
Abstract
Abstract
Introduction
Case
This infant was born prematurely by emergency cesarean section at 24 week's gestation because of early membrane rupture, weighing 445 g (extremely low birth weight), after a gestation that was characterized by a threat of miscarriage. The infant's Apgar score was 8–9. Her length was 31 cm and her cranial circumference was 20 cm. At birth, she had valid cardiac activity and some breathing activity. Respiratory assistance was started with CPAP and was continued for 5 days, but, because of her respiratory insufficiency, mechanical ventilation was necessary (34 days, followed by CPAP for another 10 days). Severe bronchodisplasia required corticoid administration for a period of 2 months, and she needed parenteral nutrition for a long period of time. A neonatal abdominopelvic ultrasound (US) scan at the age of 3 months, showed a cystic anechoic mass with septa measuring 3.5×3.4×2.5 cm, probably of ovarian origin (in the right annex).
Additional US scans confirmed the persistence of this ovarian cyst with an increasing diameter of 5.6×4×3.6 cm at the last scans performed at the end of the patient's fourth month of life (Fig. 1).
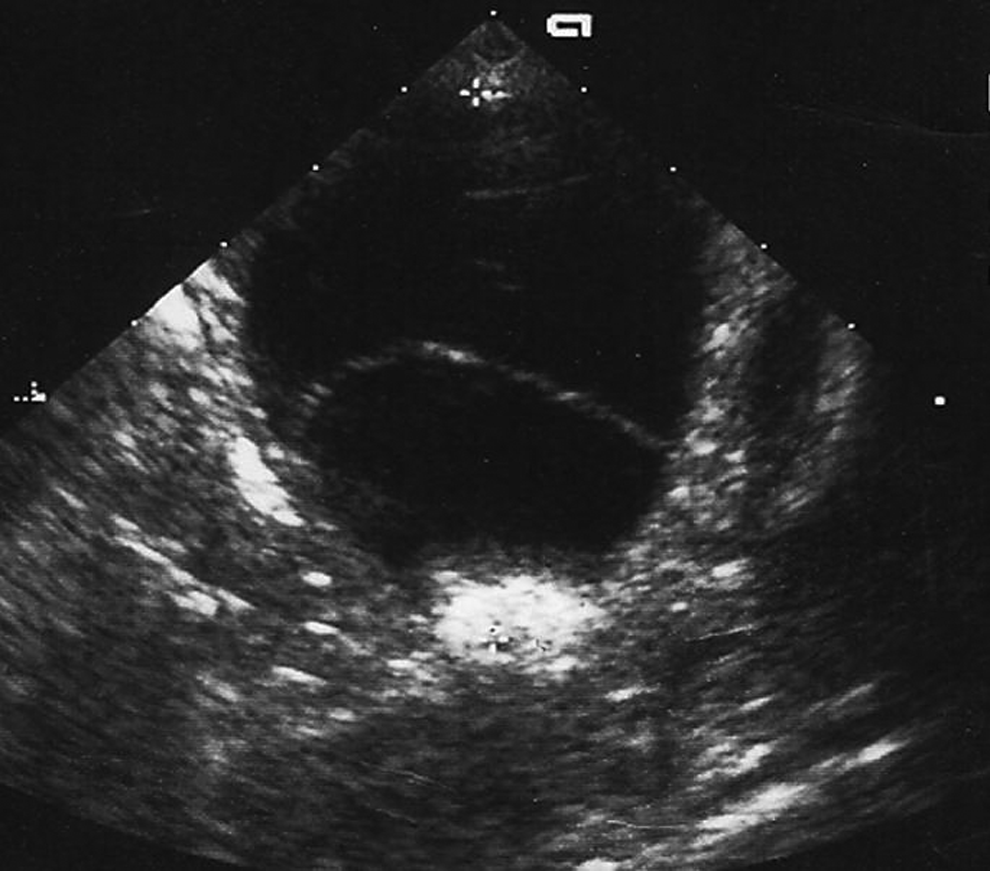
Cystic anechoic mass with septa of ovarian origin (right ovary) of 5.6×4×3.6 cm.
