
Abstract
Abstract
Müllerian duct anomalies represent a heterogenous group of congenital malformations resulting from abnormal formation or incomplete fusion of Müllerian ducts. Most cases present at puberty or early adulthood with primary amenorrhea or fertility problems although many are asymptomatic and remain undiagnosed. The reported frequency of these anomalies varies, consequent mainly to the inaccuracy of diagnostic methods used and the lack of a uniform classification system. The actual reproductive impact of each anomaly continues to remain ill defined. In addition, radiologic and endoscopic advances appear to have increased the number of unnecessary surgical corrections for these defects. This article attempts to review the reproductive impact of various Müllerian anomalies in a simplified manner. (J GYNECOL SURG 28:127)
Introduction
Most cases present at puberty or adulthood, with either primary amenorrhea or infertility, but occasionally as urinary problems or pyocolpos in childhood. Patients with primary amenorrhea usually have obstructive pathology in one or both horns of the uterus, agenesis/stenosis of cervix, transverse vaginal septum or vaginal agenesis, provided functional ovaries and a responsive endometrium are present.
Infertility may result from anatomic copulatory problems or conception may simply not occur after a reasonable period of sexual cohabitation. The actual incidence of infertility in the various subcategories of Müllerian anomalies varies. This article attempts to highlight the fertility problems of women with MDAs.
Embryology and Etiology
The female and male reproductive systems develop from PMN and Wolffian ducts, respectively, both of which are present in the 6-week embryo. Although the two systems at this stage are morphologically identical with some cellular differences, the Wolffian duct is ahead of the Müllerian duct in development. 3 In the absence of testosterone, Wolffian ducts degenerate, whereas PMN ducts grow on both sides along lateral aspects of the developing gonads. This close development between PMN and Wolffian systems accounts for the frequent coexistence of Müllerian and renal tract developmental anomalies.
The funnel shaped cranial ends of the two PMN ducts open into the primitive peritoneal cavity and form the fimbria of the fallopian tubes. The horizontal parts form the remaining parts of fallopian tubes while the caudal regions fuse with the opposite structure, possibly in a caudocranial fashion, to form the uterus, cervix, and upper one third of vagina. However, anomalies such as a septate uterus, duplication of the cervix, and longitudinal vaginal septum tend to support a segmental and bidirectional fusion of PMN ducts.4,5 A Bcl-2 gene regulated apoptosis may play a role in regression of the intervening uterine septum. 6 The lining of the fused PMN duct gives rise to endometrium whereas the surrounding mesenchyma forms the endometrial stroma and myometrium by 22 weeks of intrauterine age.
Vaginal plate develops from fusion of the caudal ends of the mesodermal PMN ducts and the endodermal urogenital sinus, and becomes canalized by the 20th week of gestation. The surrounding mesenchyma gives rise to the fibromuscular vaginal wall. Not only is the extent of the contribution of the utero-vaginal primordium and urogenital sinus still a matter of debate, but the Wolffian ducts have also been suggested to have a role in formation of the vagina. 7
Various factors such as genetics, intra or extrauterine environment, and pharmacologic agents such as diethylstilbesterol (DES) and thalidomide have been implicated in the etiology of these anomalies. 8 Although autosomal dominant, autosomal recessive and X-linked disorders of MDAs are known, most familial cases are multifactorial.
Classification Systems
Various classification systems have been proposed for grouping the MDAs into different categories. Buttram and Gibbons proposed a classification combining the degree of developmental failure with clinical manifestations. 9
Toaff et al. categorized the anomaly of communicating uteri. 10
The current AFS classification (1988) categorizes MDAs into seven classes (Table 1).
Septate Uterus
This most common congenital uterine anomaly is the result of incomplete resorption of the partition between the two fused caudal parts of PMN ducts. The process of resorption normally begins caudally and proceeds cranially, thus a complete septum represents an earlier disturbance of this resorption than the incomplete form, and may often coexist with a longitudinal vaginal septum. 11 The incidence of both complete and partial septum is 33.6%, and it may be associated with renal or skeletal anomalies.12,13 A confirmation of diagnosis and its differentiation from bicornuate uterus should be done by evaluation of fundal contour by laparoscopy, MRI, or ultrasonography in hysterosalpingographically diagnosed cases, as the management of the two conditions is different. Figure 1 is the hysteroscopic view of a subseptate uterus. A persistent longitudinal septum partially dividing the uterine cavity with an intercornual angle of ≤75% on MRI suggests the presence of septate uterus.

