
Abstract
Abstract
Introduction
The immediate endocrine responses to LOD are similar to those previously described after wedge resection, indicating that the effects are similar 3 After LOD, the main hormonal changes reported in many studies include a rapid and persistent fall of androgens (testosterone and androstenedione) with a transient increase of gonadotropins (luteinizing hormone [LH] and follicle-stimulating hormone [FSH]) during the first 24–48 hours, followed later by a gradual fall in levels of these hormones.4–6
Although the short-term endocrine effects of LOD have been extensively investigated, it is still uncertain how long these effects last. Some investigators have reported that the endocrine effects of LOD are rather transient,7,8 whereas other researchers have indicated that the treatment might have long-term beneficial effects.9,10 In a long-term follow-up study, Gjonnaess reported on the late endocrine effects of LOD in 51 women. 2 He concluded that ovarian electrocautery in women with PCOS normalizes serum levels of androgens and LH and that the results appear to be sustained for 18–20 years.
Recently, there has been a tendency to use finer laparoscopic instruments, which are more suitable for office procedures under local anesthesia, instead of general anesthesia. Introduction of this new technology has been limited, because of the the narrow-scope view of the finer laparoscopic instruments. A newer highly advanced microendscope using the new fiberoptic technology has solved this great problem, offering a laparoscopic view that is nearly similar to the traditional 10-mm telescope. This new updated 2-mm telescope has been recently used for many gynecologic procedures that were previously performed using the older traditional telescope. 11
In this study, observations of the medium- and long-term endocrine and ovarian changes in women who underwent office microlaparoscopic ovarian drilling (OMLOD) under augmented local anesthesia for PCOS are reported and observations are compared with a group of women with the same condition, but without surgical intervention (comparison group). Factors that affected the results at long-term follow-up are also examined.
Materials and Methods
Subjects
Between 2006 and 2010, a total of 194 women with anovulatory infertility associated with PCOS underwent OMLOD at El-Minya University Hospital in El-Minya, Egypt. The hospital records of these 194 subjects were reviewed. Afterward, a letter was sent to the patients to ask if they were willing to participate in the follow-up study.
Twenty-eight subjects were lost to follow-up, 20 declined to participate, and 30 were unable to provide reliable follow-up data because they had been receiving long-term hormone treatment, including the combined oral contraceptive pill, or had had hysterectomies (n=8). The remaining 116 patients provided the data for our study. All the women had anovulatory infertility of >1 year's duration and had been treated unsuccessfully with CC at up to 150 mg/day for 5 days in the early follicular phase of the menstrual cycle prior to LOD.
In 104 women, CC failed to induce ovulation (CC resistance). The remaining 12 patients ovulated, but failed to conceive after CC treatment for 6–9 months. In addition, 7 women had received human menopausal gonadotropin (hMG) therapy for ovulation induction and failed to conceive. Most of the women (n=96) attended a follow-up interview with one of the investigators, at which time, a blood sample for serum hormonal concentrations and a transvaginal scan were performed.
Comparison group
A total of 34 women with anovulatory infertility associated with PCOS who were diagnosed during the same time period of the study but had not undergone OMLOD were identified from the same hospital. These women comprised the comparison group.
All the women had anovulatory infertility of >1 year's duration. Two subjects decided to postpone fertility treatment after their initial diagnosis, and the remaining 32 women received CC. Twenty-eight of these subjects had interviews, blood tests for serum hormonal concentrations, and transvaginal scans.
PCOS
The diagnosis of PCOS in both groups of women was based on the Rotterdam criteria as follows:
1. Evidence of hyperandrogenism, early follicular phase (defined as days 2–5 of the menstrual cycle) serum LH:FSH ratio >2 and/or raised serum androgen concentrations (testosterone 2.5 nmol/L, androstenedione 10 nmol/L or free androgen index [FAI] >4).12,13 FAI was calculated using the formula: testosterone 100/sex hormone-binding globulin (SHBG).14,15 2. Evidence of an- or hypo-ovulation, or 3. Ultrasonographic evidence of polycystic ovaries (PCO): ovarian stromal hypertrophy and multiple small (6–8 mm) follicles arranged in the periphery.
