
Abstract
Abstract
Introduction
Case
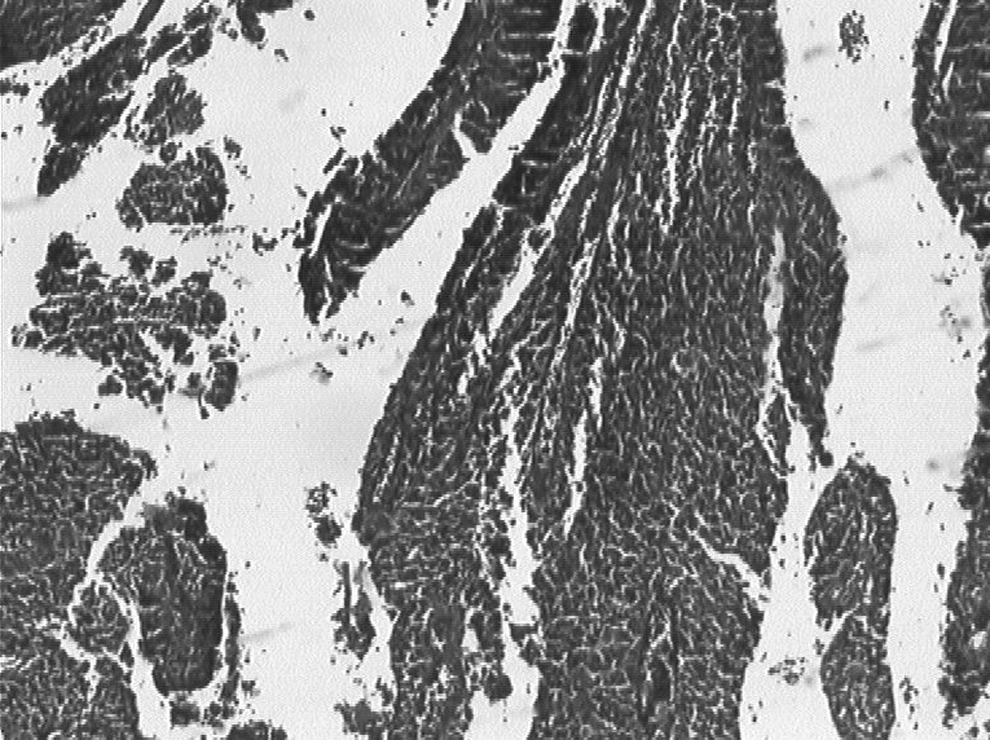
A 70-year-old woman with a history of 10 pregnancies and early marriage at 13 years old was complaining of abnormal vaginal bleeding for 6 years. A gynecologic and pelvic examination revealed a 4-cm mass in the uterine cervix, that was grossly friable and bleeding profusely, with no induration in the bilateral parametrium. A uterine cervical biopsy revealed an important tumoral and papillary proliferation with some transitional cells and some areas of in situ carcinoma. Cytonuclear atypies were frequent and evident. Mitoses were also frequent and mostly atypical (Fig 1). Dyskeratotic cells were noted. The pathologist diagnosed an undifferentiated infiltrating carcinoma. A computed tomography scan showed a 3-cm tumor localized in the uterine cervix, with no locoregional extension. Other radiological examinations yielded normal results, and no distant metastases were found. For this patient, preoperative staging was IB according to the staging system of the International Federation of Gynecology and Obstetrics (FIGO). The patient underwent a radical hysterectomy, a bilateral salpingo-oophorectomy, and pelvic lymphadenectomy (Wertheim type III). A macroscopic examination revealed an exophytic and ulcerative neoplasm that measured 2.2×1.4×1.3 cm and that was localized only in the uterine cervix. A histological examination showed evident papillary structures (Fig. 2). These papillae had a fibrovascular core with minimal inflammatory infiltrate. The papillary architecture was a dominant feature, with many mitotic figures. Keratinization was focally present. There were a few transitional cells. Some areas of intraepithelial neoplasm (CIN3) were seen. The vaginal tissue had some intraepithelial neoplasm (VAIN3). The invasion of the stroma was associated with nonspecific chronic inflammatory infiltrate. A pathologic examination did not show lymph node metastasis. These features led to the diagnosis of a PSCC. To assess the human papilloma virus (HPV) status of this tumor, in situ hybridization for HPV, common DNA was used to detect specific sequences of DNA shared by most types of genital HPV. This patient's tumor was negative for HPV. More specific testing using a polymerase chain reaction (PCR) was performed; this also yielded negative results for high-risk HPV 16 or HPV 18. She received adjuvant radiotherapy for its stromal invasion.

Medium-power view showing cytonuclear atypies and frequent atypical mitosis in the tumor of a 70-year-old Moroccan woman.
Low-power view showing papillary architecture in the tumor.
Results
The patient was seen 3 years after her surgery and did not have any recurrence or metastasis of her tumor.
Discussion
PSCC is a rare variant of SCC. A data review revealed < 50 cases. The largest series was reported by Mirashemi, 5 who discussed 12 cases diagnosed between 1990 and 1999, and Odid, 6 from Uganda, where cervical cancer is very frequent, with 20 cases diagnosed between 1963 and 1973.
