
Abstract
Abstract
Introduction
Dysfunctional uterine bleeding affects 1 in 5 premenopausal women, and it can significantly reduce their quality of life and cause anemia. 1 Treatment possibilities for dysfunctional uterine bleeding consist of anti–fibrinolytic tranexamic acid; nonsteroidal anti-inflammatory drugs; combined oral contraceptives; progestogens; danazol; analogues of gonadotropin-releasing hormone or the levonorgestrel-releasing intrauterine device; and surgical measures including curettage, endometrial ablation/resection, or hysterectomy.1–5 Danazol and curettage, however, are not recommended by the National Institute for Health and Clinical Excellence (NICE) to the National Health Service (NHS) as a therapeutic treatment for dysfunctional uterine bleeding.
Since the 1990s, endometrial ablation methods were introduced as a minimally invasive alternative treatment to hysterectomy in cases of therapy-resistant dysfunctional uterine bleeding. The second-generation techniques (thermal balloon endometrial ablation, microwave endometrial ablation, hydrothermablation, bipolar radiofrequency endometrial ablation, and endometrial cryotherapy) have largely replaced the first-generation techniques (transcervical endometrial resection or rollerball endometrial ablation under direct visualization of the uterine cavity), which are only indicated when combined with hysteroscopic myomectomy or polypectomy. In general, these newer techniques can be used when the uterus is not greatly enlarged and the uterine cavity is not distorted. 5
In April 2007, NovaSure® endometrial ablation was introduced in the Meander Medical Centre. The NovaSure endometrial ablation system consists of a three-dimensional, triangular shape bipolar ablation device that covers the entire uterine cavity. The power (maximum 180 W) generated by the NovaSure radiofrequency generator has a cutoff limit set at a tissue impedance of 50 Ω. The maximum treatment time is 120 seconds; a self-terminating procedure is based on the tissue impedance or time. Uterine-wall perforation is detected because of inability to pressurize and/or to maintain pressure in the uterine cavity with CO2. A uterine assessment with CO2 must be performed before the start of the treatment. NovaSure enables controlled endometrial ablation. The folded device has a diameter of 7–8 mm; for its introduction in the uterus a cervical dilatation (by means of a Hegar's dilator) up to 7.5 French is required. It is suitable for a uterus with a minimum cornu-to-cornu distance of 2.5 cm and a depth of 6–11 cm as measured with uterine sounding. Total sounding length of the uterus minus the cervical length equals the length of the uterine cavity. This length will be preset, resulting in unfolding of the device for only the preset number of cm. The power is automatically selected based on the cornu-to-cornu distance and the uterine cavity length. Continuous monitoring of tissue impedance controls the depth of the ablation; once the myometrial layer is reached, tissue impedance increases to 50 Ω resulting in an automatically switch off. 6
It is possible to perform the NovaSure treatment in the operating theater (OT) or the outpatient clinic (OPC). Advantages of the NovaSure procedure in the OPC are a quick procedure for the patient, without the side effects of general or spinal anaesthesia, and not requiring hospital admission. There is a reduction in costs when a patient is treated in the OPC, because OT and OT employees (anesthetists and OT assistants) and admission to the gynecology ward are not necessary. However, a NovaSure treatment in the OT guarantees a painless procedure, whereas the OPC procedure is not painless. A comparison of NovaSure treatment between OPC and OT patients has not yet been reported.
Following the introduction of NovaSure endometrial ablation in the Meander Medical Centre, a retrospective study was initiated. The objectives of this retrospective study of 112 patients were, first, to describe the effectiveness of and patient satisfaction with NovaSure endometrial ablation, and second, to compare the NovaSure procedures performed in the OPC with those performed in the OT.
Materials and Methods
Details of ethics approval
All patients who participated in this retrospective analysis gave consent for the use of the data for scientific research in which their data were processed anonymously.
Subjects
This study was conducted on all NovaSure endometrial ablation procedures (n=112) performed during the period from April 2007 to October 2008 in the Meander Medical Centre, Amersfoort, The Netherlands. Patients referred by their general practitioners for dysfunctional uterine bleeding were offered treatment with NovaSure endometrial ablation after exclusion of (pre)malignant uterine lesions. All NovaSure procedures were performed by 2 gynecologists. The patients were offered the choice of undergoing the NovaSure treatment either in the OPC or in the OT. In the OPC, a cervical block was given, and, in the OT, patients received either spinal or general anesthesia, according to their wishes. Patients of the OPC group were prescribed naproxen (500 mg 12 hours and 1 hour prior to the NovaSure procedure). After the treatment, patients in both groups were prescribed tramadol (100 mg every 12 hours) in case the analgesic effects of paracetamol and naproxen were insufficient.