16
OMLOD
The microlaparoscopic system consists of a light source, a high-speed pneumoperitoneum device, and a 1 CCD video camera. The diameter of the scope was 2.2 mm, and the grasping forceps, scissors, needle probes, biopsy forceps, and irrigator-aspirator were also 2.2 mm in diameter (all equipment made by Olympus, Tokyo, Japan). The instruments can be used by specially designed trocar (access needle; Ethicon, Cincinnati, OH), a 12-cm long and 2.5-mm-diameter metal sleeve that fits over the Veress needle. Premedication consisting of 0.5 mg of atropine sulfate and 1 mg/kg of midazolam was given I.M. One mg/kg of fentanyl followed by 1.5 mg/kg of ketamine was administered i.v. through a drip infusion line.
The patient was placed in a lithotomy position. An Access Needle (Ethicon, Tokyo, Japan) was inserted through a small incision created in the subumbilical region using the closed method, after having been locally infiltrated with Xylocaine (lidocaine) local anaesthesia. Pneumoperitoneum was induced with carbon dioxide gas. Other Access Needles were then inserted into both sides of the hypogastric region under microlaparoscopy. Four mL per port of 0.25% bupivacaine were locally injected at the trocar insertion sites in advance. All the scopes and forceps used were from the microlaparoscopy set of 2.2 mm in outer diameter (Olympus, Tokyo, Japan), while the ovarian ligament was grasped with holding forceps to fix it in place.
The ovaries were observed under the microlaparoscope. During the microlaparoscopy procedure, the size of the ovary was measured using Maryland forceps. When the forceps are extended, the distance between the two arms is 1.4 cm and this distance was used to measure the length, width, and depth of each ovary. A high-frequency 2.2-m electrocautery probe was used for ovarian drilling. The number of ovarian punctures differs according to the size and the total surface area of the ovary. A number of ranges, from 5 to 10 punctures, have been used for ovarian drilling. The electrocautery probe is provided with a cool-water irrigation channel, to cool the drilled ovary rapidly.
Ultrasound scanning
Patients underwent transvaginal scanning prior to OMLOD (n=101) and at medium- (1–3 years, n=36) and long-term (4–9 years, n=67) intervals after surgery. Two ultrasound machines of the same model (Toshiba, model Sonolayer SSA-250A, with a convex 6-MHz transvaginal ultrasound probe) have been used in the unit during the 9-year follow-up period.
At medium- and long-term follow-up, women with regular menstrual cycles were scanned on days 2–5 of the cycle, whereas women with severe oligomenorrhea were not timed according to the menstrual cycle. Each ovary was localized in relation to the iliac vessels, and scanned from inner to outer margins in longitudinal cross-sections and from upper to lower ends in transverse cross-sections.
The three diameters of each ovary were measured (longitudinal, anteroposterior, and transverse). The ovarian volume was calculated using the formula of a prolate ellipsoid: 0.523 length width thickness, according to the method of Sample et al. 17 The mean volume of the right and left ovary was calculated for each subject.
Collection of blood samples
Blood samples were taken from women in both groups early in the follicular phase (defined as days 2–5 of the menstrual cycle) or at a random time in women with severe oligomenorrhoea or amenorrhoea. The samples were collected from the patients prior to LOD and at different intervals following surgery: short- (<1 year); medium- (1–3 years); and long-term (4–9 years).
Hormonal assays
Serum hormonal concentrations were measured using well-established assays, which have been validated in the laboratory at the Department of Clinical Chemistry of El-Minya University Hospital. These assays, which have previously been described,18,19 were not changed between 1991 and 2000; that is, the same assays were used at the different periods of follow-up.
Follow-up data
The endocrinologic and ultrasonographic data were documented before and at different intervals (short-, medium- and long-term) after OMLOD. The age of the patients when the diagnosis of the condition was made, and other demographic details, including body mass index (BMI), whether infertility was primary or secondary, and duration of infertility, were also documented.
Statistical analysis
For statistical analysis, the data were entered into the Statistical Package for Social Sciences (SPSS) for PC, version 10.0.5. Continuous data were compared by Mann–Whitney U test and Wilcoxon signed-ranks test. Comparisons of categorical data were performed using 2×2 contingency table analyses. Significance was assumed if p<0.05.
