
Abstract
Abstract
Introduction
Only a few studies have evaluated the consumption of piritramide administered by PCA in combination with various non-opioid analgesics after different surgical procedures.22–25° There is still no previous controlled study using piritramide in combination with various non-opioid analgesics after abdominal hysterectomy.
The primary objective of this prospective, randomized, double-blind, placebo-controlled study was to compare postoperative piritramide consumption alone or in combination with parecoxib versus paracetamol (acetaminophen) or metamizol (dipyrone) for providing pain relief in adult patients recovering from abdominal hysterectomy during the first 24 hours. Secondary objectives were to compare the pain intensity and patient's satisfaction.
Materials and Methods
The investigative protocol was approved by the institutional review board at Klinikum Bernburg Teaching Hospital, and all patients provided written informed consent before enrolment. The study began in March 2004 and ended in August 2007. Inclusion criteria were that patients were between the ages of 18 and 75 years, and had American Society of Anesthesiologists (ASA) physical status 1–3. Patients with a history of significant cardiac, pulmonary, hepatic, or renal disease; morbid obesity; chronic pain and drug or alcohol abuse; and contraindications or previous adverse reaction to any of the drugs used in the study were excluded. Also not included were patients unable to cooperate.
Patients meeting the inclusion criteria and scheduled for elective non-malignant abdominal hysterectomy under general anesthesia were visited the night before surgery and the use of PCA for postoperative pain relief as well as scales for the determination of pain intensity and patient satisfaction were explained. After informed consent, 120 patients were assigned to one of four groups, based on a computer-generated randomization table (http://www.randomization.com).
The four study groups were (A) placebo, (B) parecoxib 40 mg, (C) metamizol 1 g, and (D) paracetamol 1 g (Table 1). The drugs were dissolved in 100 mL normal saline and given via IV infusion over 15 minutes. Patients in the placebo group received only 100 mL of normal saline. In all groups, 10 minutes before extubation 2 mg piritramide (Dipidolor® Janssen-Cilag) was injected. During the postoperative period, piritramide was offered in form of PCA by means of a PCA pump as an electronically steered syringe pump.
min, minutes; h, hours, postop., postoperation.
The study solutions were prepared by one of the researchers who was not involved in the intraoperative and postoperative treatment of these patients, whereas postoperative data were collected by anesthesiologists who were blinded as to the treatment used. Other caregivers were also unaware of the analgesic drug that would be used for each patient during the study. The group assignment code was retained until the conclusion of the study. The observation time extended during a period of 24 hours after surgery.
For premedication, midazolam 7.5 mg (Dormicum®, Roche Pharma AG Grenzach-Wyhlen, Germany) was administered orally 60 minutes before the surgical procedure. On the patient's arrival in the operating room, standard monitors were applied. Electrocardiogram (ECG), noninvasive arterial pressure, heart rate, and peripheral oxygen saturation (Sp
After the administration of oxygen via an anesthetic breathing circuit and face mask for 3 minutes, 1 mg vecuronium bromide (Norcuron®, Organon GmbH, München, Germany) was given as pre-block while anesthesia was induced with 2 mg/kg propofol (Propofol® 1%, Fresenius Kabi Deutschland GmbH Bad Homburg, Germany) intravenously, followed by 80 mg suxamethonium chloride (Lysthenon® 2%, Nycomed Deutschland GmbH Konstanz, Germany) to facilitate endotracheal intubation. After intubation, mechanical pressure- controlled ventilation was initiated at a flow rate of 1 L/min in a semi-closed system (Cicero; Dräger, Lübeck, Germany) and nitrous oxide in oxygen at a ratio of 1:1 was administered throughout surgery. The inspired oxygen and end-tidal concentrations of carbon dioxide (CO2) were measured continuously at the proximal end of the endotracheal tube using a calibrated infrared gas analyzer (Dräger PM 8050, Dräger, Lübeck, Germany). Ventilation was adjusted to maintain end-tidal CO2 between 34 and 38 mm Hg.