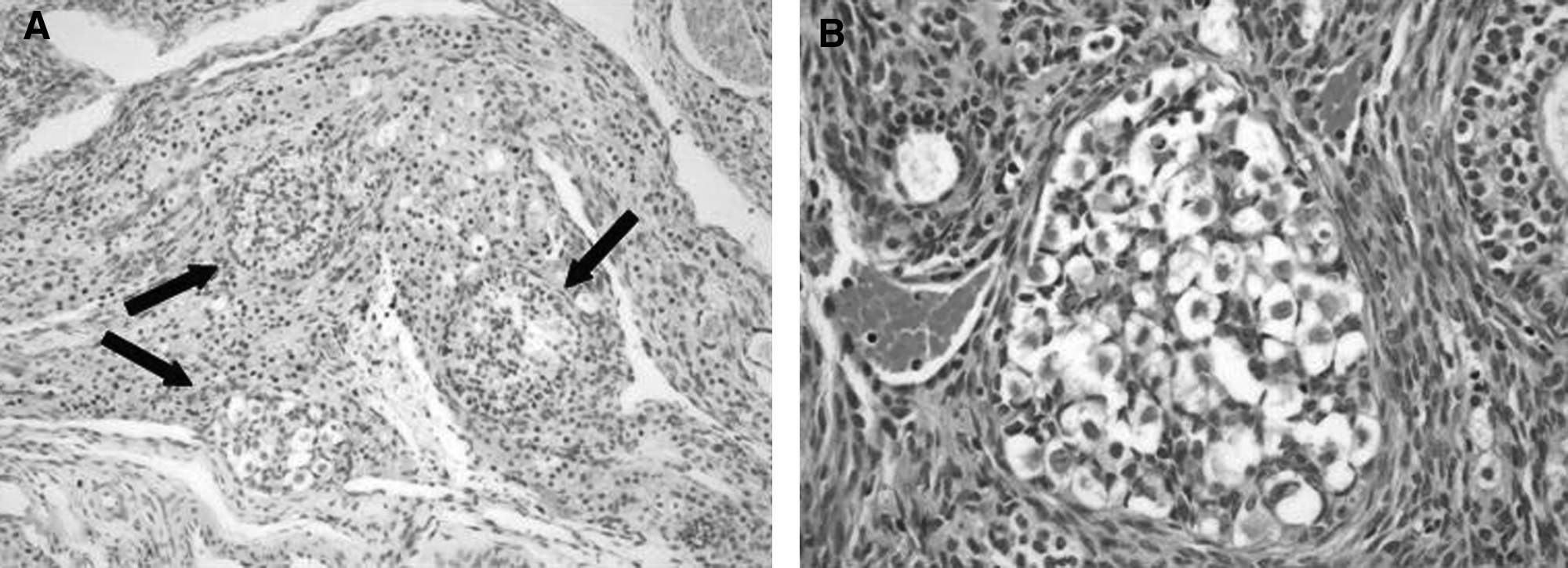
During laparotomy, which was performed when the patient was 5 months' old, a large left-sided ovarian cyst was found, 5.5–6 cm in diameter with a macroscopic follicular aspect and wall differentiated from the normal ovarian tissue. However the cyst, with the ovary, was exteriorized from the surgical incision and was aspirated to reduce its volume, thereby preventing inadvertent spillage of cyst fluid into the peritoneal cavity. Fifteen milliliters of citrine fluid were aspirated. A left ovarian cystectomy was performed. The right ovary and Fallopian tube were normal. There were no postoperative complications and the patient was discharged 3 days later. On histologic examination, the ovarian mass was found to be a simple follicular cyst with a coexisting gonadoblastoma in miniature (Fig. 2).