Ethical considerations
The local university ethical committee had approved the study before its formal start.
Results
A total of 116 patients was included in this part of the study.* The demographic, clinical, and endocrinologic characteristics of this group of subjects are shown in Table 1. The characteristics of the comparison subjects are also shown in the same table.
Menstrual patterns definitions: regular cycles, cycle length between 25 and 35 days; oligomenorrhoea, cycle length between 35 days and 6 months; amenorrhoea, absence of the menstrual period for >6 months. polycystic ovaries.
PCOS, polycystic ovary syndrome; OMLOD; office microlaparoscopic ovarian drilling; LH, leuteinizing hormone; FSH; follicle-stimulating hormone; FAI, free androgen index; PCO, polycystic ovaries; hMG, human menopausal gonadotropin; SD, standard deviation.
LH concentrations
The serum concentrations of LH and the LH:FSH ratio decreased significantly after LOD and remained low during the medium- and long-term follow-up (Fig. 1). In contrast, the serum LH concentrations and the LH:FSH ratio of women in the comparison group did not show significant changes during the same time periods.
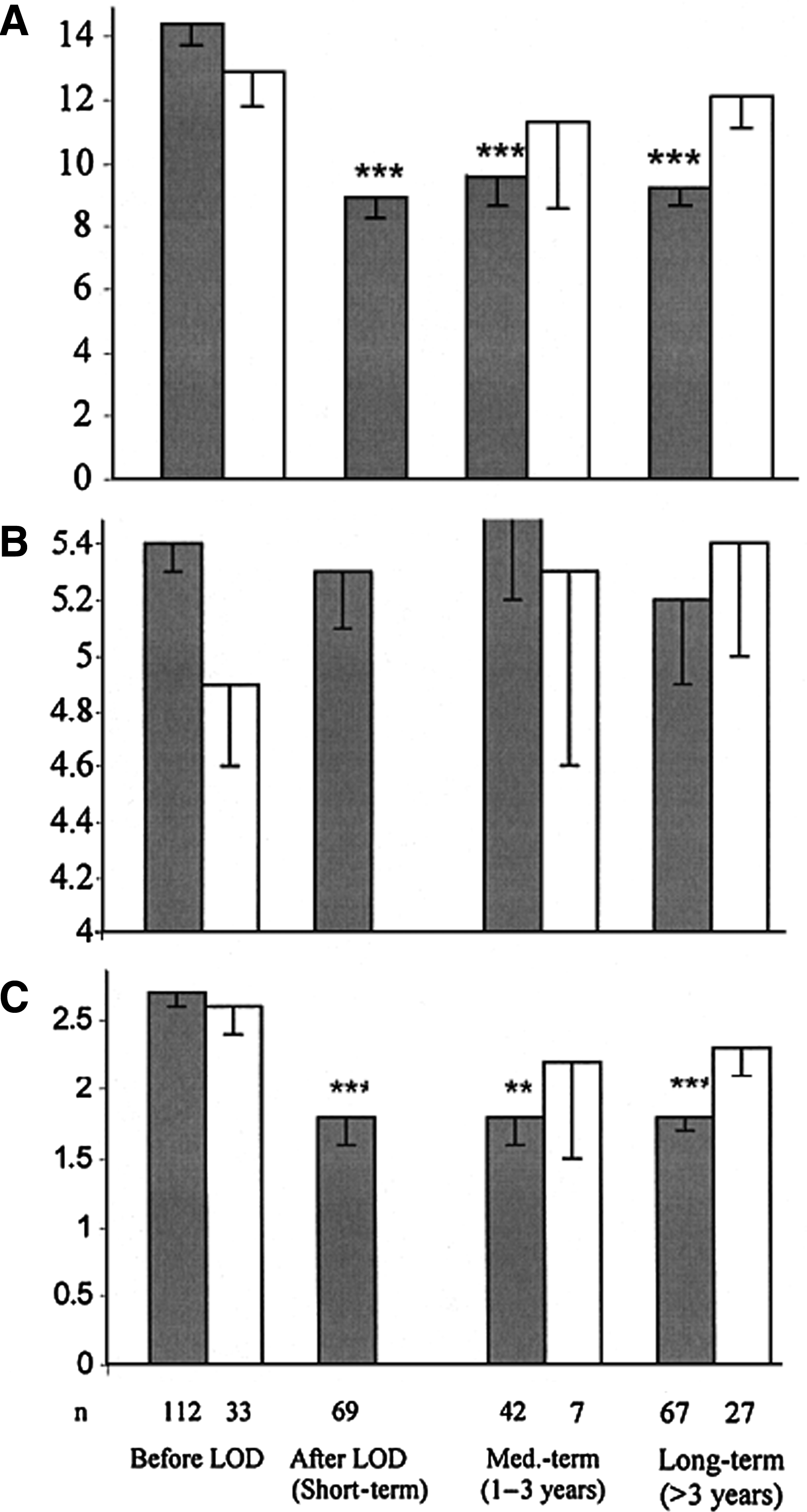
Serum luteinizing hormone (LH) and follicle-stimulating hormone (FSH) concentrations and LH:FSH ratio in women with polycystic ovary syndrome before treatment and during the three periods of follow-up. Data show mean values—1 standard error of the mean. The gray bars represent women who underwent office microlaparoscopic ovarian drilling (OMLOD) under augmented local anesthesia, whereas the white bars represent women who did not (comparison group). The Mann–Whitney test was used to compare the two groups. (
Comparison of the proportion of women with high LH concentrations (>10 international units [IU]/L) before and after OMLOD showed a significant (p<0.01) decrease from 70% prior to LOD to 33% shortly after surgery. The proportion remained low during the medium- and long-term follow-up periods (45 and 31%, respectively). In contrast, the proportion of women in the comparison group with LH concentrations >10 IU/L (67%) did not show significant changes during the same follow-up periods (57%–67%).
FSH concentrations
