
Abstract
Abstract
Introduction
This report describes a case of SCC arising in a tubal teratoma in a 50-year-old postmenopausal female, a type of case that has not previously reported to the best of the current authors' knowledge.
Case
A 50-year-old postmenopausal female (gravida 6, para 5) presented with a lump and and pain in her abdomen for 10 days. The pain was not relieved when she took analgesics. She had was no history of bleeding from her vagina and no fever. She had been tubectomised 20 years prior. There was no relevant family history.
Physical examination
A general physical examination revealed an oriented (conscious and aware of surroundings) female with mild pallor and cervical lymphadenopathy. Her blood pressure was 110/70 mm Hg, her pulse rate was 72 pulses per minute, and her respiratory rate 18 breaths per minute. An abdominal examination revealed a firm and mobile mass of 20 weeks' gravid-uterus–size with a smooth surface and regular margins. Ascites was present. A speculum examination showed that her cervix was congested, and a vaginal examination allowed the mass to be felt in her anterior fornix. Ultrasonography (US) testing revealed a bilobed cyst measuring 11×7cm, filled a with thick fluid and showing hyperechogenecity in the center. The clinical and US findings were suggestive of an ovarian cyst.
Surgery
An exploratory laparotomy revealed a multilobulated tumor measuring 10×10 cm, arising from the patient's left Fallopian tube and adherent to her omentum. A pedicle of the tumor, along with the affected Fallopian tube, had undergone torsion. Her uterus, cervix, bilateral ovaries, and right Fallopian tube were normal. A total abdominal hysterectomy, with a bilateral salpingo-opherectomy were performed, alongwith excision of the tumor and omentectomy.
Histopathology
Gross examination revealed a cystic mass, measuring 12×10×6 cm, attached to the patient's left Fallopian tube. Her omentum was attached at places on the external surface of the mass. When the mass was cut open it was noted to be partially cystic and partially solid. A tuft of hair was present within the cyst. A cut section of the Fallopian tube also revealed solid gray white areas. The distal and proximal portion of the tubal lumen appeared to be normal (Fig. 1). Microscopic examination revealed features of an MCT in which squamous epithelium had undergone malignant transformation, resulting in invasive SCC. Other mature components present were skin adnexal structures and mature cartilage (Figs. 2 and 3). Her omentum showed infiltration by the tumor. Fine-needle aspiration cytology from a cervical lymph-node showed metastatic deposits from the SCC (Fig. 4).

Photomicrograph showing mature cystic teratoma of Fallopian tube with solid gray white areas (black arrow) and cystic component containing hairs (white arrow).
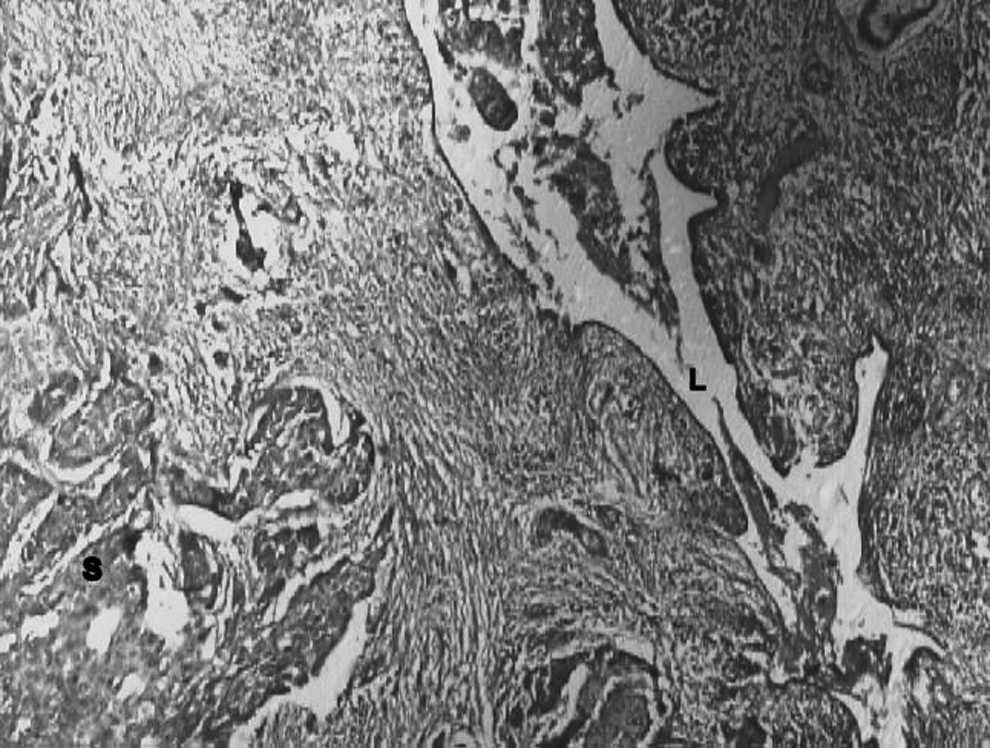
Photomicrograph showing Fallopian tube lumen (L) and focus of squamous cell carcinoma (S). H & E×40.
