
Abstract
Abstract
Introduction
Interstitial (cornual) pregnancy is a variant of ectopic pregnancy in which implantation of the embryo occurs in the interstitial segment of the fallopian tube. The interstitial segment is that portion of the fallopian tube that penetrates the myometrium. It has a length of 1–2 cm and a width of 0.7 cm. Its borders are the opening (ostium) of the tube to the endometrial cavity within the uterus and, laterally, the visible narrow segment of the tube. As the ectopic gestation grows, the interstitial segment is invaded and is encapsulated within the myometrium of the cornua of the uterus.
The incidence of interstitial (cornual) pregnancy is 2%–4% of all ectopic pregnancies and it has the highest mortality rate of all ectopic pregnancies. 2 Approximately 1 in 50 women with an interstitial (cornual) pregnancy dies. 3 Patients with an interstitial (cornual) pregnancy have a 7 times higher mortality than those with other types of ectopic pregnancies. 4 Diagnosis in a patient with a positive serum βhCG level is confirmed with a pelvic ultrasound, which visualizes an ectopic gestation within the interstitium. This can be confused with an angular pregnancy, in which the gestational sac is located within the endometrium positioned in the corner of the uterus near the fallopian tube insertion. A pregnancy located next to the interstitial section laterally is an isthmic tubal pregnancy. Two lines of treatment have been advocated: surgical intervention and medical therapy. The following case represents an interstitial (cornual) pregnancy that was diagnosed early and subsequently treated successfully with methotrexate. The advantages of this treatment will be discussed.
Case
A 34-year-old woman, gravida 8, para 2231, who was seen at the Reproductive Endocrinology Unit with a diagnosis of secondary infertility, presented to the emergency room with sudden onset of right lower quadrant pain. Her last menstrual period had been ∼ 6 weeks prior to presentation. Her serum βhCG was 38,807 mIU/mL. A pelvic sonogram showed an anterior uterus, normal in size, with an endometrial stripe of 10 mm. There was no intrauterine gestational sac identified. An 11-mm gestational sac was found in the right cornua of the uterus, which corresponded to a gestational age of 5 weeks, 1 day. This gestational sac contained a yolk sac and a fetal pole that corresponded to a gestational age of 6 weeks, 1 day (Fig. 1). There was fetal cardiac activity identified at a rate of 136 beats per minute. The right ovary contained a small simple cyst and the left ovary was normal. No free fluid was identified in the cul-de-sac.
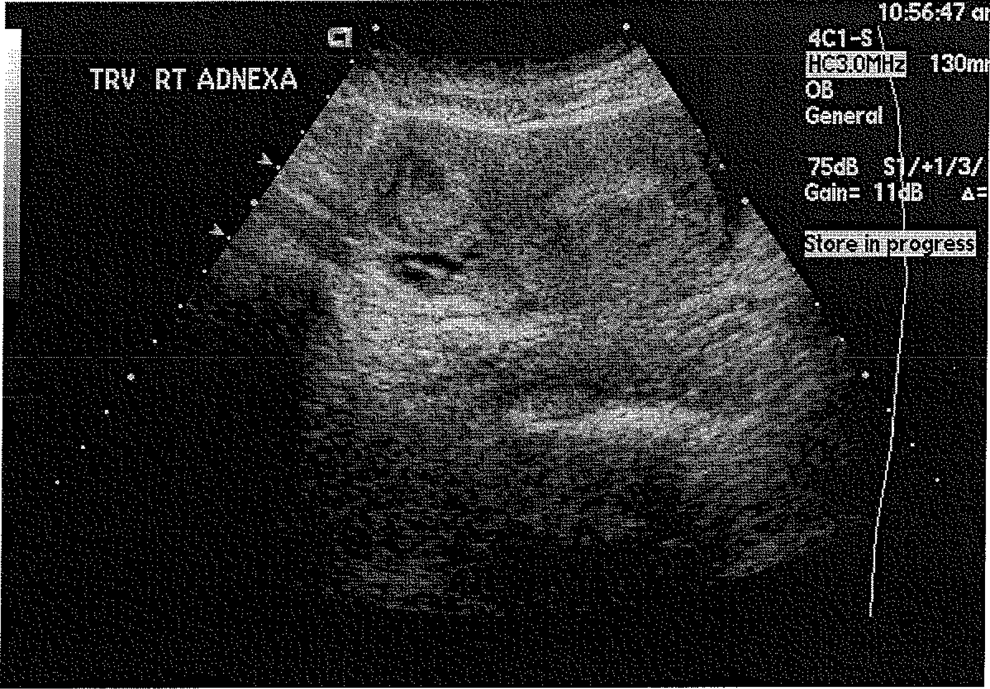
In 34-year-old woman presenting with pelvic pain and positive βhCG, a pelvic sonogram shows a right interstitial pregnancy with a normal endometrial stripe.
