
Abstract
Abstract
Background:
Despite its favorable prognosis, endometrial stromal sarcoma (ESS) commonly recurs in the abdomen and pelvis. Rarely, it recurs in the cardiovascular system. A case of isolated cardiac ESS recurrence without concurrent vascular or abdominal disease is presented in this report.
Conclusions:
This is the first documented case of intracardiac recurrence of ESS without concurrent abdominal or intracaval disease. This isolated recurrence supports a hematogenous mechanism of spread for ESS rather than intracavitary diffusion. Aggressive surgical management continues to be an option for treatment. (J GYNECOL SURG 28:140)
Introduction
The majority of patients with ESS present with early stage disease. The survival rate for stage I ESS is high, with 5 and 10 year survival rates of 98% and 89% respectively. 1 Despite a favorable prognosis, in one third to one half of patients with early stage disease the disease will recur, although often this will happen many years after initial diagnosis. The majority of recurrences occur in the pelvis and abdomen; less frequent sites of recurrence include the vagina and lung. Unique to ESS is the potential mechanism of recurrence via extension into myometrial veins and parametrial lymphatics.3,4 This can result in intravenous spread extending into the inferior vena cava and even the cardiac chambers. 5
The first reported case of isolated cardiac ESS without concurrent caval disease is presented in this article.
Case
A 53-year-old Filipino woman was incidentally diagnosed with endometrial stromal sarcoma in 1998 at the time of her hysterectomy for menorrhagia. Following imaging studies, she was clinically found to have stage I disease, and observation was recommended. She presented in 2004, 6 years after initial diagnosis, with abdominal pain. She was diagnosed with abdominopelvic disease recurrence and underwent radical surgical resection of all visible disease, including small bowel resection with partial cystectomy (Fig. 1). In 2007, computed tomography imaging demonstrated abdominal recurrence extending into the right renal cortex. The patient declined medical and surgical management in favor of continued expectant management. However, in 2008, symptomatic hydronephrosis led to a second radical debulking of all visible disease, including a right nephrectomy.
High-power view of omental nodule resected during the second radical debulking in 2004. Monomorphic cells with uniform vascularity and a low mitotic count are consistent with recurrent ESS.
Eighteen months later the patient presented to her primary care physician with fatigue and intermittent tachycardia. A chest radiograph demonstrated cardiomegaly. A transthoracic echocardiogram revealed severe atrial enlargement with a 5×5 cm mass in the right atrium protruding into the right ventricle during diastole. Its appearance was most consistent with an atrial myxoma.
The patient subsequently underwent cardiac surgery requiring sternotomy and cardiopulmonary bypass. An atriotomy was performed and a large mass with a pedicled base was resected from the mouth of the coronary sinus. The surgical impression was that of an atrial myxoma. Final pathology revealed metastatic ESS, staining positive for CD10 and estrogen receptor (Figs. 2 and 3).
