol, surgical staging cannot be done, so clinical judgment for staging has to be done as accurately as possible. Tran investigated that more than 50% myometrial invasion is seen in 24% of young patients versus 49% of older patients. 60 Approximately 7% to 10% of the patients with grade 1 endometrial cancer have deep myometrial invasion.61,62 The chance of myometrial invasion is small for patients with grade 1 endometrial cancer.
During the development of our protocol, we considered the fact that a stage Ic has a less favorable prognosis than a stage Ia, and the diagnostic tools to judge the myometrial invasion are limited. The most accurate way of imaging the myometrial invasion is by (contrast-enhanced) magnetic resonance imaging. The accuracy varies between 68% and 82%. 63 Contrast MRI is the only possibility to approach the accuracy of surgical staging. However, because the accuracy varies between 68% and 82% and there is only a small chance of deep myometrial invasion in low-grade tumors of 7% to 19%, we decided to include all assumed stage I tumors and not leave out stage Ic.60–62
The essence of performing a pretreatment laparoscopy can be discussed. Twenty-two studies described recurrences, and 29 stated that no recurrences were noticed at follow-up. Four studies did not mention recurrences. In the first group, only one study described performing a laparoscopy. In the second group without recurrences, laparoscopy had been performed in 10 out of 29 studies, and one study described pretreatment staging by laparotomy. No patients were excluded from treatment because of laparoscopic findings. We could suggest laparoscopy has been performed more often during fertility analyses before discovering endometrial cancer. However, it has not been recorded. In conclusion, from this review, we cannot conclude whether a laparoscopy is necessary. However, if lesions are suspected by vaginal ultrasound or MRI, laparoscopy is mandatory.
Grading
Endometrioid adenocarcinoma is the most common histological type of endometrial cancer in young patients. Other histological types are papillary serous and clear cell carcinoma. These are high-grade tumors and are not included in our protocol. Transitional cell, squamous cell, mucinous, and small cell cancers account for fewer than 2% of all endometrial cancers and are also excluded.
Receptor status
Positive ER and PR receptor status is of great importance to the response to progesterone. Type I tumors are typically low-grade endometrioid carcinomas, with positive estrogen (ER) and progesterone receptors (PR) in 92% of cases. A dose–response study of the Gynecologic Oncology Group showed a response rate of 37% in PR receptor positive patients and 8% in PR receptor negative patients. Likewise, ER receptor positive patients had a 26% response rate and only 7% for ER receptor negative patients. 64
Ovarian cancer
Ulbright writes that simultaneous presence of an ovarian tumor with the same histology is present in 8% of endometrial cancers. 65 The risk of synchronous primary ovarian cancer is approximately 5% for intrauterine disease. 66 The ovarian tumor should be considered as metastatic when it is small, bilateral, or multinodular with surface implants and angiolymphatic invasion in the ovarian cortex. 65
Hereditary predisposition
Endometrial cancer originates in high endogenous or exogenous estrogen levels or genetic predisposition like type II Lynch syndrome. Type I is estrogen dependent, hormone sensitive, and low stage with a very good prognosis, and type II, the minority, is associated with endometrial atrophy, being high grade, and having a high rate of recurrence. 67 Lynch II syndrome is an autosomal-dominant inherited cancer susceptibility mainly associated with colorectal cancer or endometrial cancer. 68 Patients have a risk of approximately 20% of developing endometrial cancer before the age of 50. 69 The lifetime risk of getting ovarian cancer for this group is more than 12%. 70 Women diagnosed with endometrial cancer at a fertile age should be referred to a genetic counselor.
Biological factors
Exposure to either endogenous or exogenous excess of estrogens instigates an increased risk of developing endometrial carcinoma. Among the risk factors are obesity, early menarche, late menopause, no pregnancies, and genetic disorders. The literature suggests that endometrial carcinoma in young women is less aggressive and biologically different from that of older women.4,5,7 The fact that obese women have a higher chance of a miscarriage is of secondary value and can be considered for inclusion in the counseling but will not be part of the standard work up.
Therapy
Most studies used MPA as their treatment. Eighteen of these studies used a low dose of ≤200 mg, 11 studies about 400 mg, and 7 studies a high dose of 600 mg or more. A study comparing the effects of MPA, NE, and norethynodrel on the endometrium showed a more intense response to progestin than to NE and norethynodrel. 71 MPA is free of estrogen action. Studies in recurrent endometrial cancer have shown 200 mg of MPA to be superior to the higher dose of 1,000 mg per day. It is less toxic and equally effective. 72 There is a 5–17% chance of thrombophlebitis while using MPA.73,74 A higher dose leads to an increased chance of adverse effects. Considering these arguments, we have proposed the use of 200 mg per day for our protocol.
Fertility
Before starting the conservative treatment, normal work up for endometrial cancer should be performed, including contrast enhanced MRI. Most patients start conservative treatment because of a wish for offspring. For this reason, fertility analysis of the patient and her partner (if applicable) should be performed before starting the protocol.
Outcome
Three out of 245 patients died during the mean follow-up of 47 months: two died of ovarian cancer and one died of liver cirrhosis. No patient died of endometrial cancer. The low mortality rate might be because when patients are treated conservatively, the follow-up is strict and the possibility of switching to surgery is always available. Most patients showing recurrent disease were treated surgically. While looking at the results, the influence of publication bias should always be considered. We are supported in this idea, while looking at the data we can see a recurrence rate of 31% compared to 47% is the article of Ushijima and 40.9% in a more recent study by Hahn.8,75
Conclusions
From the results of our literature review, we can conclude that for a selected group of patients, following clear guidelines and protocols, conservative treatment with progesterone is a save method to treat endometrial cancer. Using the information we extracted from the literature, we propose the following protocol.