Muscle relaxation was obtained with vecuronium bromide 0.6 mg/kg and monitored by the train-of-four stimulation method using a peripheral nerve stimulator. Anesthesia was maintained with a supplemental infusion of 3–6 mg/kg/h propofol and 3–10.5 μg/kg/h remifentanil (Ultiva®, GlaxoSmith Kline GmbH & Co. KG München, Germany) required to maintain an adequate depth of anesthesia with mean arterial pressure and heart rate within a 20% range of preoperative values. Surgery was performed via a Pfannenstiel incision. Intraoperative blood loss was determined by combining the blood collected in the suction canister as well as by estimating the blood present in the surgical sponges. No patient needed a blood transfusion. The total quantity of the infused solution during surgery was between 1500 and 2500 mL.
Fifteen minutes before the expected end of surgery, each patient was treated according to list of randomization (Table 1). Then, infusion of propofol and remifentanil was stopped and residual muscle relaxation was reversed with 0.5 mg atropine and 5–10 mg pyridostigmine at the end of the procedure when necessary. The lungs of each patient were ventilated with 100% oxygen at a flow rate of 5 L/min. Spontaneous recovery of neuromuscular function was confirmed by train-of-four monitoring. The trachea was extubated when adequate spontaneous ventilation (tidal volume >5 mL/kg) and response to verbal commands were established. The pre-programmed PCA equipment (Master PCA, Fresenius Vial Infusion Technology, Brezins, France) was provided with a 50-mL disposable syringe, and 45 mg piritramide in 45 mL saline solution was prepared for each patient. The PCA administered boluses of 2 mL (= 2 mg piritramide) with a lockout interval of 10 minutes and a maximal volume of 30 mL in 4 hours. A bolus of 2 mg piritramide was first injected 10 min prior to the extubation in the operating room. Postoperative pain was then treated by self-administration of small doses of IV piritramide using the PCA pump already mentioned.
Thereafter, the patients were directly transferred to the PACU, where further clinical observations were done for by an independent, blinded observer who was unaware of the administered study drugs. On arrival, patients were asked every 2 hours for the first 6 hours, and afterwards once every 6 hours, to quantify their pain experience at rest on a visual analog scale (VAS) between 0 and 10, with 0 representing no pain and 10 the worst imaginable pain. Likewise, pain relief was assessed by the patient on a 0–3 verbal rating scale (VRS) (0=none, 1=mild, 2=moderate, 3=complete). Patient satisfaction with the effectiveness of pain therapy was inquired at 6-hour intervals by using a four-point scale that shows the verbal expressed satisfaction of assigned numerical values: 1=poor, 2=moderate, 3=good, 4=very good. The cumulative piritramide consumption within 24 hours postoperatively was recorded at discharge from the PACU and after 6, 12 and 24 hours on the display of the PCA pump.
Data were first processed in Microsoft® Excel 2000 and then evaluated with the statistical program SPSS for Windows in version 15.0 (SPSS Inc. Chicago, IL). The primary efficacy measure was accumulated piritramide consumption. Sample size was calculated to detect a difference between groups of 30% (α=<0.05 and β=0.2; power=0.8). The power analysis was based upon a variation (standard deviation [SD]) of piritramide consumption from pilot data. Based on these assumptions, a priori power analysis suggested a sample size of 30 patients for each group.
Statistical analysis
For examination of normal distribution, the Kolmogorov–Smirnov test was applied. One-way analysis of variance (ANOVA) in normal distributed continuous variables and Kruskal–Wallis test in abnormal distributed or ordinal variables between the groups were used. When significant differences were determined, pairwise intergroup comparisons using a Mann–Whitney U test were followed. Categorical data were analyzed using χ2 or Fisher's exact test as appropriate. Differences were judged significant at p<0.05.
Results
One hundred and twenty female patients, scheduled for elective non-malignant abdominal hysterectomy under general anesthesia, were enrolled and randomized in the study, with 30 patients in each group. Because there were no dropouts and no protocol violations in any of the patients studied, a complete data set was obtained for all four groups.
Table 2 contains the demographic and patient-referred data in each group. The four groups were similar with respect to age, weight, height, body mass index (BMI), and ASA physical status.
