
Abstract
Abstract
Introduction
Innovations in laparoscopy have made it possible to decrease the numbers of hysterectomies via the abdominal approach. In 2003, hysterectomies in the United States were still being performed abdominally more than 70% of the time. 2 In 2005, abdominal hysterectomies were performed 64% of the time; 14% percent of these were laparoscopic and 22% were vaginal. 3 The current trend in gynecologic surgery seems to be more minimally invasive surgical procedures and fewer abdominal procedures.
The American College of Obstetricians and Gynecologists (ACOG) recommends a physician preference for surgical approach while suggesting consideration of the vaginal approach. 4 The American Association of Gynecologic Laparoscopists (AAGL) position statement recommended that surgeons “minimize abdominal approach and encourage minimally invasive techniques.” 5 Vaginal, laparoscopic, and robotic-assisted surgery are all consistent with shorter hospital stays, faster patient recovery, minimized blood loss, reduced infections, and increased patient satisfaction compared to open abdominal surgery. 6 Surgical training for gynecologic surgeons should strive to produce confident, well-trained physicians with broad surgical experience that is consistent with current surgical advances.
In 2004, the U.S. Food Drug Administration approved the daVinci tool (Intuitive Surgical, Sunnyville, CA) for use. The daVinci robotic-assisted surgery technique was a revolutionary operative tool utilized by many surgical specialties. Gynecologic surgeons have been in the forefront of using the technique to treat female patients.
Over the past 3 years, surgeons at the Miami Valley Hospital, in Dayton, OH, performed 30%–40% of benign hysterectomies using the daVinci robotic system. As a result of the increased use of robotic surgery as a viable option for hysterectomy procedures, the need to incorporate robotic-assisted surgery into the hospital's gynecologic education curriculum materialized. Currently, gynecologic surgeons typically receive 8 hours of postresidency training, with a significant portion of the training involving animals in laboratories.
A few residency programs provide training in robotic surgery; however, most of this training is limited and does not involve formal or simulated surgical education. In general, residency training was designed on an apprenticeship-type model (“see one, do one, teach one”). Although residents can be trained adequately with this model, many educators believe that resident training should consist of other facets such as: technical aspects, basic skills, knowledge, and evaluation. General surgery has implemented an educational program related to laparoscopic surgery. 7
The goal for the authors' surgical education program was to formally incorporate robotic-assisted gynecologic surgery into the standard 4-year gynecology curriculum. In addition, the authors recommend including robotic-assisted surgery into the required resident's case list of procedures. The authors believe that their robotic-assisted gynecologic surgery training program combines a solid educational approach with new surgical techniques.
Materials and Methods
Several educators and their desire to improve medical education influenced the authors' educational design for robotic-assisted gynecologic surgery training. The authors believe that surgical education should be innovative and that good surgical teaching should include at least five aspects: (1) knowledge; (2) basic skills; (3) experience; (4) decision-making skills; and (5) performance and evaluation (Fig. 1).7–9
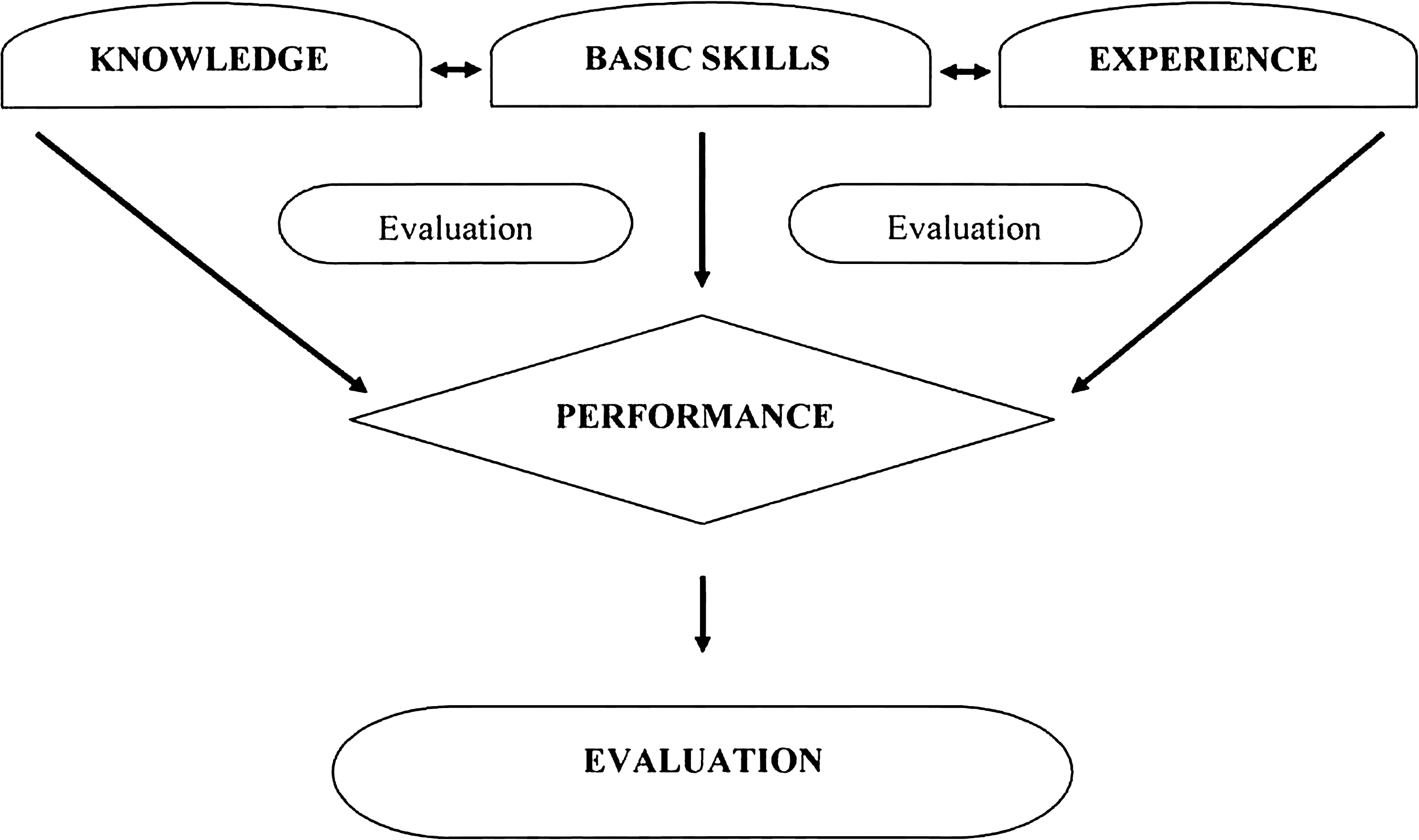
Educational Program Scheme.