Hysteroscopic view of a subseptate uterus.
The condition may not result in any reproductive problem and normal pregnancies may occur. However, a higher risk of miscarriage, preterm birth, and malpresentation may result. Buttram et al. suggested a 60% risk of spontaneous abortion, more so in the second trimester, whereas Woelfer reported a lower risk, which is more pronounced in the first trimester.9,14
The effect of uterine septum on conception is unclear. The condition is associated with a live birth rate of 58%. A significantly improved pregnancy outcome has been reported with hysteroscopic resection, in the form of reduction in miscarriage rates from 80 to 17% and an increase in live birth rates from 18 to 91%. 15 Two observational studies of 47 infertile women reported a 53.2% pregnancy rate after hysteroscopic septal resection, although no control group was included in these studies.15,16 This, in addition to the technical simplicity of the procedure supports management by surgical septal resection, particularly in cases with recurrent pregnancy losses and in those with otherwise unexplained infertility. However, a completely septate uterus with longitudinal vaginal septum may not be associated with infertility, and pregnancy in women with this condition may progress successfully without surgical treatment. Hence elective hysteroscopic incision of the complete septum in asymptomatic patients or before first pregnancy is not advocated. 11 Moreover, uterine rupture during the first pregnancy after prophylactic septal incision is a potential risk.
The poor pregnancy outcome is probably caused by implantation over the septum where a disruption of the orderly arranged blood vessels in the intermediate myometrial layer by the septum results in diminished vascular supply to the developing embryo. 17 Dabirashrafi et al. found septal implantation in 8 miscarried pregnancies out of the 12 women with septate uteri in his study. 18 The remaining 4 pregnancies that did not miscarry were on the lateral uterine wall, therefore suggesting that the pregnancies that miscarry are probably implanted on the septum. As women with this anomaly are at high risk for spontaneous mid-trimester pregnancy losses, prophylactic cerclage has been advocated in these women. 19
Arcuate Uterus
The uterus in this class VI (AFS classification) MDA bears a small (<1 cm) indentation at the fundus (Fig. 2). It was considered as a mild form of bicornuate uterus in the Buttram and Gibbons classification system. It is the most common uterine anomaly detected by the hysterosalpingography (HSG) wherein a saddle-shaped fundal indentation may be evident.,20,21 Aberrant vascularity of the fundal myometrium may sometimes be apparent. 20 It may also be regarded as subseptate uterus when the subseptum is very broad but short.

Laparoscopic view of an arcuate uterus.
Conflicting and limited literature on its diagnosis and reproductive impact compounds the management difficulties of arcuate uterus. Acien and various other authors reported the poorest survival rates and the highest miscarriage rates with this anomaly, in sharp contrast to Francisco et al., who found 80% term delivery and 82.7% live birth rate and no impact on reproductive and obstetric outcome.19,22 However, the study by Acien is vague about the difference between arcuate and septate uterus, thus making interpretation of results difficult. Lin reviewed the reproductive outcome in women with uterine anomalies after both natural conceptions and assisted reproduction and concluded that an arcuate uterus has a similar reproductive outcome to normal uteri. 23 The management of arcuate uterus is similar to that of septate uterus; however, only women with poor past reproductive performance warrant a surgical correction.
Unicornuate Uterus
Unicornuate uterus, a class-II anomaly of the AFS classification system, occurs in 6.3% of women and is accompanied by ipsilateral renal and ureter agenesis in 67% and pelvic kidney in 15%. 24 The anatomic variation is large and the unicornuate uterus may or may not have a rudimentary horn, which in turn may or may not communicate with the main uterine cavity. The rudimentary horn, when present, is difficult to diagnose and is often found by accident. This anomaly was earlier classified as an asymmetric lateral fusion defect. Figure 3 is a laparoscopic view of a unicornuate uterus with absent contralateral horn, tube, and ovary.