There was no significant change in the serum concentrations of FSH after OMLOD in either group (Fig. 1B). The mean serum FSH concentrations remained ∼5 IU/L throughout the follow-up periods after OMLOD. At long-term follow-up, the FSH levels ranged between 1.1 and 13.5 IU/L. Up to 9 years after surgery, there was no case of premature ovarian failure (POF) among women who underwent OMLOD.
Androgen concentrations
In Figure 2, the serum concentrations of testosterone, androstenedione and SHBG, and the FAI before OMLOD and at the three periods of follow-up are shown. The mean serum testosterone concentration and FAI decreased significantly after OMLOD and remained low throughout the follow-up periods. The mean serum concentration of androstenedione showed no significant change shortly after OMLOD, but showed a significant reduction at medium- and long-term follow-up.

Serum androgen concentrations in women with polycystic ovary syndrome (PCOS) before treatment and during the three periods of follow-up. Data show mean values and −1 standard deviation. The gray bars represent women who underwent office microlaparoscopic ovarian drilling (OMLOD) under augmented local anesthesia, whereas the white bars represent women who did not (comparison group). The Mann–Whitney test was used to compare the two groups before treatment and at long-term follow-up. Before treatment, not significant; long-term, p<0.01 to <0.001 (except sex hormone-binding globulin [SHBG], not significant). The results at the three periods of follow-up after OMLOD were compared with the preoperative values (Wilcoxon signed-ranks test used). NS, not significant; *p<0.05; **p<0.01:***p<0.001.
The number of subjects in the comparison group who had their androgen levels measured at medium-term follow-up was too small for it to be possible to make direct comparison between the two groups. The serum testosterone concentrations and FAI of women who had not undergone OMLOD did not show significant change at long-term follow-up (Fig. 2).
However, the mean serum androstenedione concentration of the comparison group decreased significantly (p<0.05) at that time. The percentage of women with FAI 4 showed a significant (p<0.01) decrease from 69% prior to OMLOD to 41% shortly after surgery. The value remained low (33%–35%) during the medium- and long-term follow-up periods.
