
Abstract
Abstract
Introduction
Unsafe abortion is defined as the termination of an unintended pregnancy either by persons lacking the necessary skills or in an environment lacking the minimal medical standards, or both. 3 Recent reports support an increasing trend in unsafe abortion without concomitant public policy to reverse it.4, 5
Abortion-related complications and death are usually preventable, but in an environment where restrictive abortion laws exist, overt complications such as uterine perforation with hemorrhage, bowel injury with gangrene, and tetanus infection are common place because of individuals who procure unsafe abortion in clandestine environments. 6
An unusual presentation of ileojejunal prolapse through the cervix via a laceration in the uterine fundus following unsafe abortion by an unskilled attendant, and the resultant extensive bowel surgery performed, is reported.
Case
A 22-year-old married para 1+1 (1 alive) was admitted via the accident and emergency unit with protrusion of bowel per vagina and generalized abdominal pain, 10 hours following an abortion with sharp metallic objects, that took place in a nonmedical facility. She had bled profusely and had experienced dizziness but no fainting attack. The abortion was procured at an estimated gestational age of 12 weeks; 6 weeks after confirmation with a urine pregnancy test. The patient's last pregnancy was 2 years previously.
On examination, the patient was found to be anxious, sweating, and markedly pale. Pulse rate was 120 beats per minute and blood pressure was 80/40 mm Hg. There was generalized abdominal tenderness with guarding. Pelvic examination revealed a blood- stained foul-smelling vulva with ∼1.5 m of gangrenous ileum protruding per vagina with no active bleeding (Figs. 1 and 2). Her cervix was 2 cm dilated with traumatized edges. The vagina was normal. A diagnosis of uterine perforation with bowel injury following unsafe abortion was made. Hemoglobin concentration was 5 g/dL; electrolytes were within normal limits. The patient was resuscitated with intravenous fluids and antibiotics; had 3 units of whole blood transfused, and received tetanus prophylaxis. She underwent an emergency exploratory laparotomy.
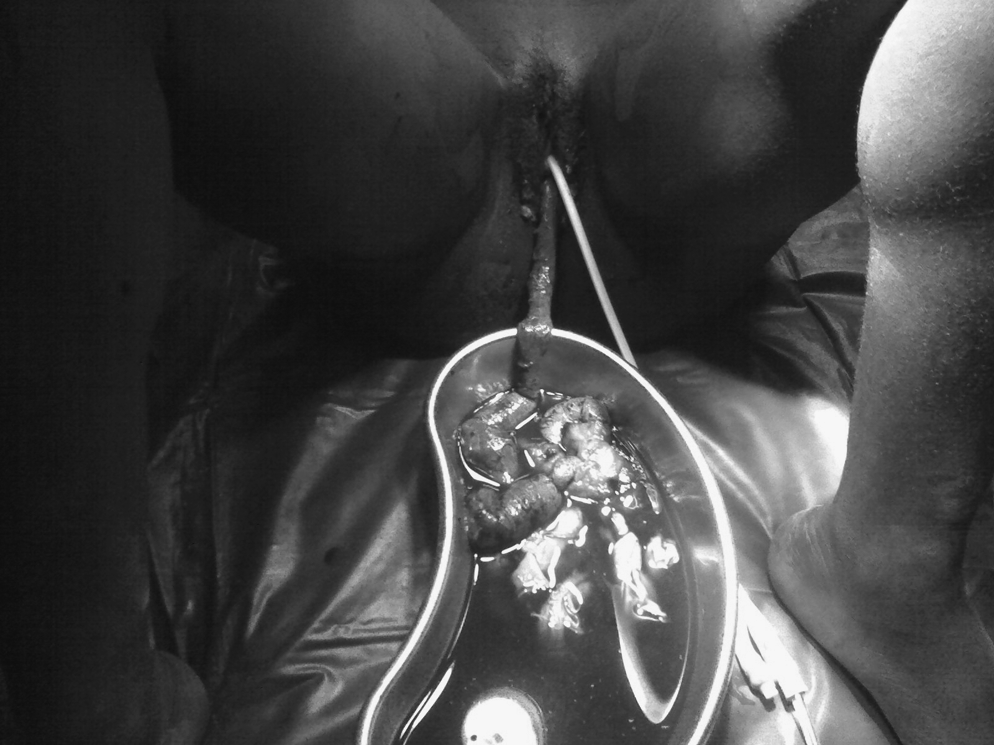
On presentation, first view of bowel prolapse.

On presentation, second view of bowel prolapse.
At surgery, there was hemoperitoneum of 1.5 L; 14-week size uterus with transverse ragged laceration of the fundus bleeding actively; 1.5 m of gangrenous ileum protruding through the cervix via the uterine laceration; ragged edges of the remaining ileum up to 4 cm from the ileocecal junction; edematous distal jejunum with bleeding points ∼16 cm in length; grossly normal ovaries, tubes, appendix and large bowel; and no retained product of conception (Figs. 1–3). She had uterine repair, jejunal resection (distal 16 cm), total ileal resection, right hemicolectomy, and colonojejunal anastomosis. She was continued on antibiotics.

Close-up view of fundal injury.
She was discharged on the 10th postoperative day after counseling on contraception and hospital delivery, and parenteral vitamin B12 supplement. She was seen after 5 weeks with no complaint.
Discussion
This case highlights the problem with unsafe abortion in Africa. Abortion is legally prohibited in this country and carries religious and social stigma. 7 This gives rise to its being performed in secret by untrained personnel in poorly equipped facilities, with attendant complications. Factors associated with high rates of abortion mortality and morbidity in developing countries include inadequate access to contraception, restrictive abortion laws, pervading negative attitudes to abortion, and poor health infrastructures. 8
In their review of 9 cases of bowel prolapse following uterine perforation seen in Sokoto, Ntia and Ekele 9 found that the ileum was involved in 67% of the cases whereas the uterine injury was on the fundus 78% of the time, which is similar to what was found in this case. Unlike in the cases reviewed, this patient presented within 10 hours of instrumentation and recovered with no anastomotic leakage. 9
In the case under review, the activity of the abortionist resulted in a drain on the lean purse of the patient and her family in terms of the cost of medical care, surgery, and hospital stay; and caused a preventable strain on the hospital facilities and surgeon. The case brings to the fore the need for contraception and effective public policy to address the issue of unsafe abortion.
Fortunately for this patient, she presented early at a tertiary institution where the complications were managed successfully. This is not always the case. 9 Poverty, coupled with fear of legal recriminations, prevents those with complications from seeking professional help on time. 10 Nevertheless; the surgery performed in this case disrupted the enterohepatic circulation, vitamin B12 absorption, and water reabsorption in the gut. This predisposed the patient to megaloblastic anemia and diarrhea.
Conclusions
The issue of abortion remains a delicate one in Nigeria, presenting a complex of moral and ethical dilemmas. In all societies, however, no matter what the legal, moral, or cultural status of abortion is, there are women who will seek to terminate an unwanted pregnancy. 9 This abortion with bowel injury highlights the persisting problem of unsafe abortions in Nigeria. Bowel injury is a serious and life-threatening complication in a case such as this, although occurring in this patient in an unusual presentation.
More health education, improvement of healthcare services, and changes in the restrictive abortion laws have to occur to reduce the incidence of unsafe abortion and its attendant morbidity and mortality.
Footnotes
Disclosure Statement
No competing financial conflicts exist.