With a confirmed diagnosis of right interstitial (cornual) pregnancy, the patient was informed about both surgical and medical management. The patient consented to medical management with methotrexate. The blood count was normal with hemoglobin of 12.5 g/dL and a hematocrit of 37.2%. The white blood cell count was normal at 6.6 K/μL. The liver enzymes were normal. The patient weighed 53 kg and her height was 163 cm with a calculated body surface area of 1.55 m2. She was given methotrexate in a dose of 50 mg(m2). The calculated dose was 78 mg of methotrexate, which was administered i.m. On day 4 following treatment, her serum βhCG level increased to 53,128 mIU/mL. On day 7, βhCG levels decreased to 41,457 mIU/mL, a 20% decrease in βhCG level compared to day 4. This confirmed that the medical treatment had been effective. The patient continued follow-up with βhCG levels and sonograms. By day 54 following methotrexate administration, her βhCG level had decreased to 3 mIU/mL, which is in the negative range of the test (Table 1, Fig. 2).
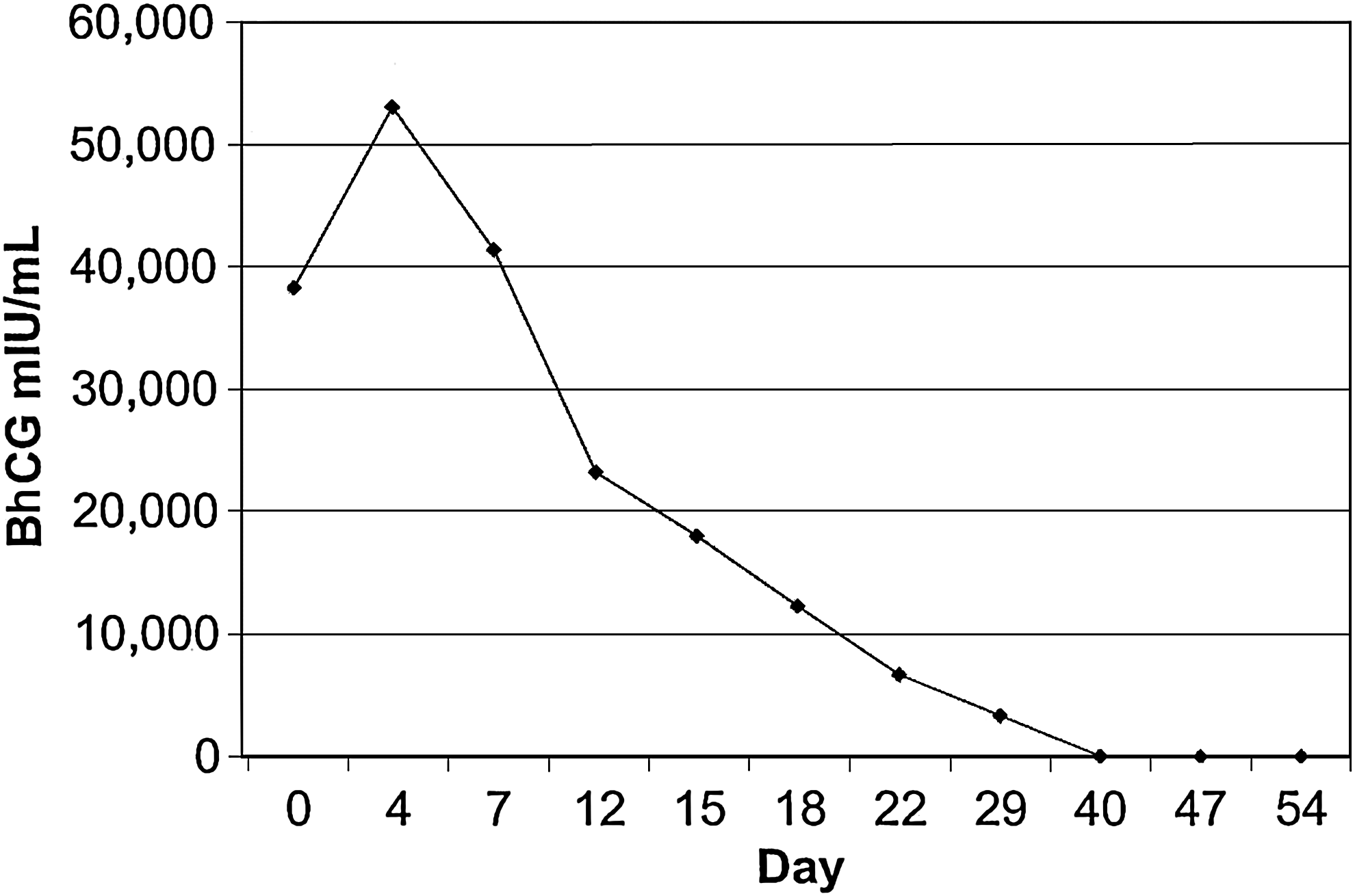
βhCG levels in MIU/mL over time following treatment with methotrexate.
Discussion
Interstitial (cornual) pregnancy is a rare form of ectopic pregnancy. Its location constitutes a diagnostic dilemma. The gestational sac is present in the cornua of the uterus surrounded by myometrial tissue, and has no connection to the endometrial cavity. 5 If these cases are not diagnosed properly, rupture of the cornual pregnancy can lead to massive hemorrhage and shock, as the cornua is a highly vascular part of the uterus. It is supplied by the Sampson artery, which is connected to both the uterine and ovarian artery.
Several forms of treatment have been described in the literature. Surgical evacuation of the products of conception followed by repair of the uterine wall in the cornua has been described using both laparotomy and laparoscopic procedures. 6 Another surgical management is excision of the cornua with the pregnancy inside it, and then repair of the uterine wall. 7 Complications include bleeding, and the defect that will be repaired may leave a scar and weak point in the uterus that could lead to rupture during subsequent pregnancies. 8 Another procedure that has been described is complete hysterectomy to preclude rupture of the uterus and massive bleeding. 9