The current authors reviewed 145 files of carcinoma of the uterine cervix in their institution, from 2005 to 2008. The most common histologic type was SCC as mentioned in the literature. The current case is the only PSCC diagnosed, probably because of the difficulty involved in diagnosing this subtype of carcinoma. This difficulty had been reported by Randall and Anderson. 2 In addition, it was observed that invasion may be difficult to reveal histologically unless deep biopsies are obtained,7,8 although there is no precise definition of PSCC. Ng 9 suggested that papillary tumors should be diagnosed only if papillary or anastomosing frondlike architectural patterns were seen in 70% of the tumor tissue. The papillary variant of SCC is histologically and clinically distinctive and should be segregated from VSCC. Some investigators have reported the similarity of these lesions to transitional cell carcinoma (TCC) of urothelial origin, but the relationship between PSCC and TCC is controversial and has not yet been defined conclusively. 5 In the present case, some transitional cells were noted, and the pathologist asked if there is any tumor in the urinary tract, but this was not the case.
Clinically PSCC, appears at any age in women of during the childbearing period, with greater frequency in postmenopause. PSCC is distinguished by late metastasis, late recurrences, and good prognosis. For example, Koenig 10 reported a vaginal recurrence 12 years after initial diagnosis, and Randall and Anderson also noted similar findings in 2 of their patients. 2 In Mirashemi's cases (12 with PSCC), 5 the one recurrence occurred 3 years after the initial diagnosis. Ten patients are currently free of disease and 1 patient was alive with disease despite stage IIIA presentation. PSCC tumors are proliferatively active even though they have a tendency to have an indolent clinical course. The role of HPV in the pathogenesis of this rare variant of cervical cancer has not been established yet. In Mirashemi's series of 12 cases, 5 6 of 12 cases were positive for HPV DNA; in these cases a high proliferative activity was observed. Randall and Anderson found no koilocytosis. 2 Also, Odida, with his large series of 20 patients from Uganda, did not find cytologic changes associated with viral replication. 6 The frequency of high-risk HPV recovery from a papillary squamous tumor is less than the reported from SCC in general. 11 In another study, Trivijitsilp analyzed papillary immature metaplasia, 12 and found 6 cases of papillary carcinoma and 1 case of papillary carcinoma in situ. In this group of 7 cases, 6 were positive for HPV nucleic acid, of which 4 were positive for HPV 16, 1 was positive for an unknown HPV type, and the sixth patient was HPV-negative. However, the seventh case in the group had carcinoma that involved the cervix and ovary, had transitional-cell differentiation, and was positive for HPV 18. The literature on the significance of HPV infection and prognosis in cervical carcinoma is mixed. There is some evidence that absence of the HPV in cervical carcinoma may be associated with poor prognosis factors, 13 but this concept has not been valid.2–11 Young et al. noted that contamination from adjacent areas of CIN may be the source of false–positive HPV detection in cervical carcinoma specimens. 15 In the current case, testing for HPV yielded negative results. Even though that patient's tumor had VAIN 3, this may explain the absence of recurrence in the 3 years of follow-up. Table 1 provides comparisons between the current case and other cases, with respect to the presence or absence of HPV.
Superscript numbers represent references.
Sawada M, Matsushima H, Kitawaki J. A case of papillary squamous carcinoma of the uterine cervix. Jpn J Clin Oncol 2010;40:373.
Fujimoto T, Sakuri N, Shimizu M, Watari H. Papillary squamous cell carcinoma of the uterine cervix: A report of two cases with human papillomavirus 16 DNA. Acta Obstet Gynecol Scand 2002;81:176.
The histologic features of PSCC are characterized by papillary architecture with fibrovascular cores of variable width. These papillae are covered with dysplastic epithelium, have mitotic figures visible in all levels of epithelium, have keratinization that is inconspicuous, and have koilocytic change that is mostly absent.
The histologic appearance of VSCC is also well-characterized in the literature. 14 The microscopic features are quite different from those of PSCC. VSCC tumors have an exophytic hyperkeratosis surface and push the border at the base. Cytological atypia is minimal or absent.
The histologic appearance of TCC includes fronds lined by polygonal cells, occasional nuclear grooves, and a complete absence of keratinization in all fields. 14
The tumor cells of PSCC are similar to cells in some conventional nonpapillary SCC of the cervix.
17
A possible explanation could be that the tumor cells in papillary carcinoma produce some factors that induce a papillary desmoplastic
Conclusions
PSCC is a rare subtype of SCC of the uterine cervix; this kind of tumor has specific biologic, histologic, and clinical characteristics. Current treatment recommendations are indistinguishable from those applied to the more-common SCC of the uterine cervix, given that that PSCC responds to the same therapeutic approaches used for SCC. PSCC's response to radiation, in particular, is the same as that of conventional SCC. However, the current authors look forward to gathering additional cases for further investigations into the biologic and genetic nature of PSCC. Such research may help to find therapies that can be applied directly to PSCC.
Footnotes
Disclosure Statement
No competing financial conflicts exist.