She was readmitted to the hospital and was studied. Her serum tumor markers (αFP; CEA, βHCG, and CA125) were evaluated during this hospitalization and the results were negative. The karyotype of the patient was a normal female chromosome pattern of 46 XX. The abdominopelvic RM for tumor staging was normal. The patient was followed up again at 1 month. Her left ovary appeared greyish and was 2×0.8 cm in size, with several small cysts of 2–3 mm. Her Fallopian tube was normal aspect. A left salpingo-oophorectomy and a biopsies of the contralateral ovary (cortical and medullar) were performed. There were no signs of abnormal iliac and aortocaval nodes, and there were no alterations of her omentum noted on examination and palpation. There was no ascites for cytology to assess.
Results
The patient started eating the day after, and she was was discharged the following day. Histopathology showed a normal left ovary and a normal right ovary, without any neoplastic residual tumor in the left ovary. This patient is now 9 years old; she has grown up normally. Pelvic US shows that she has a normal right ovary.
Discussion
Ovarian masses in children are an uncommon occurrence. Childhood ovarian masses represent a heterogeneous group of lesions with many etiologies. It has been reported that up to 64% of these masses are neoplastic. 2 Primary ovarian tumours are the second most common tumors seen in women over age 35. The incidence of benign and malignant neoplasms is around 2.6 cases per 100,000 in girls younger than 15. These tumors represent < 2% of all malignancies in girls under 16, and are primarily are germinal tumors (60%). 3 Malignant ovarian tumors in children and adolescents are rare (∼ 0,9% of all malignancies), 4 with 10% being tumors of the stroma ovary, while superficial epithelial tumors account for < 15%–20% of ovarian neoplasms. A minimum percentage (∼ 10%) of neoplasms include sarcomas, lymphomas, and other rare forms of growths.
Cystic lesions of the ovary are most common during infancy and adolescence, as they are in newborn infants. The incidence of antenatally diagnosed, clinically significant ovarian cysts is ∼ 1 in 2500 live births. Ovarian cysts are the rule—not the exception—in newborn infants. At birth, up to 98% of newborn girls have small ovarian cysts seen on US. Approximately 20 percent of these cysts are larger than 9 mm. Fetal gonadotropins (follicle-stimulating hormome [FSH] and luteinizing hormone [LH]) decrease during the last trimester of pregnancy, but increase subsequently after birth. FSH and LH levels in the newborn peak at 3–4 months of age, most likely in response to the postnatal fall in estrogen.
Ovarian cysts are the most common cystic abdominal masses seen in newborn girls, given the frequency of small cysts detected with US. 4 The differential diagnosis of intra-abdominal cystic masses in newborn girls includes ovarian cysts, gastrointestinal duplications, mesenteric cysts, urachal cysts, omental cysts, and renal cysts. 5
Cysts of any size that are complex, with multiple septa, solid components, or hemorrhaging, should be followed carefully or treated. The presence of a single septum or presence of a “daughter cyst” is common in simple cysts and does not warrant the diagnosis of a complex cyst. Any neonatal simple cyst > 2–2.5 cm should be followed carefully or treated.6,7
Simple ovarian cysts < 4–5 cm in diameter should be observed, as there is a high likelihood that these will resolve spontaneously. There is more controversy about the management of large simple cysts (>4–5 cm in diameter) and complex cysts. Surgical treatment and US aspiration are indicated for simple cysts > 5 cm to prevent ovarian torsion.8,9
Neonatal complex cysts are usually the result of perinatal ovarian torsion or prenatal hemorrhaging into a cyst. Given that the risk of malignancy is essentially nonexistent, there is no mandate to remove complex cysts surgically in neonates. In the modern era, there are few reported cases of malignancy in a neonatal ovarian mass or cyst. In fact, the only reported case of malignancy in a neonatal ovarian mass was made in 1945. 