ASA, American Society of Anesthesiologists; SD, standard deviation; m, meters; BMI, body mass index.
The piritramide consumption in the four groups over 24 hours is presented in Figure 1. The first required amounts of piritramide in the PACU were similarly high in all groups and also, the incremental piritramide consumptions after 6, 12, and 24 hours showed no significant difference among the four groups. Likewise, the frequency of PCA bolus demands did not differ in the four groups (Table 3). Also with the cumulative PCA-piritramide consumption no significant difference could be found among the groups (Fig. 2). However, the cumulative piritramide consumption was slightly lower in the metamizol group at 24 hours, whereas the patients in the parecoxib group had the highest piritramide consumption as compared with the other groups.
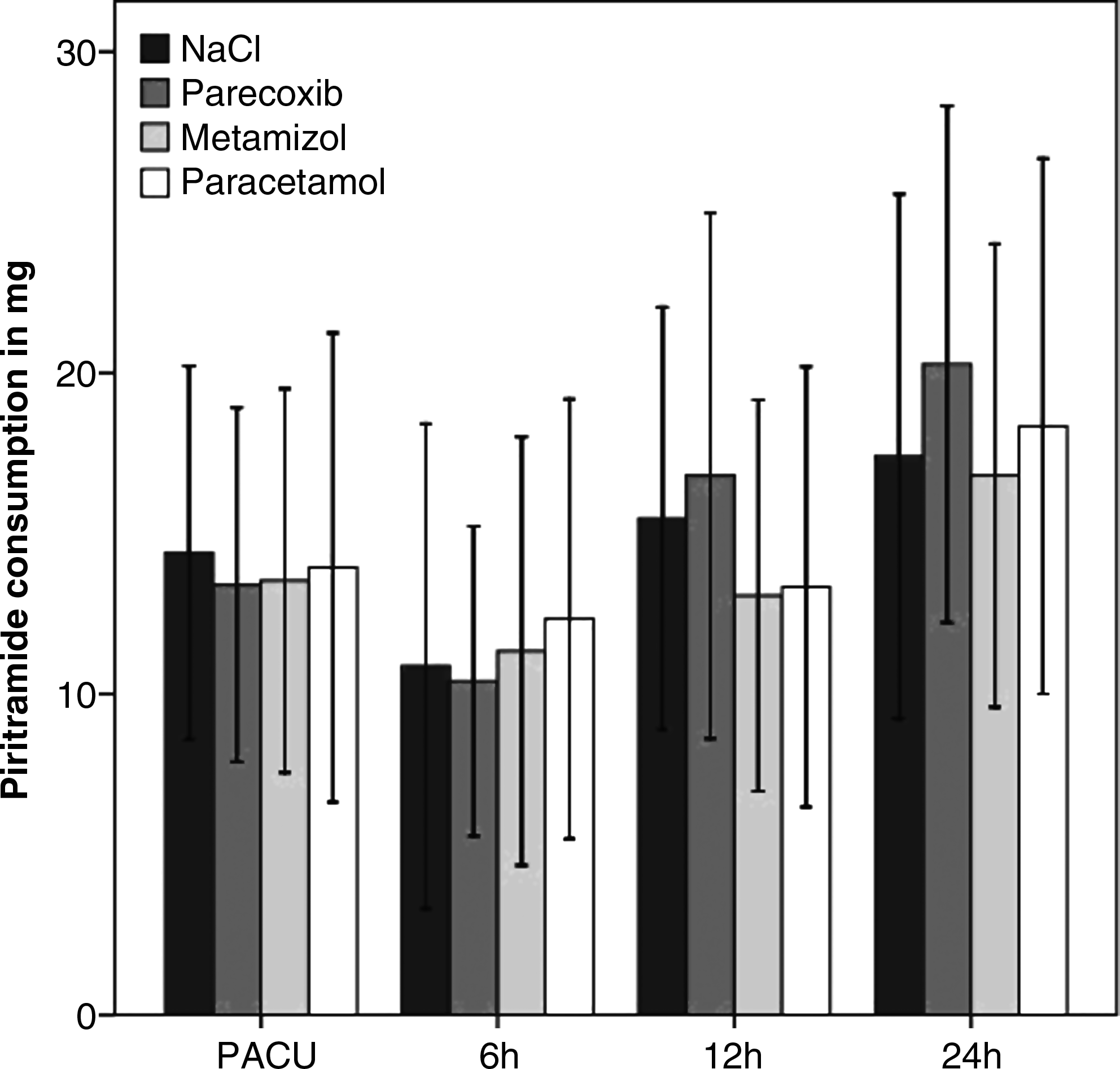
Piritramide consumption in mg (mean and standard deviations) over 24 hours postoperatively. PACU, postanesthia care unit.