The patients treated in the OT were admitted to the daycare department, whereas patients who had undergone the treatment in the OPC could leave the hospital directly after the procedure.
At least 6 months following the NovaSure procedure, the patients (n=112) were sent a questionnaire concerning their experience and satisfaction with the NovaSure treatment. Four patients did not return the questionnaire; these patients were approached by telephone. One patient stated in the telephone interview that she had not returned the questionnaire because she was not satisfied and was referred to a university hospital for a second opinion, and a hysterectomy was performed at that hospital. One patient stated that she had not returned the questionnaire because she did not understand the questions; however, she said that she had amenorrhea. For 3 patients, the phone number was not correct any more, and these patients were considered to be lost to follow-up. A total of 107 patients (95.5%) was included for complete follow-up.
Data collection and definitions
Data were collected by reviewing the medical charts and a questionnaire.
Dysfunctional uterine bleeding was defined as a duration of menstrual blood loss for >7 days, an increased quantity of menstrual blood, or irregular menstrual blood loss.1,2 Subjective experience of patients was of major importance for the definition of dysfunctional uterine bleeding.
The data included the ages of the women at the time of the NovaSure treatment. The location of the NovaSure treatment—OT or OPC—was recorded. For patients treated in the OT, the type of anesthesia (spinal or general) was registered. The sounding length (cm), cervical length (cm), length of the uterine cavity (cm), width of the uterine cavity (cornu-to-cornu distance in cm), the power (W) used, the duration of the NovaSure treatment (seconds) was recorded.
The questionnaire consisted of questions regarding menstruation before and after the NovaSure procedure: median duration of the menstruation (days), presence of dysmenorrhea, and presence of clots. After the NovaSure procedure, the presence of amenorrhea (absence of menstruation: 0 days) was recorded. Furthermore, the presence of pain and nausea experienced during the NovaSure procedure (this was only analyzed for the patients who had been treated in the OPC) was questioned. A score from zero 0 to 10 was used, in which 0 indicated no pain/nausea and 10 indicated worst pain/nausea possible. Use of analgesics (days) after the NovaSure procedure was recorded as well. Finally, the patients were asked to give an overall satisfaction score assessing the NovaSure treatment, once more a score ranging from 0 to 10 was used.
Statistical analysis
To check for accuracy, the data entered were double checked. All analyses were performed by using SPSS version 15.0. Statistical comparisons for continuous variables were made with a Mann–Whitney U test. Dichotomous and categorical variables were compared using χ2 test or Fisher's exact test when appropriate. Within-subject analyses were performed using repeated measures.
A p-value<0.05 was considered to be statistically significant.
Results
Baseline characteristics
Table 1 shows the baseline characteristics of the total cohort (n=107), the patients treated in the OPC (n=57) and the patients treated in the OT (n=50). Of the patients treated in the OT, 21 (42%) received spinal anesthesia and 30 (58%) received general anesthesia. No significant differences in baseline characteristics were noted between the OPC and OT cohorts.
Comparisons were made with a Mann-Whitney U-test. OPC, outpatients clinic; OT, operating theater; SD, standard deviation; min, minimum; max, maximum.
Effectiveness
The mean duration of menstruation prior to the NovaSure treatment was 13 days (standard deviation [SD]=9). The mean duration of menstruation, the presence of clots, and dysmenorrhea were not significantly different between the OPC and OT groups (Table 2). In more than half of the patients amenorrhea occurred, and this was not significantly different between patients treated in the OPC and in the OT.
Comparisons were performed by a Mann–Whitney U-test a Chi-square test or Fisher's exact test where appropriate.
In the patients who did not have amenorrhoea.
OPC, outpatients clinic; OT, operating theater; SD, standard deviation; min, minimum; max, maximum.
Table 3 shows a comparison of menstruation characteristics before and after the NovaSure procedure. The mean duration of menstruation significantly decreased, as did the presence of blood clots and dysmenorrhea (all p<0.001).
Comparisons were performed by repeated measures.
SD, standard deviation; min, minimum; max, maximum.