10 This was a case of bilateral “ovarian carcinoma” reported in a 30-week stillborn. Although malignancy is not a concern in a newborn with an ovarian mass, benign cystic teratomas, although rare, can occur in newborns. Failure of a neonatal cyst to resolve, particularly if there are any solid components seen on US, should raise the possibility of a benign cystic teratoma and should lead to surgical intervention. The youngest patient with a malignant teratoma—by far the most common malignancy of the ovary in children—was 14 months,7,11 while Katara et al. described a newborn with gonadoblastoma, antenatal diagnosis of a complex cyst with multiple septa; this patient was was operated on in the fourteenth day of her life. 5 Gonadoblastoma is a rare tumor in children, occurring either in children with intersex disorders or with abnormal gonads. No data are published on the race distribution of this condition. These tumors are normally more frequent in phenotypic females who have a genetic karyotype with a Y chromosome. Nearly all of patients who develop gonadoblastomas have chromosomal anomalies consistent with an intersex syndrome, and the genotypic sex is frequently inconsistent with the phenotypic appearance. In particular, 80% of gonadoblastomas occur in phenotypic females with intra-abdominal testis, while the remaining 20% occur in patients who have other conditions involving intersexuality. 5 Three fourths of the gonadic tumors arising in dysgenetic gonads are gonadoblastomas. 12 Scully reviewed 74 cases and found that 89% were chromatine-negative and had a karyotype of 46XY or 45X/46XY. 13 Troche and Hernandez in a literature review of 140 cases of neoplasms arising in dysgenetic gonads found that 80% had these karyotypes. 14 Patients are usually older adolescents or in the third decade of life with a history of primary amenorrhea. Androgen production by the tumor causes amenorrhea. 15
These small tumors may be found incidentally during excision of gonadic streaks or dysgenetic gonads. The tumors become invasive early, and gonadectomy is recommended as soon as 46XY gonadic dysgenesis is diagnosed. A person's predisposition to develop gonadoblastoma exists early in life. It is generally diagnosed before the age of 20 usually as a result of investigation of ambiguous genitalia or amenorrhea. Approximately 40% of gonadoblastomas are bilateral. These tumors are often associated with invasive germinoma (50% of reported cases) or with other forms of germ-cell tumors (embryonal carcinomas, chorocarcinomas, yolk-sac tumors) in 8%. The tumors range in size from microscopic (the current case) to as large as 8 cm in diameter. Histologically, the tumor is composed of nests of immature germ cells admixed with smaller sex cord cells. 16 The first type is similar to the large germ cells found in dysgerminoma/seminoma.
The second cell type resembles small immature Sertoli cells. In addition, a third type of cell can frequently be seen in the stroma of the tumor and is nearly identical to the Leydig cells, with the exception of having visible Reinke crystals. The two main cell types form discrete solid aggregates that often contain calcifications. If the germ cells invade the margins of these discrete aggregates, the lesion is no longer considered benign and is considered to be a dysgerminoma/seminoma. With advanced local growth, the dysgerminoma/seminoma nearly obliterates the architecture that characterizes the benign histologic features of the gonadoblastoma. Approximately 17% of germinomas arising in gonadoblastomas are bilateral. Treatment for an individual with gonadoblastoma is surgical, and the main complications observed are related to the wound (e.g., infection). The prognosis of patients with gonadoblastoma is excellent if the tumor is removed before it transforms into a malignant germinoma/seminoma occurs.
Conclusions
This article described the first case of a pure neonatal gonadoblastoma in a patient with a normal 46XX karyotype and no dysgenetic gonads. Surprisingly, there was a micro area of gonadoblastoma in a normal follicular cyst that did not have a solid area but only one septum. No signs of complication of the cyst were present. Salpingo-oophorectomy was, however, necessary because this is required by the oncologic protocol for treating this kind of tumor.
A case of gonadoblastoma without a Y chromosome is very rare. A case of gonadoblastoma with dysgerminoma in one ovary and a gonadoblastoma with dysgerminoma and a yolk-sac tumor in the contralateral ovary has been reported in a 46 XX 10-year old girl. 12 The prognosis for gonadoblastoma is good because pure gonadoblastoma does not metastasize. The current patient was followed with US scanning in the following months and years, and these tests yielded negative results for ovary neoplasms. As of this writing, the patient is now 9 years old, in good health, with a normal left ovary (as seen on US). There were no sequelae after the treatment she had received 9 years ago.
Footnotes
Disclosure Statement
No competing financial conflicts exist.