Ultrasound findings
ln Figure 3A, the proportion of women with ultrasound evidence of PCO prior to treatment and at medium- and long-term follow-up, are shown. The results show that the proportion of women with ultrasound evidence of PCO significantly (p<0.01) decreased after OMLOD and remained low during the follow-up periods. By contrast, no similar changes were observed in the comparison group during the corresponding follow-up periods.
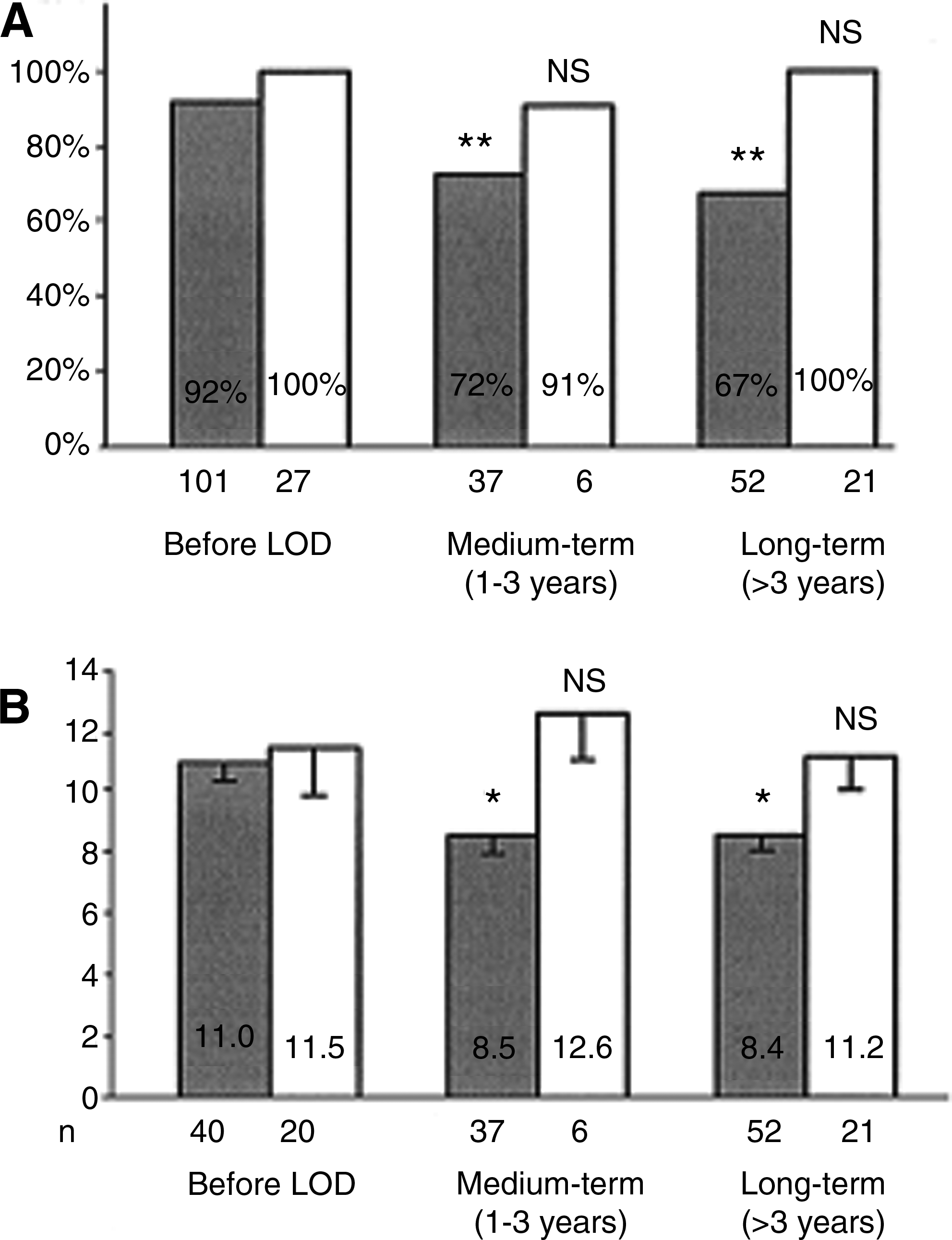
Ovarian changes in women with polycystic ovary syndrome before treatment and during the three periods of follow-up. The gray bars represent women who underwent office microlaparoscopic ovarian drilling (OMLOD) under augmented local anesthesia, whereas the white bars represent women who did not (comparison group). (
Figure 3B shows the mean ovarian volume for both groups of women before treatment and at medium- and long-term follow-up. The mean ovarian volume decreased significantly (p<0.05) at medium-term follow-up after OMLOD and the effect was sustained for up to 9 years. However, the ovarian volume in the comparison group did not show significant changes during the same periods of follow-up.