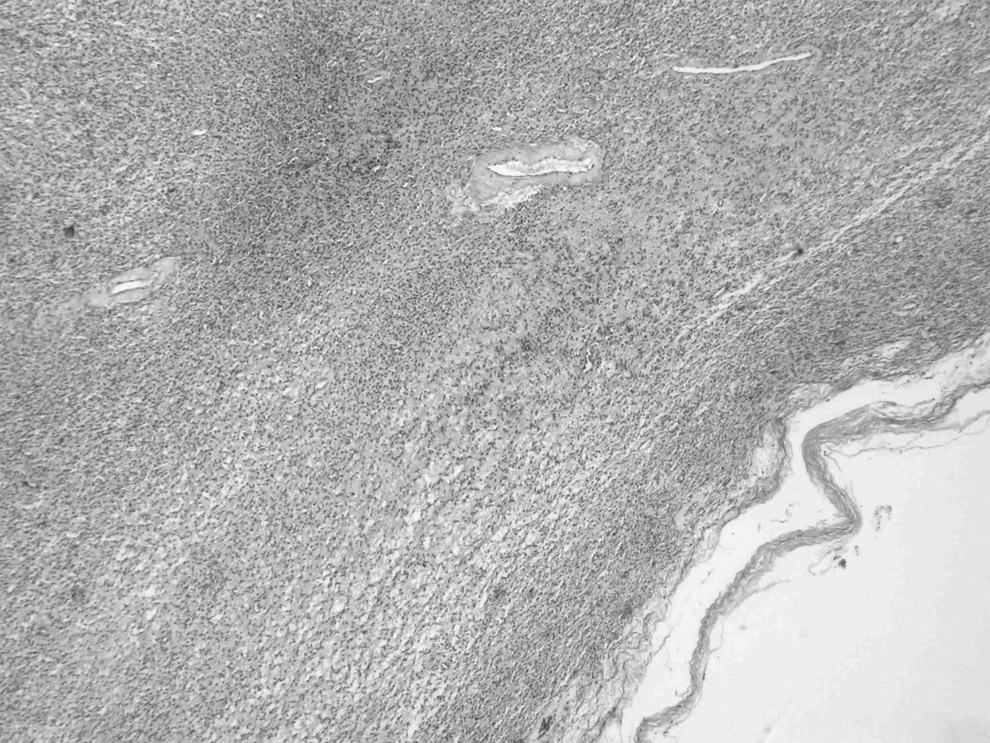
Low-power view of intracardiac metastatic lesion resected in 2010. Pathologic features are again consistent with recurrent ESS.

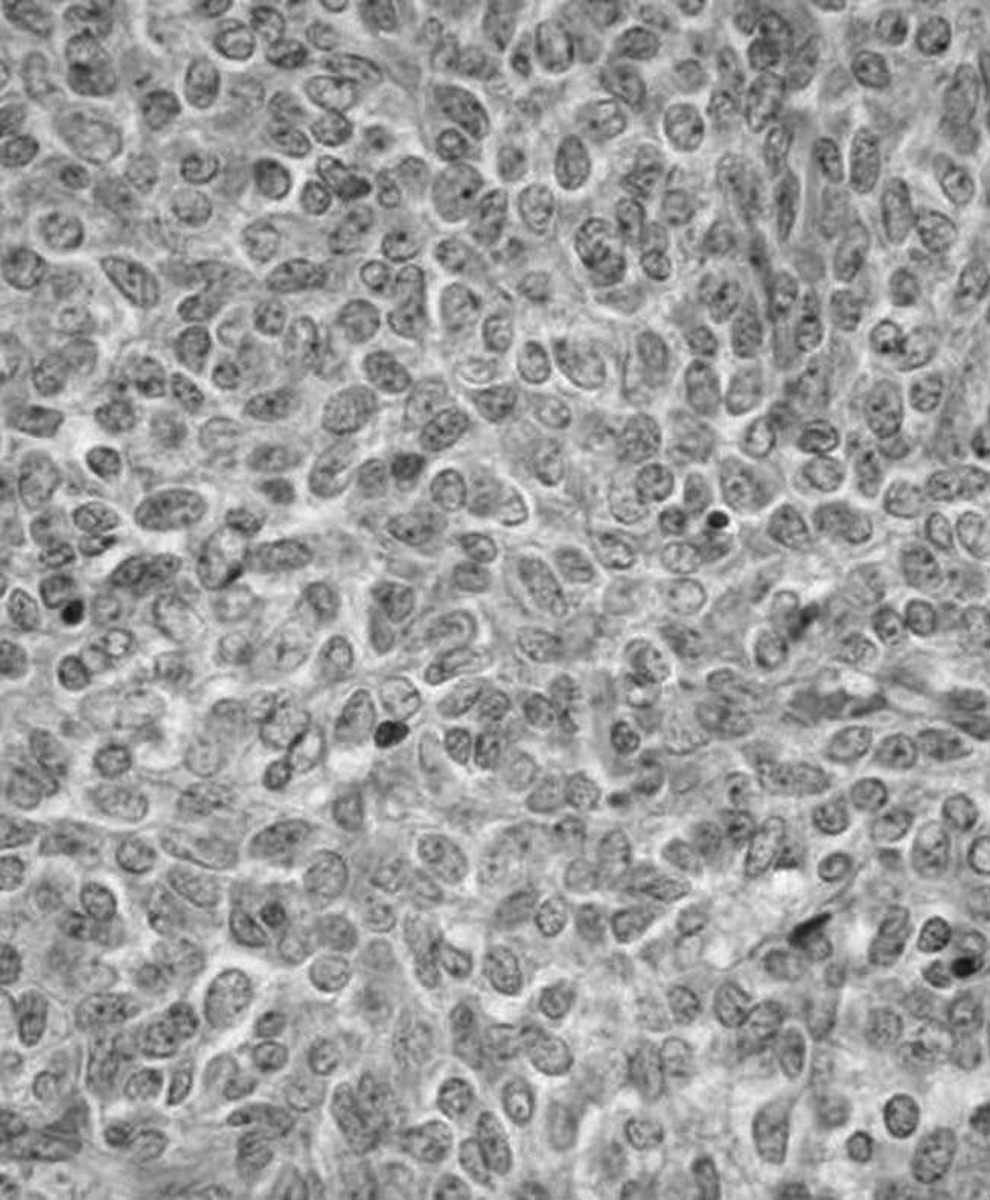
High-power views of intracardiac metastatic lesion resected in 2010. Pathologic features are again consistent with recurrent ESS.
Results
The patient's symptoms resolved and she is now currently without evidence of disease.
Discussion
Endometrial stromal sarcoma rarely involves the cardiovascular system. In a recent summary spanning 20 years of case reports, 19 separate cases of cardiovascular involvement with either primary tumor or secondary recurrence were reviewed. 5 All of these cases involved a tumor thrombus in the inferior vena cava with varying degrees of cardiac extension. None of these were isolated cardiovascular recurrences, as all 19 patients had evidence of concurrent abdominal disease. Radical resection, including either cavotomy or atriotomy was attempted in 10 of 19 patients, and was accomplished with low morbidity and high success.
In contrast to these cases, the case reported here is of isolated cardiac recurrence. This patient had no evidence of abdominal or caval disease. At the time of surgery, the atrial mass was grossly consistent with an atrial myxoma, although final pathology confirmed metastatic ESS.