Pain experience and patient satisfaction
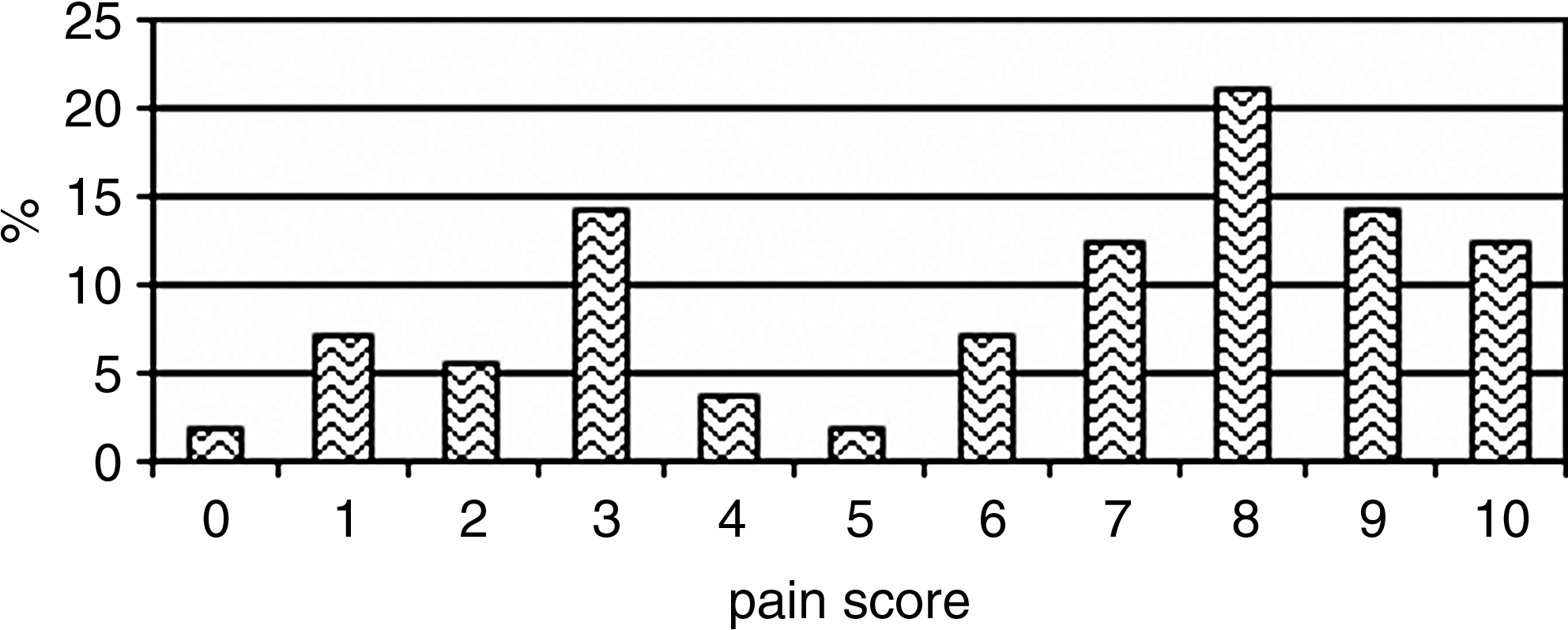
Figure 1 presents the pain experience (based on a pain score ranging from 0 to 10) of the NovaSure procedure reported by the patients in the OPC group. The majority reported a score of 8 (21.1%), however a variable distribution is shown.
Outpatient clinic
Table 4 shows the mean pain score and satisfaction score. The mean menstruation pain score in the total cohort was 5.7 (SD=3.1) and was not significantly different between the OPC and OT patients (p=0.179). The mean NovaSure pain score experienced by the OPC group was 6.3 (SD=3.0). A menstruation pain score of ≥9 (mean menstruation pain score of total cohort+1 SD) was considered to indicate an extremely painful experience. OPC patients who reported that the NovaSure treatment had been extremely painful (a score of 9 or 10) appeared to have a significantly higher mean pain score during menstruation prior to the NovaSure treatment: 7.0 (SD=2.1), compared to a menstruation pain score of 4.7 (SD=3.2) in patients who reported the NovaSure treatment to be less painful (score≤8, p=0.014). See Table 5.
Comparisons were performed by a Mann–Whitney test.
OPC, outpatients clinic; OT, operating theater.
High NovaSure pain score was defined as 9 or 10, and a low pain score of ≤8. Menstruation pain score ranged from 0 to 10. Comparison was performed by a Mann–Whitney U test.
SD, standard deviation.
Furthermore, 80.6% of the total cohort were reported to have used analgesics after the NovaSure procedure. The mean duration of analgesics usage was 3.8 days (SD=6), and this was not significantly different between the OPC and OT groups (3.3 days [SD=5.3] and 4.4 days [SD=6.8], p=0.396).