It is essential that the correct diagnosis is made through proper ultrasound evaluation, as some of these cases are misdiagnosed as intrauterine pregnancy. Some patients have had attempts at induced abortion that were unsuccessful, and others have produced fatalities.
Hysteroscopic extraction of the cornual pregnancy has been described in 3 cases in the literature.10,11 This should not be a routine procedure and should only be performed by an expert with the conjoined use of laparoscopy, to avoid perforation of the cornua.
Uterine artery embolization has been recognized as a method of treatment for various obstetric and gynecologic conditions that cause uterine bleeding. 12 This procedure has been used for treatment of an interstitial (cornual) pregnancy in a case report from 2004. The patient had a twin interstitial (cornual) pregnancy and following embolization her βhCG levels became undetectable within 2 months. 13
Treatment with methotrexate for ectopic pregnancy was introduced because of its success as an antimetabolite drug for the treatment of cancers. 14 Methotrexate is a folinic acid antagonist that interferes with DNA synthesis in the rapidly proliferating trophoblast. In order to avoid side effects, the preoperative evaluation of the patient must include a complete blood count and liver function studies to ensure that there is no pre-existing bone marrow suppression and that the liver is functioning normally. Methotrexate has been given directly in the gestational sac successfully in patients with interstitial (cornual) pregnancies.15,16 It is also given systemically in the form of intramuscular injections or intravenous administration. 17 In this protocol, methotrexate is given in a dose of 50 mg/m2 body surface area. The criteria for the use of methotrexate in the treatment of tubal ectopic pregnancy have been described previously to include: 1) a pregnancy ≤3 cm in diameter by ultrasound; 2) a patient who is hemodynamically stable; 3) no fetal heart activity in the gestational sac; and 4) a βhCG level that must be <3000 mIU/mL. However, these criteria have evolved.
