
Abstract
Abstract
Introduction
Case
A 25-year-old woman presented with a backache and vague abdominal pain of 1 month's duration. She was uniparous, had had a full-term cesarean delivery 4 years earlier, and had breastfed the infant for 16 months. Her present menstrual cycles were regular (once in 28 days with a 5-day menstrual flow). Her last menstrual period occurred on December 12, 2010. Results of a physical examination revealed a right adnexal mass, ∼10×15 cm, palpated separately from the uterus with no other organomegaly. An earlier computed tomography (CT) scan (on December 11, 2010) showed a mass in the pelvis with solid components of 14×9×10 cm of right ovarian origin, a right adrenal lesion, and a well-defined lesion 3×3 cm in the anterior pole of the spleen. A positron emission tomographic (PET) scan (December 18, 2010) showed metabolically active lesions in the lower abdomen (13.7×8.5×10.5cm), right adrenal gland (5.5×5.5cm), and spleen (3×3.9 cm). Tumor markers, namely α-fetoprotein, CA-125, and lactate dehydrogenase (LDH), were within normal limits, whereas her β–human chorionic gonadotropin (βHCG) level was raised with a value of 8120 mIU/mL. Esophagogastroduodenoscopy, colonoscopy, and chest radiography testing all yielded normal results.
The patient underwent a laparotomy (on December 23, 2010) with excision of a right ovarian mass. A frozen section of the right ovarian mass (nodular mass of 14×9×5cm; Fig. 1) revealed large multinucleated syncytial cells, intermingled with clusters of polygonal cells resembling cytotrophoblasts, and large areas of hemorrhage and necrosis. The pathology was consistent with chorocarcinoma. Infracolic omentectomy, a partial splenectomy (Fig. 2) by use of radiofrequency ablation, and a right adrenalectomy (Fig. 3) with diagnostic endometrial curettage were performed. Her uterus, left ovary, and tubes were grossly normal and were left in situ. Final histopathology confirmed a diagnosis of choriocarcinoma of the right ovary (Fig. 4), with a part of the spleen measuring 6×5×2.5 cm and a tumor size of 3×2×2 cm, and a right adrenal gland measuring 6×3.5×3 cm, both of the latter two confirming tumor metastasis. The omentum showed no tumor deposits, and endometrial tissue that was currattaged showed only proliferative changes, without evidence of any malignancy. Fluid cytology was negative for malignancy. Based on all the abovementioned findings, a final diagnosis of nongestational ovarian choriocarcinoma, with metastases to the splenic parenchyma and right adrenal gland, was made.

Resected specimen of right ovarian tumor.
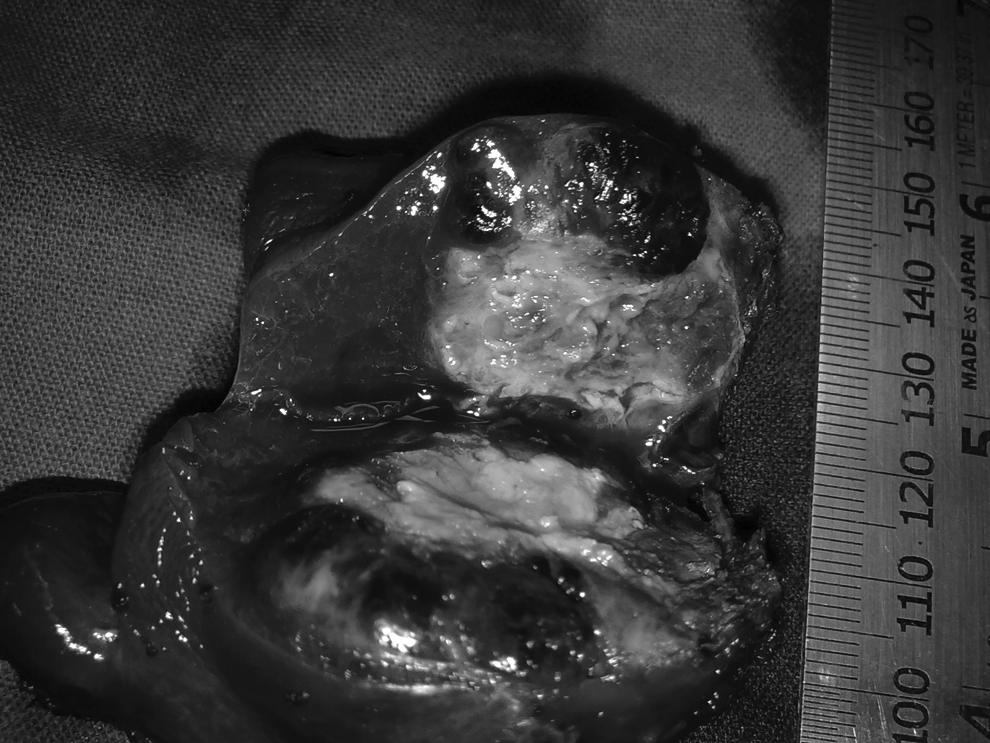
Cut section of partial splentomy showing the parenchymal metastases.