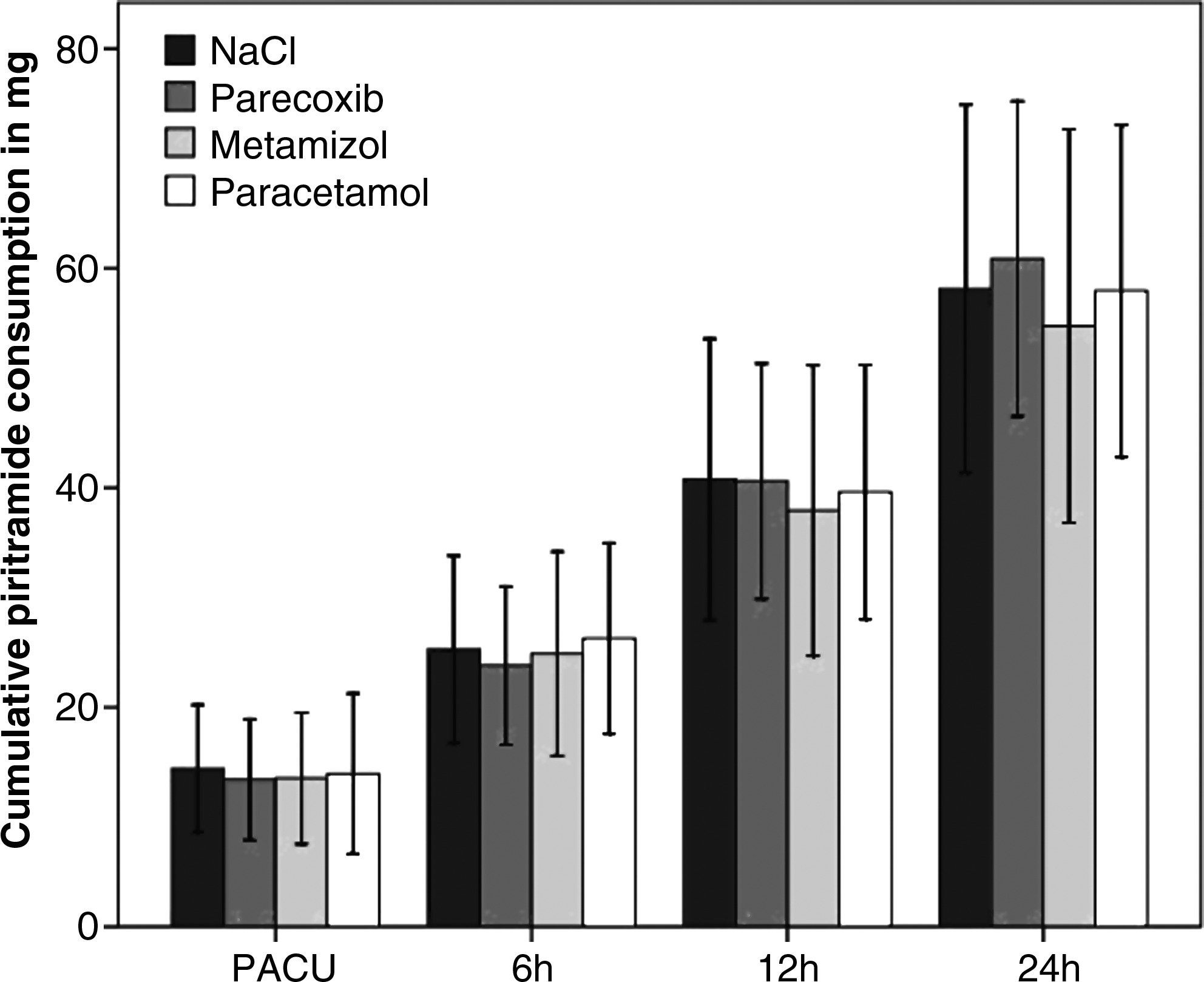
Cumulative piritramide consumption (mean, standard deviation) in all groups at different investigation times. There was no significant difference among the groups. PACU, postanesthesia care unit.