Just as ESS rarely metastasizes to the heart, cardiac metastases from other cancers are considered rare. However, a recent review of primary postmortem studies found the incidence of cardiac metastases to be higher than anticipated, ranging from 2.3 to 18.3%. 6 Metastatic tumors are >100 times more common than primary malignancies of the heart.7,8 In female patients, the most common cancers that metastasize to the heart are from the lung, lymphoma, breast, and pancreas. Less frequent are malignancies of the stomach, ovary, liver, and colon, as well as melanoma and leukemia.6,7,9 In a large review of postmortem studies, no cases of metastasis from ESS were described. 7
Tumors can spread to the heart through various mechanisms including direct extension, and hemotogenous, lymphatic, and intracavitary diffusion (through the inferior vena cava [IVC] or pulmonary veins). Approximately two thirds of cardiac metastases are found in the pericardium, and only 5% involve the endocardium. A tumor involving the coronary sinus, as is presented in this case, is exceedingly rare. 6 Previous case studies have suggested tumor spread through intracavitary diffusion, whereas our case may uniquely represent hematogenous cardiac metastasis.
Conclusions
Similar to the caval tumors described previously, this case was treated successfully with surgical resection, which alleviated this patient's tachycardia as well as eliminating her isolated recurrence. This case further supports aggressive surgical management of late recurrences of endometrial stromal sarcomas.
Footnotes
Disclosure Statement
No competing financial conflicts exist.