Factors affecting the endocrinological outcome
The possible impact of age and BMl on the results of the follow-up was analyzed. However, the mean serum concentrations of testosterone (1.7 nmol/L) and androstenedione (6.5 nmol/L) in women with BMI >25 kg/m2 were significantly (p<0.05) higher than those of women with BMI 25 kg/m2 (1.2 and 4.9 nmol/L).
Discussion
In this study, the long-term endocrine and ultrasound changes in 116 anovulatory women with PCOS after OMLOD and a comparison group of women with the same condition, who had not undergone OMLOD, were observed.
LH
Age at the time of follow-up had a significant impact on the serum concentrations of LH after OMLOD. Women 36 years old had significantly (p<0.01) lower levels of LH (7.5 IU/L) than those (10.4 IU/L) of younger (35 years) women. In contrast, BMI at the time of long-term follow-up did not appear to have any significant impact on the serum LH concentrations, compared to the control group (13±6.2 IU/L). In women with a BMI>25 kg/m2, the mean serum concentration of LH was 9.5 IU/L, which was not significantly different from that of women with a BMI 25 kg/m2 (8.9 IU/L).
FSH
Age at the time of long-term follow-up did not have a significant impact on the serum concentrations of FSH. Fourteen patients were ages 39–45, and their FSH concentrations ranged between 2.4 and 8.1 IU/L with a mean value of 4.9, compared with the control group (FSH=5±1.6 IU/L).
Androgens
As far as androgen levels are concerned, age did not have a significant impact on FAI and serum concentrations of testosterone and androstenedione at the time of long-term follow-up. The current authors confirm previously reported endocrine changes shortly after OMLOD, including lowering of the LH:FSH ratio and the serum concentrations of LH and androgens.3–5,6,9,20–25
These endocrine changes seemed to last during the medium- and long-term follow-up periods (up to 5 years). This observation is comparable with an earlier report by Gjonnaess who demonstrated that the endocrine changes after LOD were stable for 18–20 years. 2
Naether et al. also showed that serum testosterone concentrations decreased after LOD and remained low for up to 6 years. 10 However, the current authors confirmed in this study that these long-term endocrine changes are produced by ovarian drilling rather than the effect of advancing age, because the serum concentrations of LH and androgens in women who underwent OMLOD were significantly lower than those of the comparison group at corresponding periods of follow-up.
The proportion of women with high LH concentrations (>10 IU/L) decreased significantly from 70% to 33% shortly after OMLOD but increased back to 45% during the medium- term follow-up (1–3 years). This latter increase, although statistically insignificant, shows a trend toward an increase in serum LH concentrations >1 year after surgery.
One may therefore speculate that the effect of OMLOD faded in a proportion of women (∼15%) 1 year after surgery. At long- term follow-up, the proportion of women with high LH concentrations decreased to a level (31%) seen at short-term follow-up after OMLOD. This latter decrease may be explained by a phenomenon related to the natural history of the disease, in that the clinical and endocrine features of PCOS become less pronounced with advancing age.26,27
This is supported further by the observation that older women (>36 years of age) at the time of long-term follow-up had significantly lower serum LH concentrations than did younger (<36 years of age) subjects. However, it appears that ovarian drilling had contributed to the long-term changes of serum LH concentrations, as the proportion of women with LH >10 IU/L at long-term follow-up after surgery was significantly lower than that of the comparison group during the corresponding follow-up period. A trend toward a reduction in the proportion of women with high serum concentrations of LH at long-term follow-up was not observed in the comparison group, possibly because of the small number of women included in that group.