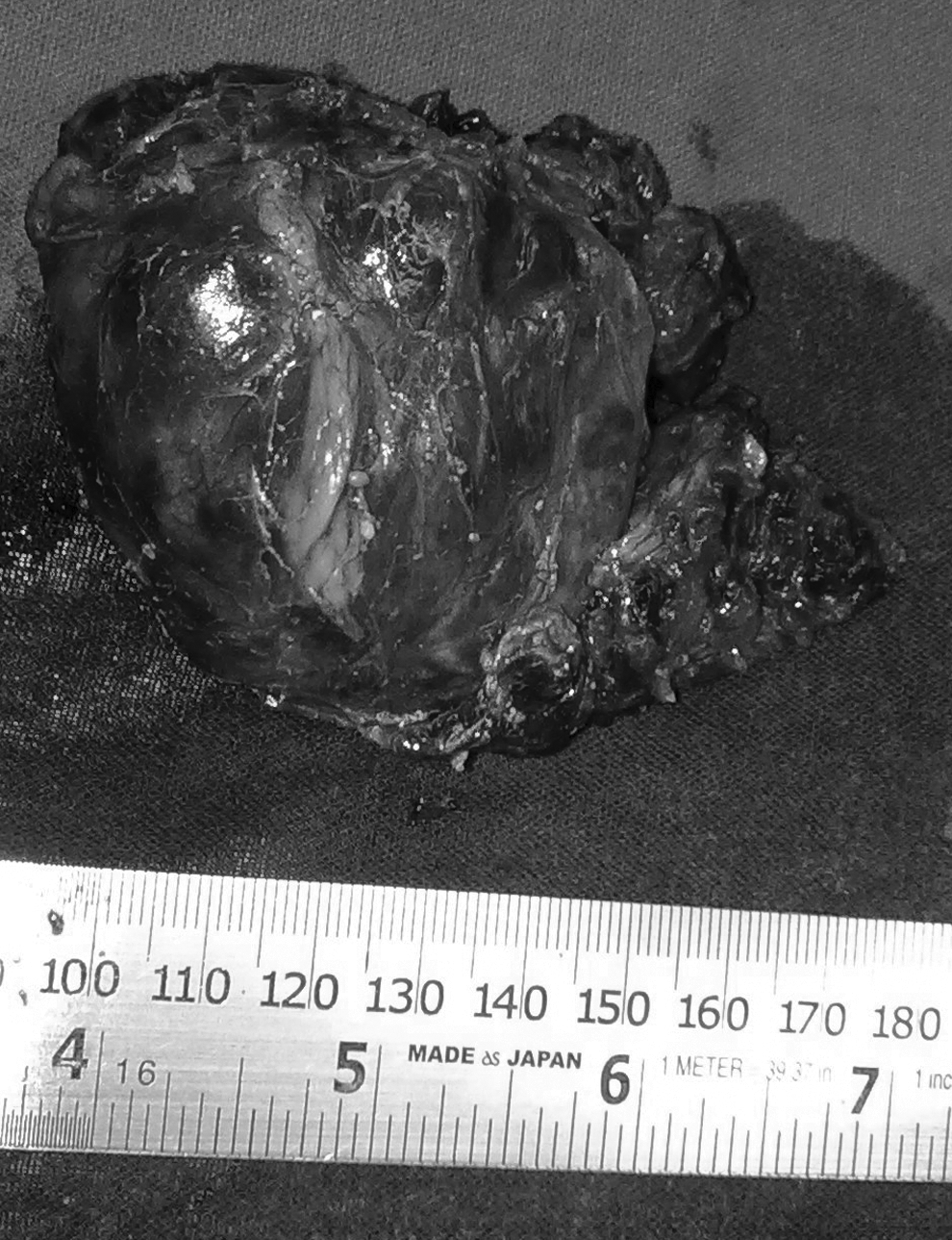
Gross specimen of right adrenal gland.