Laparoscopic view of a unicornuate uterus and absent contralateral uterine horn, Fallopian tube, as well as ovary.
The reproductive outcomes of the unicornuate uteri appear to be the poorest among all MDAs, although normal pregnancies can occur. Most obstetric complications occur in the first 20 weeks and can result in miscarriage, uterine rupture, or maternal death (0.5%).25–27 The anomaly has a significantly poor reproductive outcome secondary to abnormal uterine vasculature and reduced muscle mass. Analysis of 393 pregnancies by Lin revealed that the condition is associated with a tubal pregnancy rate of 4.3%, pregnancies in the rudimentary horn in 2% of conceptions, a high miscarriage rate of 34.4%, a preterm delivery rate of 43.3%, and a live birth rate of 54.2%. 23 The abnormal uterine vasculature, a relatively more receptive blood supply for the embryo in the tube and greater chance of sperm/ovum migration to the opposite side may account for the higher ectopic pregnancy rates. Transmigration of one or both gametes may also result in implantation of pregnancy in the rudimentary remnant, which eventually ruptures in late first or second trimester, posing diagnostic difficulties. 5 For this reason, the rudimentary horn should be excised prior to pregnancy as a preventive measure, usually by laparoscopic hemihysterectomy. 23 However, surgical treatment is not indicated when the rudimentary horn lacks an endometrium. 25 The cervix of an anatomically anomalous uterus and of a unicornuate uterus in particular has been considered to have a role in the difficulty in maintaining a viable pregnancy. Roddick et al. proposed a higher ratio of muscle fibers to connective tissue in the cervices as a cause of its tensile weakness. 28 The asymmetric downward force exerted by the anomalous and markedly increased pressure during pregnancy adds to the existent predisposition, thus prompting some clinicians to advocate prophylactic cerclage in women with this condition. 29 Abramovici et al. reported a decline in the spontaneous abortion rate from 88% to 0 and an increase in term deilvery rate from 0 to 87% after this procedure. 30 Although several studies have advocated prophylactic cervical cerclage in pregnancy, none have been randomized and nearly all have lacked controls. Blum found that half of his study population of second trimester losses with uterine anomalies had significantly diminished levels of serum cystine aminopeptidase, an enzyme that neutralizes oxytocin. 31 Malpresentation, often consequent upon the paucity of intrauterine space, coupled with the irregular uterine contractility in labor, may account for the increased abdominal deliveries reported in women with this condition.
Uterus Didelphys
Didelphic uteri account for 6%–11% of all uterine malformations and are the result of completely or partially arrested midline fusion of PMN ducts. 32 Apart from the duplication of uterus and/or cervix, the vagina too may have a complete (in 75% cases) or partial longitudinal septum. A syndrome of obstructed hemivagina and ipsilateral renal anomaly (OHVIRA), first reported in 1922, includes duplicated uterus as the concomitant uterine anomaly. 33 Bladder exstrophy with or without vaginal hypoplasia, congenital vesicovaginal fistula with hypoplastic kidney, and cervical agenesis may be associated with didelphic uterus.32,34,35
The literature on the reproductive impact of this condition is limited by the low number of subjects. The condition is reportedly associated with an ectopic pregnancy rate of 2.3%, a miscarriage (particularly second trimester miscarriage) rate of 20.9%, a preterm delivery rate of 24.4%, and a live birth rate of 68.6%.12,36 The presence of an associated vaginal septum may have no impact on fertility but may occasionally result in dyspareunia or vaginal discharge. In the presence of a longitudinal vaginal septum, coitus and hence simultaneous pregnancy can occur in each uterus with the resultant twins being invariably dizygotic. Delivery of the second twin 3 hours to 8 weeks after the delivery of first twin has led clinicians to believe in each pregnancy being a separate entity, with lactation beginning after the arrival of the second twin.37,38 Advocates of both vaginal and cesarean deliveries have found favor in this situation. In the report by Nohara et al., the first twin was delivered abdominally at 25 weeks' gestation whereas the second twin was delivered vaginally at 35 weeks without any adverse maternal or neonatal outcome. 38 Figure 4 shows a didelphic uterus after the second cesarean section, the smaller horn having the cesarean scar of previous delivery. Unilateral placental abruption and unilateral preterm labor are also documented in this condition.38,39 Consequent upon more frequent association of cervical dystocia and malpresentations in women with didelphic uteri, the incidence of cesarean section is higher. However, vaginal dystocia during labor caused solely by a vaginal septum has not been reported. The frequent association of endometriosis resultant from retrograde menstruation from complete unilateral outflow obstruction may also adversely affect fertility. In the event of coexistent pregnancy and an obstructed contralateral vagina, vaginal septal resection is indicated. Women with didelphic uterus and a long history of recurrent spontaneous miscarriages or preterm births may benefit from Strassman metroplasty, although it is not uniformly recommended, and the results may often be disappointing. In addition, cervical unification is technically difficult and carries the risk of cervical stenosis or incompetence. 40

Operative view of a didelphic uterus after cesarean section on the larger horn. The smaller horn had the scar of a previous cesarean delivery.