The inclusion criteria are patients with stage I grade 1 and 2 endometrial cancer, under the age of 40 years, progesterone receptor positive, wishing for offspring, and whose informed consent has been obtained for the treatment advice of total hysterectomy including bilateral salpingo-oophorectomy. The exclusion criteria are patients with recurrent endometrial cancer, endometrial cancer more than stage one and/or grade two, and high-risk cell types.
Patients are treated with 200 mg MPA per day for at least 6 months and more more than 12 months. The minimum duration of treatment is a 3-month-long treatment course and a 3-month-long consolidation course. Three monthly check-ups with hysteroscopy and endometrial sampling are performed to investigate the effectiveness. If a suspicious lesion is seen, it is resected. In cases of irregular bleeding, a hysteroscopy will be performed directly.
After two negative endometrial samplings, conception may be pursued.
Follow-up starts after two negative endometrial samplings. During a period of 5 years, a hysteroscopy with endometrial sampling will be performed every 6 months. After this period, check-ups are done yearly.
Factors that must be reported in future case reports are: receptor status, drug use, body mass index, attempts for pregnancies, fertility problems, follow-up, and histology results.
Treatment is stopped if (1) histology results show endometrial cancer after three cycles of 3 months of therapy; (2) one of the samplings shows endometrial cancer grade 3; or (3) imaging shows extrauterine disease.
If a patient is excluded from the protocol, she receives a total hysterectomy including bilateral salpingo-oophorectomy. The protocol is shown in Figure 1.
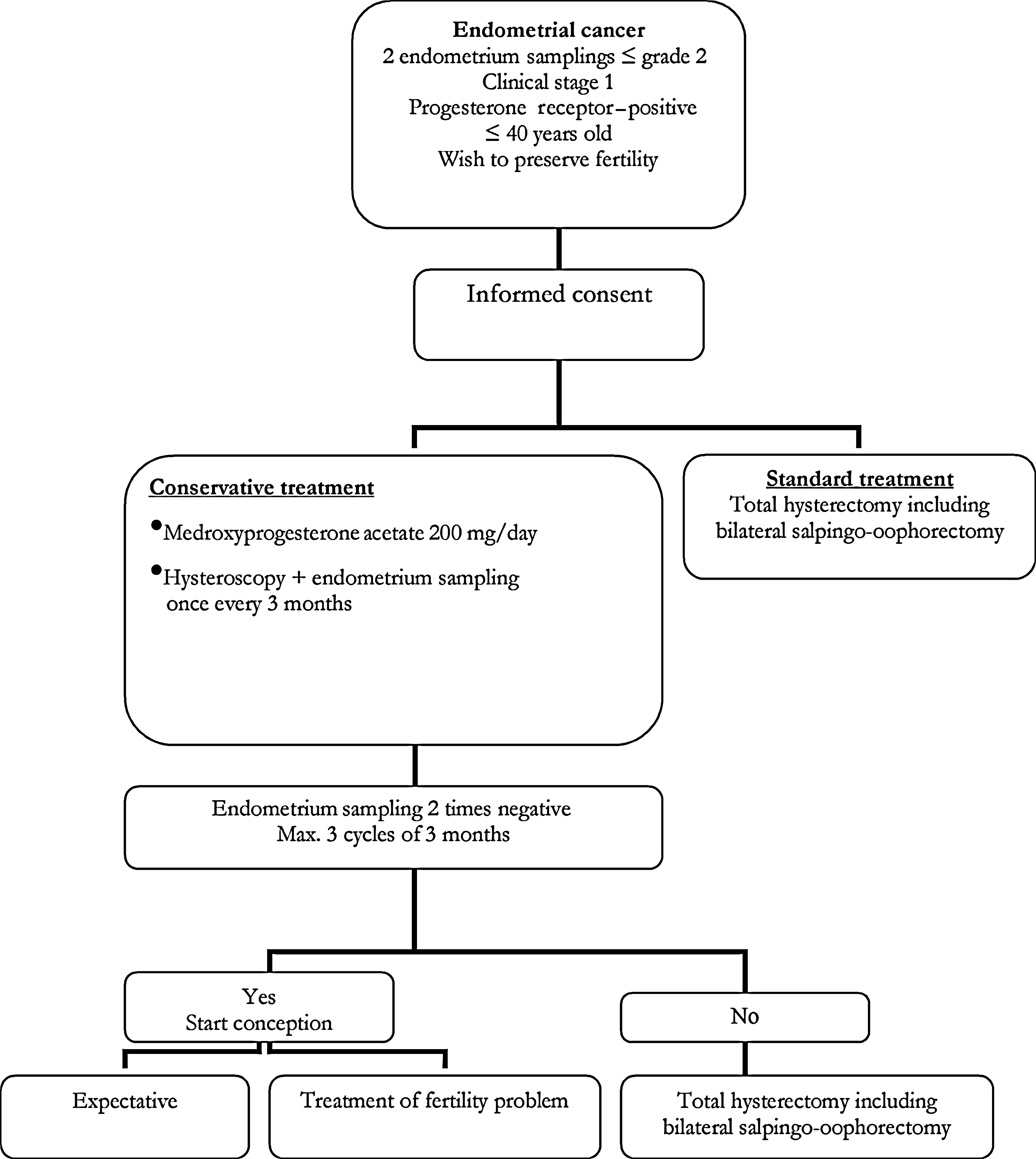
Flow chart showing conservative treatment of endometrial cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.