PCA, patient-controlled analgesia; SD, standard deviation; PACU, postanesthesia care unit; h, hours.
The VAS scores showed a significant difference only at 6 hours after surgery between the NaCl group and the paracetamol and parecoxib groups (Fig. 3). In all groups, VAS scores were highest upon arrival in the PACU. The highest value was found in the NaCl group with 6.5, and the lowest value was found with 5.1 in the metamizol group. Afterwards the VAS score dropped for all groups almost continuously after surgery, with the highest value of 2.6 in the NaCl group and the lowest of 2.2 in the paracetamol group after 24 hours. In all groups, the VAS score was <4 at 4 hours postoperatively, and at 12 hours was <3. Furthermore, it is evident in Figure 3 that the VAS score for the placebo group with NaCl was at all times slightly higher than for the other groups, indicating that the patients felt obviously somewhat stronger pain.
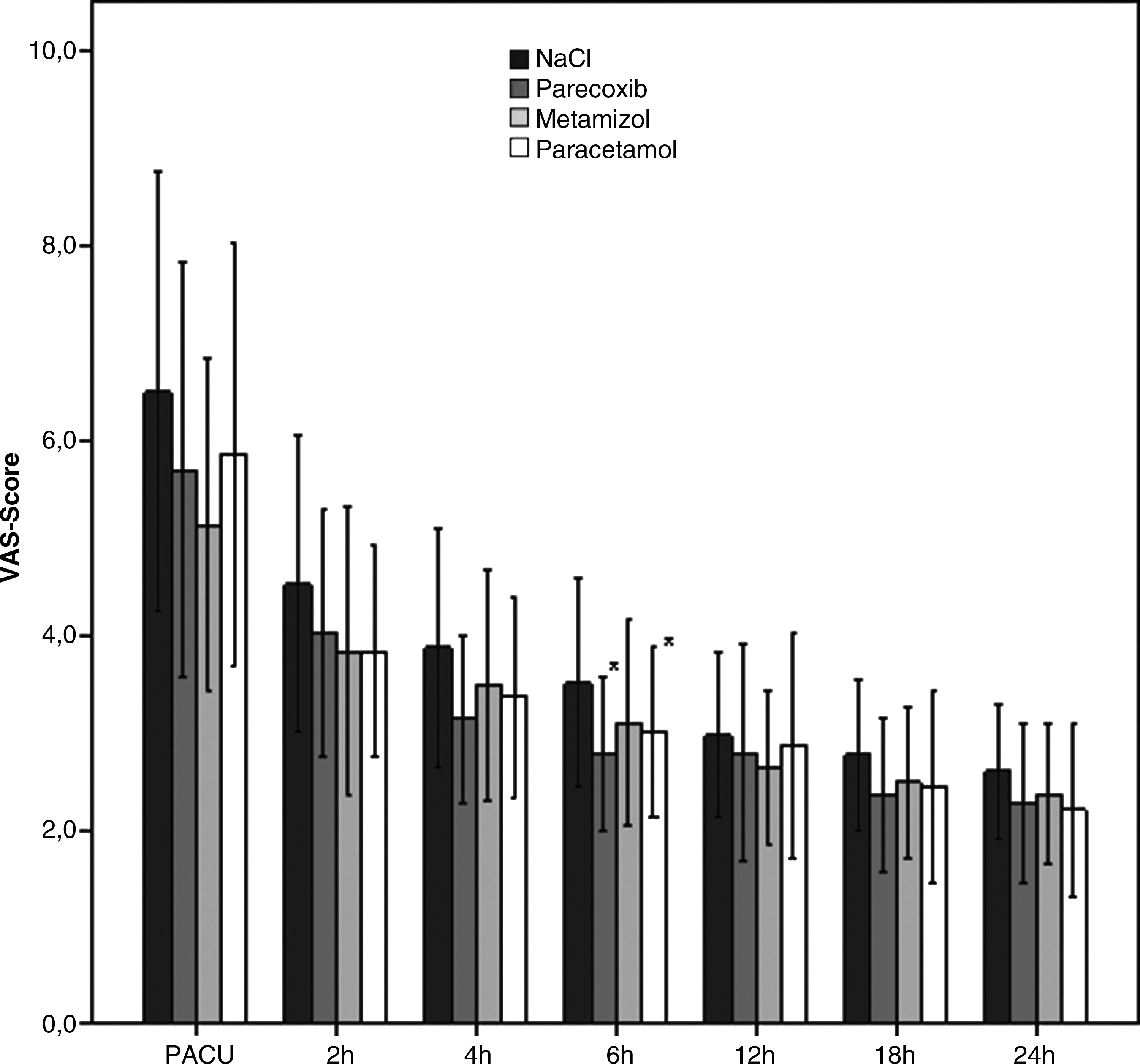
Visual analogue scale (VAS, mean and standard deviations) over 24 hours postoperatively (0=no pain; 10=worst imaginable pain). *P<0.05 parecoxib and paracetamol versus NaCl. PACU, postanesthesia care unit.
Overall, infrequent nausea and vomiting were observed, although the patients had not received an antiemetic prophylaxis. No drug reactions apart from nausea and vomiting, which were treated with antiemetics on the ward, occurred in this study. In regard to the patient's satisfaction, no significant difference was found during the investigation period among the four groups. In the PACU, satisfaction of the patients assessed on the four-point scale was moderate, and then rose continuously to good and very good in all groups. Likewise, the pain relief score in all groups showed no significant difference.
Discussion
This study examined the opioid-sparing effects and analgesic efficacy of parecoxib, metamizol, and paracetamol when used as part of a multimodal treatment of pain associated with abdominal hysterectomy.26–28 The drugs were selected because they are routinely used for the IV treatment of postoperative pain.