There was a trend toward a decrease of serum androgen levels with the increasing number of years after LOD, possibly because of the effect of advancing age (Fig. 2). A similar trend toward a decrease of androgen levels was also observed in the comparison group; in particular, the significant reduction of serum androstenedione concentrations at long-term follow-up. The impact of advancing age on serum concentrations of androgens was not observed, possibly because of the effect of an increasing BMI with age, which is associated with an increase in androgen levels.
In the current cohort of patients, there were no cases of POF up to 5 years after OMLOD. At long-term follow-up, 14 women were ages 39–45 years and their FSH concentrations ranged between 2.4 and 8.1 IU/L. It can therefore be concluded that using the techniques described in this study is safe and is not associated with an increased risk of premature menopause.
Ultrasound changes
In this study, the long-term impact of ovarian drilling on sonographic features of the ovaries is reported for the first time. Ovarian drilling resulted in a significant reduction in ovarian volume, and the effect was sustained throughout the follow-up periods. In one study, Tulandi et al. reported on the short-term effect of ovarian drilling on ovarian volume as measured by three-dimensional (3D) ultrasound. 28
They found that ovarian drilling resulted in a transient increase followed by a significant reduction in ovarian volume from a preoperative mean value of 12.2 mL to 6.9 mL 3 weeks after surgery. In the present study, this reduction in the ovarian volume after ovarian drilling (from 11 to 8.5 mL) was confirmed. In addition, the current study showed that this change in ovarian volume seems to last for up to 9 years.
The mechanism of this reduction of the ovarian volume by ovarian drilling is not clear. Tulandi et al. measured the volume of ovarian tissue destroyed by the needle electrode in an excised ovary using a 3-dimensional projection of colored serial microscopic images. 28 These researchers found that a single drilling would destroy an average of 0.4 mL of stromal tissue, and concluded that 10–15 drillings in an ovary would result in a total tissue destruction of 4–6 mL. This could account for the observed reduction of the ovarian volume.
It may also explain why the magnitude of reduction of the ovarian volume in the current study (from 11 to 8.5 mL), in which 3–10 punctures per ovary were applied, is smaller than that (from 12.2 to 6.9 mL) observed by Tulandi et al. who made 10–15 punctures per ovary. 28
However, it is not clear whether these findings in an excised ovary can be extrapolated to the intact ovary. Another possible explanation for the reduction of ovarian volume is the normalization of ovarian function produced by ovarian drilling. This is supported by the hypothesis that the typical morphologic features of PCOS, although still not fully understood, are caused by changes in ovarian function, that is, thecal hyperactivity and chronic anovulation. 29
It may be argued that the difference in ovarian volumes could be the result of inter-observer variability or the use of different ultrasound machines. These points are unlikely to be valid, as: (1) Earlier studies have demonstrated that real-time, 2-dimensional pelvic ultrasonography is a relatively accurate and reliable method of determining ovarian volume.30–32 (2) In this unit, two similar ultrasound machines have been used throughout the 9-year follow-up period.
It may also be argued that the reduction of ovarian volume after ovarian drilling is a sign of excessive ovarian tissue destruction and could be associated with an increased risk of ovarian damage and POF. However, as discussed previously, in this cohort of patients there was no POF, even though 14 patients were ages 39–45. It can, therefore, be concluded that this reduction of ovarian size is a sign of normalization of ovarian function in women with PCOS, rather than a sign of ovarian damage.
Conclusions
The long-term beneficial effects of ovarian drilling on ovarian morphology are supported further by the significant reduction in the incidence of women with ultrasound evidence of PCO at medium- and long-term follow-up compared with at the preoperative level. In conclusion, the current study's data show that OMLOD normalizes ovarian function and morphology in women with PCOS and that these effects seem to be sustained for up to 5 years in most patients.
Footnotes
Acknowledgments
The authors are grateful to all the women who participated in the study. The authors are are also grateful for the valuable help of the staff in the university imaging and biochemical departments, in El-Minya University Hospital.
Disclosure Statement
No competing financial conflicts exist.
*
Another part of the study, is trying to compare the long-term prognosis of OMLOD, compared with other modes of treatment rather than the surgical one.