Bicornuate Uterus
Bicornuate uterus results from incomplete fusion of the Müllerian ducts at the level of the uterine fundus while the lower uterus and cervix are completely fused and unified. This results in two separate but communicating endometrial cavities with a single cervix and vagina. A muscular intrauterine septum corresponds to an indentation of at least 1 cm depth at the external fundus. 41 Complete extension of the septum to the level of internal os and external os results in formation of bicornuate unicollis and bicornuate bicollis uteri, respectively. The septum is limited to the fundal region in the partial variety. Bicornuate uterus may also be an uncommon component of a mild variant of the urorectal septum malformation. 42
Women with this anomaly may not have any reproductive problem and the diagnosis may be made incidentally. Conception is usually not an issue, although the resultant pregnancies may be complicated by spontaneous miscarriage (66%) and preterm birth. 43 A twin pregnancy in one horn of the bicornuate uterus, which terminated spontaneously at 22 weeks, has been reported by Narlawar et al. 44 Figure 5 is an ultrasonic picture of a 20-week twin pregnancy, with one twin in each horn of a bicornuate uterus. A study on 56 bicornuate pregnancies reported the incidence of preterm deliveries, live births, spontaneous miscarriages, and ectopic pregnancies to be 25%, 63%, 25%, and 0%, respectively. 23 However, the study did not elaborate on the reproductive performance of the subcategories of bicornuate uteri. Raga et al. evaluated the reproductive performance of 26 women with this anomaly and reported a term pregnancy rate of >60%, with a take-home baby rate of 62.5%. 43 Poorest reproductive prognosis has been occasionally reported with partial rather than complete defects. 22
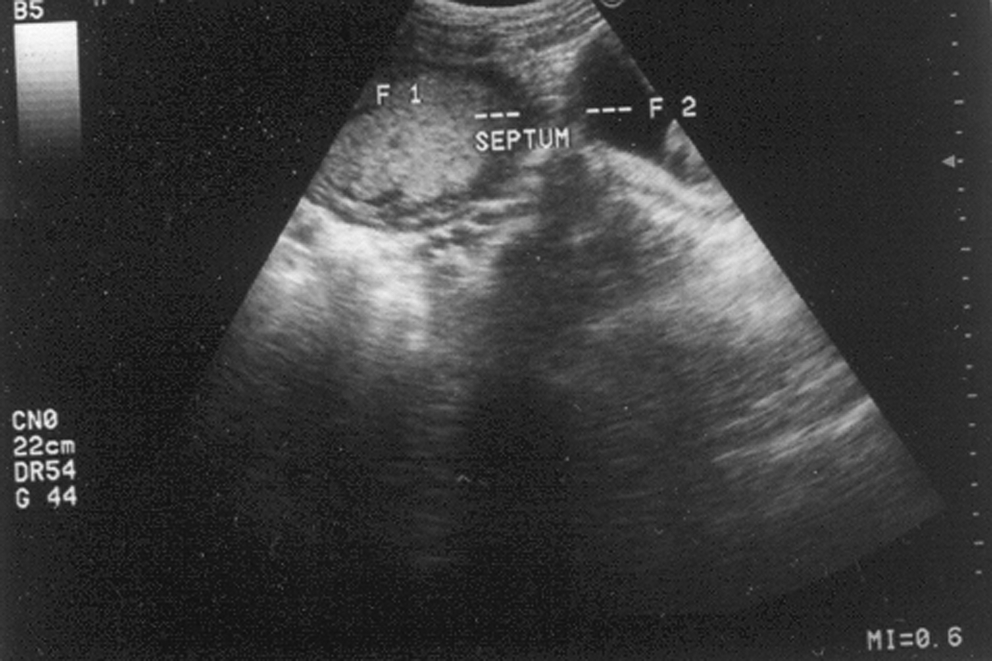
Ultrasonic picture showing 20-week twin pregnancy, one twin in each horn of a bicornuate uterus.