Parecoxib is the only parenterally administered cyclo-oxygenase-2 (COX-2) inhibitor. Among the anti-inflammatory drugs, selective COX-2 inhibitors have the most supportive data for their beneficial effects as part of multimodal analgesia, and offer benefits with regard to their adverse effect profile. 29
Metamizol is still widely used in Europe and South America, and has additional antispasmodic and antipyretic effects in patients with visceral pain. In other countries, it is banned because of an association with life-threatening blood agranulocytosis, although the strength of the association has been a matter of much debate.30–34 However, in the discussion of metamizol-induced agranulocytosis, the overall risk should be considered in comparison with other non-opiod analgesics that are not devoid of serious side effects. 30 Nevertheless, because of the risk of agranulocytosis, patients should probably be monitored for blood dyscrasias and, extremely rarely, broad-spectrum antibiotics with hematopoietic growth factors should be administered if agranulocytosis occurs. 23 The third drug used in our study, paracetamol, can now also be administered intravenously, and is therefore gaining renewed interest in this setting because of its minimal adverse effects.
As opioid, patients self-administered or “titrated” piritramide via an IV PCA to a satisfactory level of effect. A small bolus dose in combination with a short lockout time improves individual titration of analgesia and takes into account the large inter-individual variance on analgesic requirements. 24 A bolus dose of 2 mg piritramide with a lockout time of 10 minutes is routinely prescribed in Germany. 22 A background infusion was not provided in this study because of a possible increased risk of respiratory depression. 6
Abdominal hysterectomy was selected because it may produce considerable postoperative pain, and there is obviously no randomized, double-blind, placebo-controlled study that compares IV administered parecoxib, paracetamol, or metamizol, on piritramide consumption in the early postoperative period of abdominal hysterectomy.