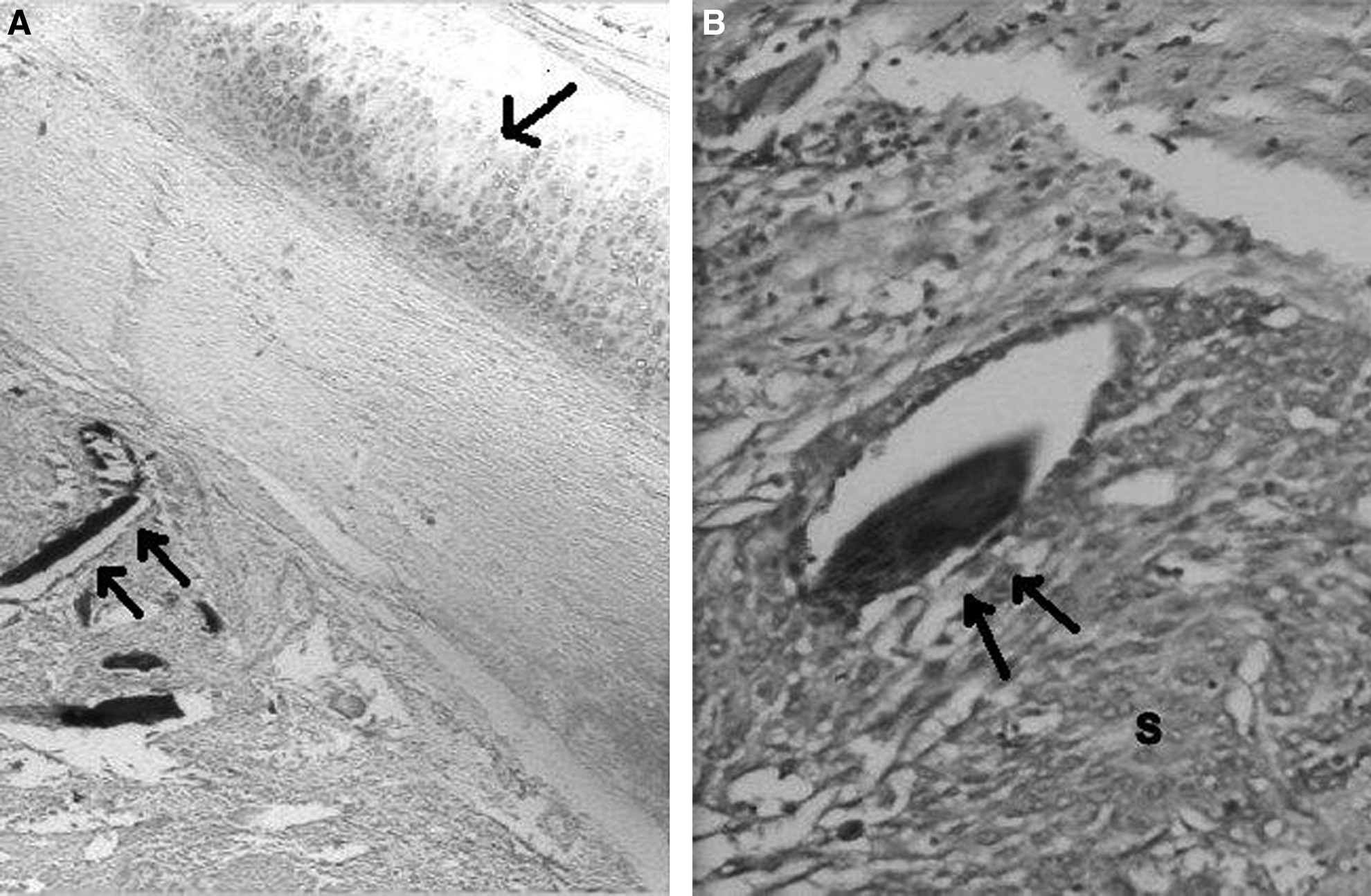
Photomicrograph showing
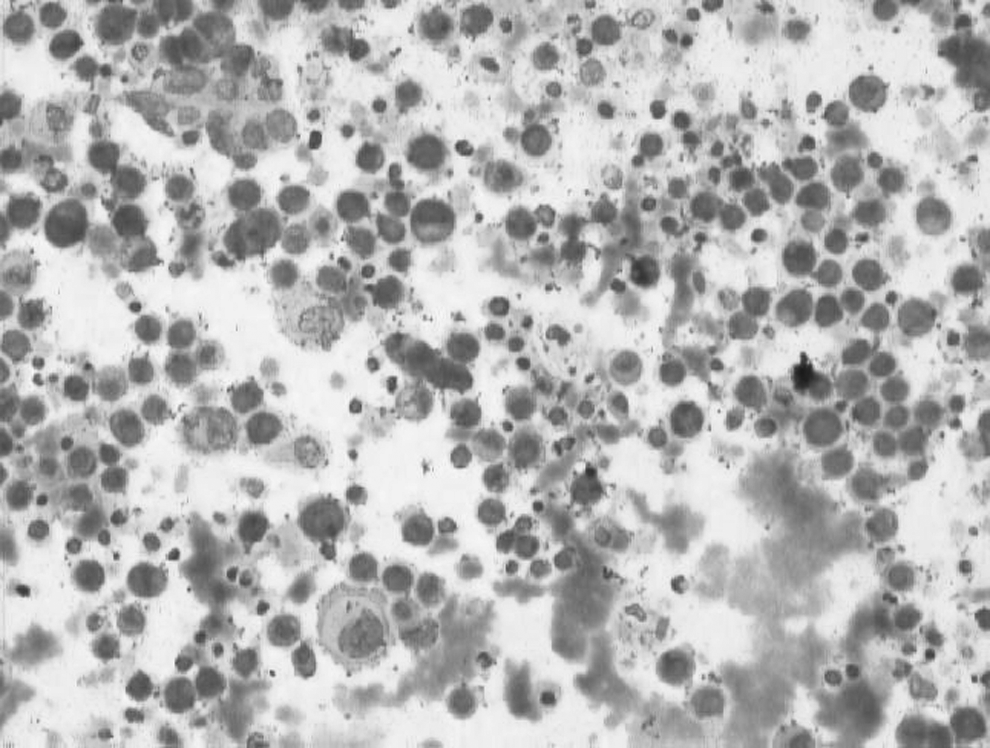
Cytology smear showing metastasis of squamous cell carcinoma to cervical lymph node. (Romanowsky×200
Results
Postoperatively, the patient underwent chemotherapy, but she died from progression of the disease 9 months after surgery.
