
Abstract
Abstract
Introduction
In some cases, during penetration, small fragments, most consisting of cortex only, separate and form accessory adrenal structures. Ectopic adrenal tissue has been identified in multiple sites such as the liver, kidney, pancreas, transverse colon,celiac plexus area, broad ligament, ovary, testis, and epididymis, as well as retroperitoneally along the course of the vessels of gonads.3–6 The most common location of adrenal rests are within the testes or along the spermatic cord. Some authors estimated that these rests may be present in 50% of newborns, but most of them become atrophic by adulthood.1,7
Granulosa cell tumors, which secrete estrogen, are seen in women of all ages. They are found in prepubertal girls in 5% of cases; the remainder are found in women throughout their reproductive and postmenopausal years. They can be seen bilaterally in only 2% of patients. In the prepubertal population, a granulosa cell tumor is associated with 75% of sexual pseudoprecocity because of the estrogen secretion. Through reproductive age, most patients have menstrual irregularities or secondary amenorrhea, and cystic hyperplasia of the endometrium. 8
A rare case of ectopic adrenal tissue at the adnexal region, contralateral to a malignant granulosa cell tumor of the ovary, is reported.
Case
A 50-year-old patient, gravida 4, para 2, was admitted to the gynecology clinic having had menorrhagia, dyspareunia, and abdominal distention for 12 months. She also had had type 2 diabetes and hypertension for ∼5 years. Her physical examination demonstrated mild tenderness and fullness on the right adnexa. Her pelvic Doppler ultrasound imaging showed a mass measuring 144×19×93 mm containing cystic and solid regions with low resistance blood flow. She had serum CA-125: 29.3 international units (IU)/mL, follicle-stimulating hormone (FSH): 0.006 mIU/mL, luteinizing hormone (LH):1.37 mIU/mL, and estradiol (E2):64 pg/mL. After consolidating her systemic conditions,, she was prepared for surgery. Initially she had a diagnostic laparoscopy. After the diagnosis of bilobulated fragile and irregular surface mass and diameter of 15 cm in the right adnexa, a right salpingo-oophorectomy was performed by laparotomy. The material was sent for frozen section and the result was malignant stromal tumor. Hysterectomy, left salpingo-oophorectomy, and bilateral pelvic and para-aortic lymphadenectomy were performed in sequence. The patient was discharged from the hospital after her seventh postoperative day. The pathologic report showed a granulosa cell tumor in the right ovary, and ectopic adrenal cortical tissue surrounded by adipose tissue on the left ovary. Peritoneal cytology was tumor negative. The left ovary and fatty tissue specimen were stained with hematoxylin-eosin (HE). (Figs. 1 and 2)
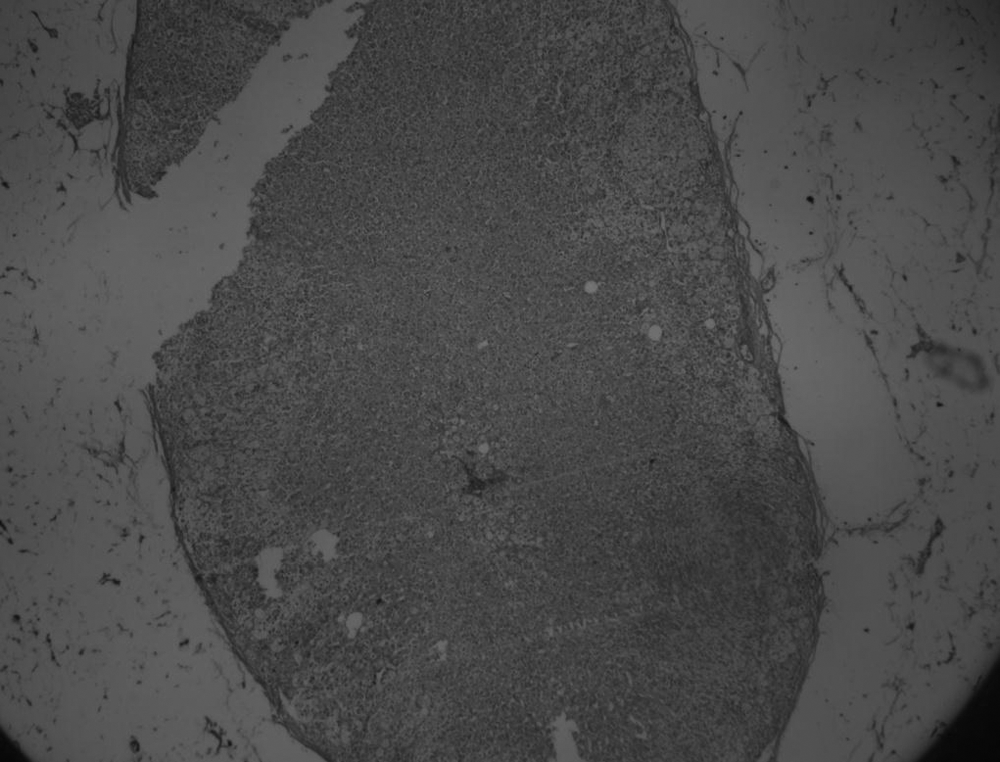
The capsule and three zones of ectopic adrenal tissue surrounded by adipose tissue. (hematoxylin-eosin [HE]×4).

Ectopic adrenal tissue with zona fasciculata and reticularis (hematoxylin-eosin [HE]×20).
Discussion
With intense examination, accessory adrenal tissue may be found in at least 50% of neonates and infants. This accessory adrenal tissue atrophies with advancing age as it becomes physiologically unnecessary in the presence of normal adrenal glands.3,6
The most common region for the ectopic adrenal tissue is the spermatic cord, and it is incidentally seen during surgical procedures such as herniotomy or orchiopexy in the inguinoscrotal region.9–11
Ectopic adrenal tissue is rarer in the adult female population. Ectopic adrenal tissue was found in the wall of an ovarian serous cystadenoma by Usta et al. and in the right uterine adnexa by Kim et al.3,12
Rarely, ectopic adrenal tissue can become clinically significant. Adrenocorticotropic hormone (ACTH)-independent Cushing's syndrome can occur with adrenal hyperplasia or ectopic adrenocortical adenoma presenting with faciotruncal obesity, facial erythrosis, easy bruising, striae, hypertension, and amenorrhea. 7 In this patient, these findings, other than chronic hypertension, were not observed. The probability of neoplasia or hyperplasia is low in ectopic adrenal tissues. 13
The germ and adrenal gland cells migrate together during the embryologic period. It can be postulatd that the granulosa cell tumor may originate via this migration theory. In women with granulosa cell tumors who do not want children, bilateral excision of the ovaries is suggested, even if the contralateral ovaries appear normal.
Conclusions
Ectopic adrenal tissue is relatively rare in the adult female genital tract. It can be seen during surgery incidentally but occasionally may be clinically significant as mentioned previously. Surgeons should be aware of this uncommon entity.
Footnotes
Disclosure Statement
No competing financial conflicts exist.