MRI scores over ultrasonography and HSG in distinguishing bicornuate from septate uterus. This distinction is important as the bicornuate uterus is associated with few reproductive problems and rarely needs surgical management, in contrast to septate uterus. Detection of two uterine bodies and a single common cervix, with an intercornual distance of >1050 on MRI is characteristic of a bicornuate uterus. 45 Moreover, an outwardly concave external contour suggests a bicornuate uterus, as against the outward convexity of normal or septate uteri. 46 HSG is only 55% accurate in differentiating these two anomalies. 47 Laparoscopic evaluation of the fundus is the definitive distinction modality.
Metroplasty is rarely indicated in bicornuate uterus and should be reserved for women with repeated spontaneous miscarriages (particularly mid-trimester miscarriages) and preterm birth, with no other evident etiology. 27 Prophylactic cerclage has also been suggested to have a role in management of these women as an attempt to prevent mid-trimester pregnancy losses. 19
Cervical Atresia
Atresia of the uterine cervix is a rare anomaly in women with Müllerian agenesis and is associated with vaginal aplasia in 50% of cases. 48 These patients usually present as adolescents with cyclical intense abdominal pain and primary amenorrhea. The condition has conventionally been managed by laparotomy and restoration of uterovaginal continuity by using foreign bodies such as Foley's cather, T-tubes and intrauterine contraceptive devices (IUCDs) for a few months to maintain patency. However, cervical stenosis and later occlusion are common long-term sequelae. Darai et al. described a successful laparoscopic-assisted uterovaginal anastomosis for cervical atresia concurrent with partial vaginal aplasia. 49
T-Shaped Uterus
T-shape of the uterus has been associated with in-utero exposure to DES, a drug banned since 1971. As a result, its occurrence and clinical significance is decreasing as most affected women have by now passed their reproductive years. The presence of a T-shaped uterus is associated with a ninefold increase in ectopic gestation and a twofold increase in miscarriage and preterm delivery rates, in comparison to a matched control population. 50 The antiestrogenic effect of the drug on the endometrium may additionally have a contributory role in the adverse obstetric outcome seen in this condition. However, infertility has not been reported in women with this condition.