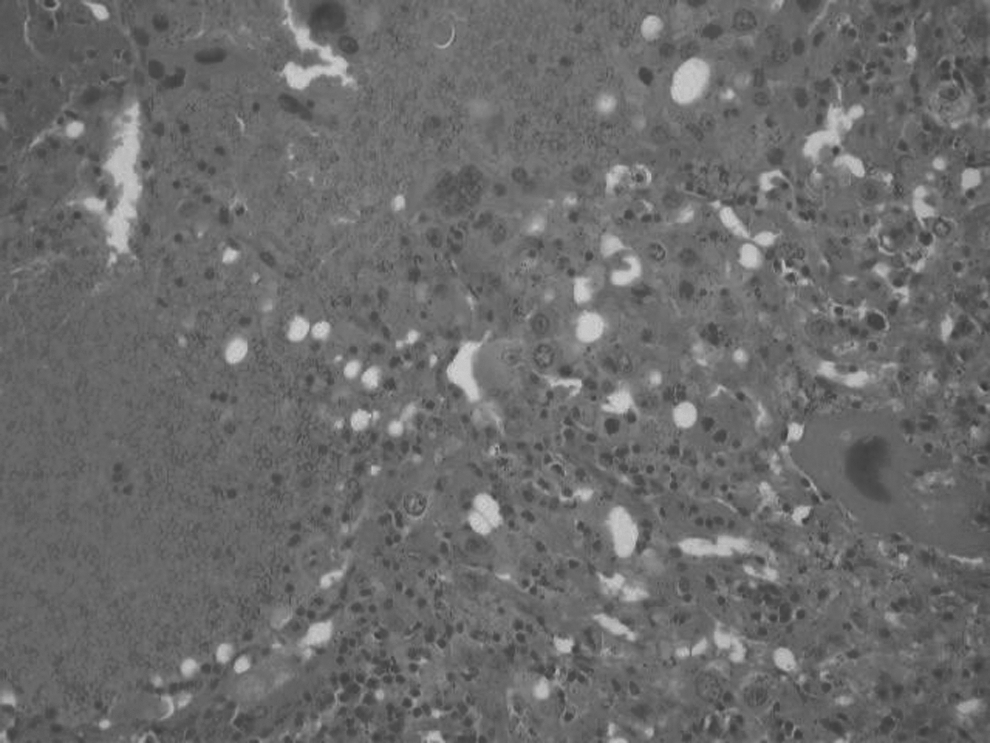
Microscopic picture of right ovary, confirming diagnosis of choriocarcinoma. with multinucleated syncytiotrophoblast and areas of hemorrhage.
Results
The patient's β-HCG decreased to 913.63 mIU/mL within 1 week postoperatively. she was started on adjuvant chemotherapy, with a regimen of bleomycin, etoposide, and cisplatinum (BEP) and has so far received three cycles of the same agents and four cycles of etoposide and cisplatinum (EP). Bleomycin was removed from the regimen (to prevent pulmonary toxicity), as the patient had already received 240 mg. Her β-HCG normalized to a value of 4.1 mIU/mL. She also received two cycles of prophylactic chemotherapy subsequently, and was in complete remission 5 months from the date of surgery.
Discussion
Gestational choriocarcinoma is known to have a good prognosis. However, nongestational choriocarcinoma has a poor prognosis and, hence, requires more aggressive therapy (combined therapy) in the form of chemotherapy with surgery. 6 It is important to distinguish between gestational and nongestational choriocarcinoma for this reason. Diagnosis of nongestational choriocarcinoma is made by exclusion of disease in the uterine cavity and absence of a molar or intrauterine pregnancy, and pathologic confirmation of the disease. 7 Also, the presence of paternal DNA in the tumor can be used to distinguish gestational from nongestational choriocarcinoma. 6
It is probably justified to call this case “pure primary nongestational ovarian choriocarcinoma” because of the absence of disease in the currettaged material from the uterus, the low levels of β-HCG, and the presence of pure type shown via histopathology of the right ovary. DNA analysis was not performed, as the facilities to do this were not available.
As the patient was young and wished for fertility-sparing treatment (she expressed this desire during preoperative counseling), and as the uterus and left adnexa were grossly normal, a fertility-sparing treatment was performed by preserving the uterus and nondiseased adnexa. There are earlier reports of fertility-sparing treatment in pure nongestational ovarian choriocarcinoma. 8
In this case, as a part of complete cytoreduction, infracolic omentectomy, partial splenectomy (metastatectomy), and right adrenalectomy were performed. Metastatic disease as seen on the PET scan was completely excised for aggressive management of the disease. Partial splenectomy was performed, with an idea of preserving immunologic function of the spleen, 9 in view of young age of the patient, by using a radiofrequency probe to make the line of division bloodless. Solitary splenic metastases from female genital tract malignancies are rare. 4
Metastases to the adrenal glands from ovarian malignancies are very rare; there is only 1 case reported of metastasis to the adrenal gland from ovarian choriocarcinoma reported in a 30-year experience of 464 adrenal metastases. 5 Survival is better with an aggressive surgical approach involving removal of metastases, compared with an approach not involving surgery. 5 For completion of cytoreductive surgery, a right adrenalectomy was performed in the present case. This case had concurrent parenchymal metastases to the spleen and right adrenal gland from a right ovarian choriocarcinoma, which has never been reported; this might be the first case reported.
Conclusions
Aggressive surgical treatment combined with multiagent chemotherapy is likely to produce a good outcome. This patient received two cycles of chemotherapy and continues to receive the same, as the number of cycles required might be as many as 10. 6
Footnotes
Acknowledgments
The authors contributed to this article as follows: Drs. Ramarajapalli and Rao contributed information on the surgery; Dr. Prathima contributed information on pathology; Drs. Ramarajapalli, Rao, and Killara contributed information on patient care; and all authors contributed to the writing of the article.
Disclosure Statement
No competing financial conflicts exist.