In the results of this current study there was no opioid-sparing effect, as demonstrated by the lack of significant differences in piritramide consumption among the four groups at any investigation time in a 24-hour postoperative period. Only piritramide consumption was slightly lower in the metamizol group at 12 and 24 hours compared with the three other groups (parecoxib, paracetamol, and placebo), whereas the patients of the parecoxib group had the highest, however not significant, piritramide consumption at 12 and 24 hours compared with the metamizol, paracetamol, and NaCl groups. Therefore, this study showed no statistically significant opioid-saving effect by administering additional non-opioid analgesics. In the literature, there are controversial results in this matter. Because of the lack of studies with piritramide in abdominal hysterectomy, the current study had to draw on studies with piritramide in different operative procedures or studies after abdominal hysterectomy using paracetamol, metamizol, or parecoxib combined with other opioids, rather than piritramide in comparison for appraisal of this study's results.
The current study confirmed the previously published results by Soltesz et al., who demonstrated that parecoxib 40 mg twice daily provides postoperative pain relief similar to that achieved with metamizol 2.5 g injected intraoperatively, followed by 1 g every 6 hours over a period of 48 hours after vaginal hysterectomy, and found no significant differences with regard to piritramide consumption. 25 Other studies also did not report any significant difference in time to first request for piritramide and cumulative consumption of piritramide as assessed by the PCA data.23,35,36 In contrast, several conventional nonsteroidal anti-inflammatory drugs (NSAIDs) and selective COX-2 inhibitors have been shown to reduce opioid requirements and improve analgesia.37,38 Ng et al. found that parecoxib 40 mg IV was associated with significant reductions in 24-hour morphine consumption and pain intensity following abdominal hysterectomy. 39 Also, other studies found a reduction in morphine consumption when combined with NSAIDs or COX-2-inhibitors after abdominal hysterectomy.7,11,12
Apart from the lacking superiority of one of the investigated drugs in combination with piritramide given over PCA, a significant difference in the VAS pain scores was registered only at 6 hours after surgery between the NaCl group as compared with the paracetamol and parecoxib groups. However, the VAS score was higher in the placebo group at all investigation times than in the drug groups, and the highest level of the VAS score was registered upon arrival in the PACU in all groups. At 12 hours and thereafter, however, VAS scores were all <3. Therefore, it may be difficult to demonstrate an additional benefit with an analgesic when baseline pain is low in all groups. By comparing our VAS scores with those of Soltesz et al. 25 the magnitudes of the VAS scores after vaginal hysterectomy directly after surgery were very similar to those in the current study (VAS: 6). However, in their study, mean VAS dropped to 1 after 12 hours, whereas the current study had VAS scores >2 despite higher piritramide consumption. This implies a higher pain intensity in abdominal hysterectomy.
Despite avoiding antiemetic prophylaxis, no drug reactions apart from nausea and vomiting, which were treated with antiemetics on the ward, occurred in the current study. In addition to patient-related factors, the use of total IV anesthesia with propofol and remifentanil for abdominal hysterectomy may have contributed to a low incidence of postoperative nausea and vomiting as already reported.3,5 In regard to the patient's satisfaction with the pain medication, no significant difference was found during the investigation period among the four groups.
Conclusions
The missing opioid-sparing effect in this study might have been caused by failure to administer equipotent doses of non-opioid analgesics. The maximum dosage recommended by the manufactures for IV application in adults is 40 mg parecoxib twice a day. In contrast, we used 1 g metamizol and 1 g paracetamol three times daily (t.i.d.), whereas the maximum dose recommended by the manufacturer is 1 g four times daily (q.i.d.). In addition, opioid dosage immediately following surgery in all groups was obviously not high enough to provide adequate postoperative pain control after remifentanil/propofol-based anesthesia for abdominal hysterectomy. It may therefore be better to use lockout times of 5 rather than 10 minutes. 23 This might also explain why the results in this study might be at odds with previously published data.3–5
Footnotes
Disclosure Statement
No competing financial conflicts exist.