Discussion
Primary neoplasms of the Fallopian tube are rare. Adenocarcinoma is the commonest Fallopian tube tumor, but it still constitutes < 1% of all malignancies of the female genital tract. 6
Approximately 58 cases of mature teratomas of the Fallopian tube have been reported in the literature, with the first case being reported in 1865. To date, 4 cases of immature teratomas of the Fallopian tubes have also been reported, but tubal teratomas undergoing malignant transformation in the form of SCC has not been reported in the literature so far. 3
The age of these tumors occurring in the 4th decade of life.1,2,6 Most of the patients are nulliparous or have a parity < 2.2,6 Patients usually present with colicky abdominal pain, dysmenorrhoea, leucorrhoea, menstrual irregularity, and postmenopausal bleeding.2,6 Unusual presentations include coexistence with tubal pregnancy, a free floating pelvic mass, and rupture into the rectum. 6
Tumors are located most frequently in the lumen, often attached by a pedicle to the inner tubal wall; they may, however, be intramural or attached to the serosa. 1 The size of tubal teratoma varies widely, ranging from 0.4 cm to 20 cm.1,2,6
The criteria for diagnosing a primary tubal malignancy are very rigid, because, by convention, a carcinoma involving both the endometrium and Fallopian tube is classified as an endometrial tumor, and a malignancy involving both an ovary and a tube is regarded as an ovarian neoplasm. A primary tubal malignancy is diagnosed, based on its location and by virtue of complete separation of the tumor from the uterus and ovaries. 7
The origin of teratomas has been a matter of interest, speculation, and dispute for centuries. Now, the most widely accepted theory is the parthenogenic theory, which suggests an origin from primordial germ cells. 4 Two other theories, one theory suggesting an origin from blastomeres segregated at an early stage of embryonic development and the second theory suggesting an origin from embryonal rests have been proposed. Support for germ-cell theory has come from the anatomical distribution of the tumors, which occurs along the line of migration of the primordial germ cells from the yolk sac to the primitive gonad.2,4,6 The incidence of tubal teratoma is much lower, despite tubal derivation from the urogenital ridges and their proximity to the ovaries; both of these factors might be expected to lead to a higher occurrence of these tumors in the Fallopian tubes. 2
Histologically, tubal teratomas are similar to teratomas of the ovary and elsewhere. Malignant transformation has been reported in ∼ 1.5%–3% of cases of ovarian teratomas. Any of the tissues present in a MCT may undergo malignant transformation; however, the most common is SCC (75%). Others types of cancers include carcinoid tumor, thyroid carcinoma, basal-cell carcinoma, adenocarcinoma of the intestinal epithelium, malignant melanoma, leiomyosarcoma, chondrosarcoma, and hemangiosarcoma.8,9
The malignant component may involve only a part of a tumor, making it difficult to identify. Grossly, this component appears as a polypoid mass, a mural nodule, or mural plaque as an area of hemorrhage and necrosis. SCC arising in MCT can be seen microscopically as nests of squamous cells infiltrating the stroma or as a cyst lined with malignant squamous cells. Other histologic patterns include papillary, insular, verruciform, or spindle cell type cells. 5
The prognosis of MCT undergoing malignant transformation has been reported to be very poor, with a 5-year survival of only 15%–30%. The potential prognostic predictors include tumor grade, FIGO stage, rupture, or spillage, vascular involvement, and mode of tumor infiltration.5,8 Better prognosis has been reported when the malignant element was SCC, as compared to other histologic types of tumors. 8
Conclusions
Given that an exact management protocol has not been defined because of the rarity of this conditoin, it seems prudent to follow current management guidelines for ovarian immature/malignant teratomas, depending upon the patient's desire to maintain her reproductive function and menopausal status. 3 Surgical staging based upon the cytologic examination of peritoneal washings and pleural fluid for malignant cells, and screening of retroperitoneal, inguinal, and other lymph nodes as well as the hepatic parenchyma for metastasis is particularly important. 7
As the incidence of malignancy of the Fallopian tube is very low, and tubal teratoma undergoing malignant transformation has not been reported so far, this possibility should be considered after excluding the direct extension to the Fallopian tube from malignancies of adjacent organs such as the ovaries, uterus, and cervix.
Footnotes
Acknowledgements
Thanks are due to all coauthors and the technicians for making significant contributions to this study.
Disclosure Statement
No financial conflicts of interest exist.