Uterine Anomalies and Assisted Reproduction
Very few studies are available that look at the assisted reproductive technology (ART) outcome in various uterine anomalies. Lavergne et al. studied 38 women undergoing 119 oocyte retrievals and compared the reproductive outcome with a French national database of 7677 in vitro fertilization (IVF) oocyte retrievals over the same period. 51 They reported 11.7% pregnancy rates per retrieval, 13.6% pregnancy rate per transfer, and 5.8% implantation rate (pregnancy rate per embryo) for the studied group, all rates being lower than those in the national database. Untreated septate, unicornuate, and bicornuate uteri had a 50% reduction in pregnancy rate per transfer and implantation. Heinomen et al. compared IVF rates of 17 subjects with uterine anomalies (55 IVF cycles) with a historic database from the same hospital (8.2% versus 17.5%–19%) and found a lower delivery rate per embryo transfer in women with unicornuate and didelphic uteri. 52 However, the small number of cases is a serious limitation to the interpretation and significance of this study. Marcus et al. looked at 24 women with uterine anomalies who underwent 47 IVF cycles and found implantation rates of 27.3%, 22.5%, 11.6%, and 13.2% in didelphic, septate, bicornuate, and unicornuate uteri, repectively. 53
Vaginal Septum
A vaginal septum, one of the most common congenital malformations of the female genital tract, may be transverse or longitudinal. Both types of septae may be complete or partial. A transverse vaginal septum is the result of faulty vaginal canalization that may, at times, be a consequence of in utero DES exposure. As a result of its embryonic origin, the transverse septum is usually located at the junction of upper one third and lower two thirds of the vagina, although it can occur at any level. It may be discovered incidentally on routine gynecologic examination or may present with dyspareunia. A lower pregnancy rate and more extensive endometriosis is seen with a high transverse septum, suggesting early onset of retrograde menstrual flow as an etiological factor. Rock and Zacur reported 26 cases of transverse vaginal septum with associated urinary tract anomalies, coarctation of the aorta, atrial septal defect, and anomalies of lumbar spine. 54 Improper lateral fusion of the distal ends of PMN ducts results in a longitudinal septum that may again be partial or complete. It is usually located in the lower vagina and may coexist with a bicornuate uterus with one or two cervices. Haddad et al. reviewed 202 cases and described a complete longitudinal septum (from cervix to introitus) in 45.6% women, a high partial one in 36.15% and medium or low partial onein 18.3%. 55 Uterine anomalies coexist in 99.4% of complete/partial high septa and in 30.3% of partial medium or low septa, septate uterus being the most common associated uterine anomaly. Septal thickness varies and a fibrous septum is commonly lined with vaginal epithelium, but occasionally may be encircled by a muscular layer to form a double vagina. In cases of didelphic uterus with a longitudinal vaginal septum, one uterine hemicorpus is usually better developed than the other. If intercourse consistently occurs on the vaginal side connected to the hypoplastic uterine hemicorpus, infertility and miscarriages can result. Figure 6 shows a complete longitudinal vaginal septum, on one side of which opened the cervix of a bicornuate uterus while the opposite side was blind but roomy. The woman presented with primary infertility of 12 years' duration, and coitus was being practiced in the blind vaginal side. A simple excision of the septum resulted in conception within 3 months. Ultrasound is the most sensitive imaging modality for vaginal septa. However, clinical examination is more sensitive, accurate and practical, hence imaging may be used in cases of obstruction of the upper vagina or uterus. MRI can, in addition, differentiate the type of collected fluid above the vaginal septum.

A complete longitudinal vaginal septum, on one side of which opened the cervix of a bicornuate uterus while the opposite side was blind but roomy.
Asymptomatic longitudinal septa do not warrant division in all cases and excision may be limited to those patients with dyspareunia, copulatory problems, or obstruction to drainage from one vaginal half.
Conclusions
Variations in the mode and timing of presentation as well as diagnostic pitfalls make the Müllerian anomalies more complex to manage. MRI may have a role in differentiating bicornuate from septate uteri. Arcuate uterus is the most common anomaly and has a reproductive outcome comparable to that of normal uteri. Septal resection in cases of septate uteri may help to improve outcome in women with recurrent pregnancy loss and in those with otherwise unexplained infertility. However, its distinction from bicornuate uterus is essential prior to surgery, as most bicornuate uteri will not require surgery. Bicornuate uteri may not cause any reproductive problem and surgical correction should be limited to women with recurrent pregnancy losses. Unicornuate uterus has the poorest reproductive prognosis among the MDAs. Presence of functional endometrium in rudimentary horn in association with unicornuate uterus usually warrants excision of the rudimentary remnant prior to pregnancy. Although uterus didelphys is also associated with poor reproductive outcome, results of metroplasty are unsatisfactory, and the procedure should only be considered in women with a long history of recurrent spontaneous miscarriages or preterm births.
Footnotes
Disclosure Statement
No competing financial conflicts exist.