
Abstract
Abstract
Introduction
Case
A 41-year old nulliparous Chinese woman presented to the Gynaecology Clinic with symptoms of monthly abdominal pain lasting for 2 days. Her last menstrual period had been 6 months earlier and she complained of hot flushes. She had had an intrauterine device (IUD) fitted in China in 1998 and requested it to be removed. On speculum examination no threads were visible. On the ultrasound scan, the IUD was noted to be present in the endometrial cavity (Fig. 1) and the patient was booked for a hysteroscopy and removal under general anesthetic after appropriate counseling.

IUD appearance on ultrasound scan.
At hysteroscopy, the IUD appeared to be an elongated coiled metallic structure lying on the posterior uterine wall closer to the fundus. The cervix was dilated to No. 8 Hegar's. Initially, polypectomy forceps were used; however, the IUD was too difficult to grasp using this method. Finally the IUD was removed with a curette (Fig. 2). Operative hysteroscopy was not available in the theater at that time. The commonly used thread retriever would not have helped in this case.

IUD after removal.
Discussion
IUDs are the most popular mode of contraception in China, used by >40% of women of reproductive age. 1 The stainless steel ring (SSR) or Gräfenberg's ring is the most commonly used IUD in China and has been available since the 1950s.
As more women are emigrating from China, gynecologists need to become familiar with the different types of Chinese IUDs. These are shown in Figure 3. The Chinese government decided to change over to copper IUDs in 1993, because of the comparative studies quoting higher failure and expulsion rates with SSRs. 2
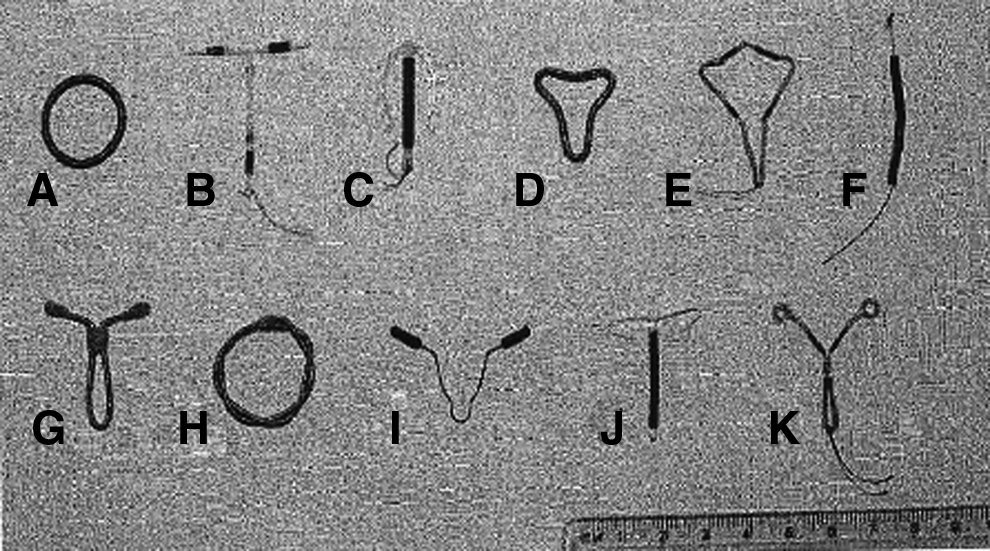
Types of intrauterine devices.
The SSR is a threadless IUD, which can be used as a permanent contraception, and became popular with the strict Chinese policy on limiting family size. Expulsion of the SSR has not been reported, however perforation rates are five per thousand insertions. The rigid steel device can stimulate contractile activity of the uterus, forcing it into the myometrium, which could lead to embedding and perforation if retained for longer periods.
The difficulties with removal of Chinese contraceptive devices have been discussed in detail in the study by Cheung. 3 His study describes his personal experience over 10-year period in removing IUDs. In his cohort of 491 women, 327 (66.6%) had their IUD inserted in China, 154 (31.4%) had it inserted in Canada, and 10 (2%) had it inserted in other countries. Successful removal of Chinese IUDs in the office was 72.3% in contrast to 95.8% for the IUDs that had been inserted in Canada (p<0.001). He reports use of an IUD removal hook to retrieve the IUD in the office.
The SSR accounted for the 63.4% of all IUDs removed in the study. The SSR is estimated to cost <25% of the price of the copper T IUD, hence its popularity in China. Copper IUDs that are commonly used now are the uterine-shaped IUD, gamma Cu380 IUD, MULTILOAD® Cu 375, and GyneFix®. These are shown in Figure 3. 3
The uterine-shaped IUD (D in Fig. 3) is designed in the shape of the uterine cavity with a stainless steel coiled wire framework similar to the SSR with copper added. 3 The gamma Cu380 IUD (G in Fig. 3) is made up of a gamma-shaped stainless steel wire frame with a copper wire in the middle layer. It also contains a silicone elastomer ring in the middle, and two side arms containing indomethacin. The Gynefix (F in Fig. 3) consists of six 5-mm-long copper sleeves threaded onto a monofilament polypropylene thread. The device is inserted into the myometrium of the uterine fundus with a special inserter, which anchors the knot at the end of the device to the uterus. 3
Conclusions
The main difficulties encountered in removing Chinese IUDs are absence of visible thread outside the cervix, unfamiliarity with the various types of IUDs, and postmenopausal status or nulliparity of the patient. Use of pre-procedural misoprostol may be beneficial. Because of the inert nature of the Chinese IUDs, indefinite retention of the IUD can be recommended in women in whom the office procedure has failed. 3
Footnotes
Disclosure Statement
No competing financial conflicts exist.