Nausea was reported in 36.8% of the patients, but the majority (61.9%) had a nausea score of ≤5.
Patient satisfaction was evaluated with the same score range as pain experience was evaluated. The majority (53.3%) had a score of 10 and stated that they were completely satisfied, followed by a score of 9 in 14% of the patients and a score of 7 in 10.3% of the patients
Table 4 shows the mean satisfaction score of 8.5 in the total cohort; the satisfaction score was significantly higher in the OT group (p=0.027). In 2 patients (1.9%) who were completely dissatisfied after the NovaSure treatment, a hysterectomy was performed.
Discussion
In this study population of 107 women who had undergone NovaSure endometrial ablation because of dysfunctional uterine bleeding, there was an amenorrhea rate of 51.4%, a hysterectomy rate of 1.9%, and a patient satisfaction score of 10 (indicating complete satisfaction with the NovaSure treatment) in 53.3%.
The NovaSure treatment had resulted in a significantly decreased mean duration of menstruation, significantly decreased presence of blood clots, and decreased dysmenorrhea (after at least 6 months up to 2 years following the treatment).
Bongers et al. reported an amenorrhea rate of 43% and a hysterectomy rate of 6.3% 1 year after the NovaSure treatment. In this study, a significant reduction of duration of menstruation was also found, as well as a decreased presence of dysmenorrhea. 7 According to Kleijn et al., an amenorrhoea rate of 48% and a hysterectomy rate of 10.3% were found after 5 years of follow-up of 126 patients treated with NovaSure endometrial ablation. Furthermore, an improvement of quality of life over time was found. 8
The OPC group reported the pain experience of the NovaSure procedure to be almost similar to the pain experienced during menstruation. However, OPC patients who reported that the NovaSure treatment had been extremely painful scored significantly higher on the menstruation pain score prior to the NovaSure treatment than did patients who reported the NovaSure treatment to be less painful.
Although no significant difference in effectiveness was shown between the OPC and OT groups, a significantly higher satisfaction was reported in the OT group, which probably resulted from the pain experienced by the patients in the OPC group.
In the study period from April 2007 to October 2008, 116 patients were scheduled for the NovaSure treatment, the procedure was be performed on 112 patients; for 4 patients the NovaSure endometrial ablation system did not pass their uterine assessments with CO2, resulting in a failure rate of 3.4%. These failures occurred shortly after initiating the NovaSure treatment in the Meander Medical Centre. Since ultrasonographic measurement of uterine size is now performed prior to offering the NovaSure treatment to the patients, no more CO2 failures have occurred.
A hysterectomy had been performed on 2 of the 107 patients studied. However, 1 of the patients who was not included in the follow-up was referred to a university hospital after being dissatisfied with the NovaSure treatment result, and she underwent a hysterectomy. Including this patient would have resulted in a hysterectomy rate of 2.7%.
One of the limitations of this study was the retrospective design. Second, in some studies perimenopausal women are excluded, because the occurrence of amenorrhea after the NovaSure treatment could have been influenced by the initiation of menopause. However, the indication for the NovaSure treatment was, for all patients, the presence of dysfunctional uterine bleeding, and the aim was to evaluate the effectiveness of and patient satisfaction with the NovaSure treatment in patients with a correct indication (dysfunctional bleeding) for the procedure.
Furthermore, the relation between pain experience during menstruation and pain experience during the NovaSure treatment is probable, but numbers are small. Therefore, the important finding that patients in the OPC group had higher mean menstruation pain score needs to be confirmed in a larger study population.
In this study population, no complications occurred. However, it should be realized that transmural coagulation of the myometrium as well as mechanical perforation of the uterus has been reported with the NovaSure device, which could lead to bowel, bladder, and vascular injuries.
Conclusions
NovaSure endometrial ablation is a valuable and effective treatment option for patients with dysfunctional uterine bleeding. It is possible to perform the treatment both in the OT and OPC. Significantly lower patient satisfaction was found in the OPC, probably resulting from the pain experienced by these patients. NovaSure treatment in the OPC is good option for a selected patient population. In the OPC, patients who reported a high level of pain during their menstrual period were found to have significantly greater pain experience of the NovaSure procedure; therefore, we recommend that these patients be treated in the OT.
Footnotes
Acknowledgments
Authors E.L. and A.B. performed all NovaSure treatments in the study population. M.J.C. performed the data collection and statistical analysis. S.A.M.W. assisted in the data collection.
Disclosure Statement
No competing financial conflicts exist. No funding was provided for writing this article.