The present case is a patient who was counseled about surgical versus medical management and opted for medical treatment. Her βhCG level on the day of the treatment was 38,807 mIU/mL. There was fetal heart activity in the gestational sac. After 54 days, the βhCG had decreased to a negative value. The patient was followed regularly with βhCG levels and ultrasounds that showed gradual decrease in the size of the gestation sac, and finally, complete resorption of the pregnancy (Fig. 3). In addition, the uterus and fallopian tubes remained intact. Follow-up by hysterosalpingogram confirmed the patency of both tubes (Fig. 4). Subsequently, as of this writing, the patient successfully achieved a normal intrauterine pregnancy at 17 weeks.
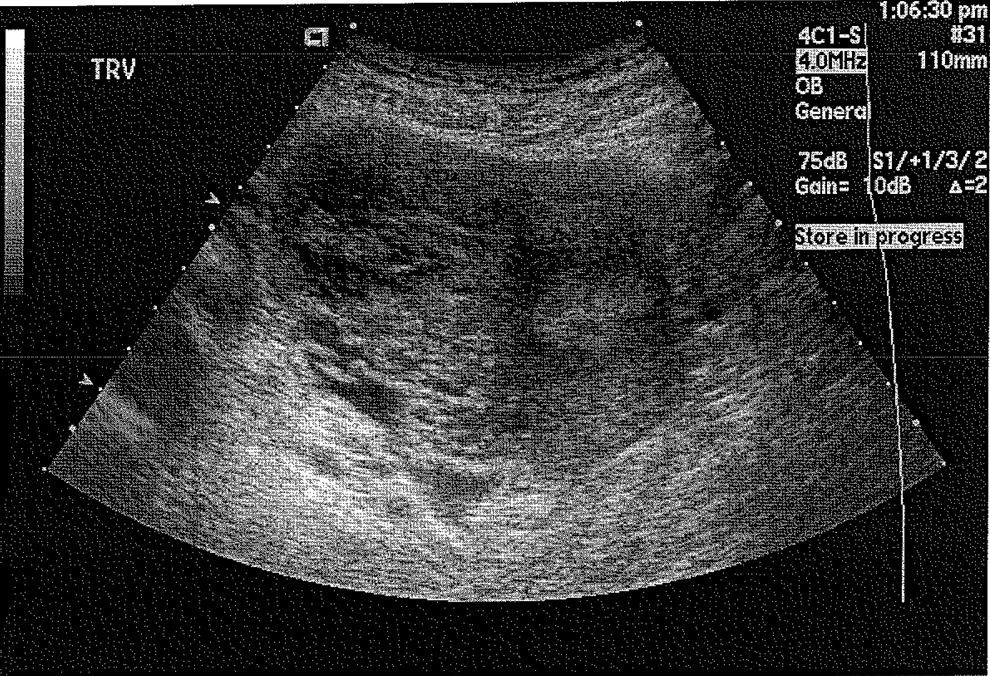
Methotrexate treatment shown to be effective in the presence of high βhCG levels and positive fetal heart activity.

Follow-up hysterosalpingogram reveals patency of both tubes.
Methotrexate treatment for interstitial (cornual) pregnancy should be considered in order to preserve fertility potential. The original criteria for medical treatment have been modified to include patients with various types of ectopic pregnancy. The size of the pregnancy as defined by sonogram evaluation has been expanded to include those >3 cm in size. Fetal heart activity is not now considered a contraindication. In addition, βhCG levels have not been a restrictive factor for medical treatment. The report of a patient with a βhCG level of 102,000 mIU/mL who was successfully treated with methotrexate, has been published. 18 In another report, methotrexate was successful in >80% of proximal tubal ectopic pregnancies with βhCG levels >100,000 IU/L. 19
Conclusions
In conclusion, medical treatment for unruptured interstitial (cornual) pregnancy is effective and prevents uterine surgery that may have complications for future pregnancy.
Footnotes
Disclosure Statement
No competing financial conflicts exist.