The course design and evaluation was approved by the department of obstetrics and gynecology program curriculum committee and by the Miami Valley Hospital's institutional review board. The training was applied when consent was obtained from patients who were scheduled for robotic surgery, and the residents worked under direct supervision and monitoring by expert faculty members.
The obstetric and gynecologic residency-training program included a total of 24 residents (6 residents per year) with ∼70% of the surgical training being performed at a large tertiary-care university-affiliated community hospital. The gynecologic surgery rotation included 4 residents (1 per each postgraduate year [in years 1–4]) and lasted 8 weeks.
The robotic-assisted gynecologic-training began with a knowledge-based educational approach that included lectures regarding the surgical application of robotic assistance and one online tutorial of the schematics and functions associated with the daVinci robotic system.
The basic skills component of the training comprised developing both hands-on familiarity with the robot, and port placement and docking. The basic skills included: setting-up the robotic system; simulation drills with camera mobility; dexterity training; achieving maneuverability; needle manipulation; suturing; and dissection. The simulation equipment for this activity was developed by the Chamberlain Group, LLC, in Great Barrington, MA, and cost approximately $1,000. Faculty members trained in robotic surgery observed, taught, and evaluated residents during skills-drill training and surgical procedures.
Maneuvering a camera drill on the Whoville pod simulation, each resident rotated the camera to the right and to the left and practiced focusing closer and farther away to become familiar with the camera's ability. Once proficient in the above tasks, the resident picked up one ring and passed it from the right hand to the left hand using a needle grasper. During this activity, the resident visualized the needle driver's ability to grasp and compress the object, and determined the amount of pressure required to achieve proper control of the ring without over- or undergrasping.
The program was designed to use reasonable surgical-task models as part of the basic-skills training and was designed to be cost-efficient (<$1,500). However, many educators use simpler tasks-models that can be made with old or discarded materials. The main point of these choices was to set up basic-skills tasks that allowed residents to develop both physical skills and gain cognitive education.9–11
During the basic-skills training, the first activity, Whoville, involved placing rings on various colored “mountains.” Two points were assigned to each basic-skills portion of this task. The task started with fifteen different colored rings. The resident was to place a ring on the mountain, based on the color of the closest corresponding mountain. For instance, a green ring was supposed to be placed on a green or yellow mountain, a red or orange ring was supposed to be placed on a red or orange mountain, and a blue ring was supposed to be placed on a blue or purple mountain. The activity was timed and evaluated, based on the number of times the ring was dropped; 3 seconds were added for each individual drop.
The second activity was called the Ring Jump. Rings were supposed to be placed on several spaces, with one space left open. The resident was to jump a ring with one hand and remove the ring that had been jumped with the opposite hand. This process was continued until no further jumps were available. Jumps could be straight, lateral, or at an angle >90°, and the goal was to leave one ring at the end of the task. Three seconds were added to the total time for each additional ring remaining.
The third activity was the most challenging. It involved an S-hook pod using a small suture, usually a 3-0 Vicryl on a SH needle. There were ten hooks to be completed. The resident started at hook 1 and passed the needle by the hook, using both hands enabling him/her to manipulate the needle and gently follow the curve that passed through the hook. This was done consecutively through the ten hooks. The activity required the resident to exercise effective attention to detail; therefore, the resident was evaluated based on how well he/she observed the successive changes that transpired during suturing. This activity was timed and evaluated based on the degree of difficulty and the number of times the needle was dropped, although the emphasis was placed on assessing control of the needle through the process.
The fourth activity involved suturing a straight incision (i.e., a vaginal-cuff closure). The suture is a figure eight with four-knot throws placed. The resident was allowed to practice the first figure-eight suture. The second figure-eight suture was then timed. Evaluation was based both on the time and the quality of the suture placement related to strength and cohesion.
The residents underwent four, 4-hour basic-skills training sessions (totaling 16 hours). Three of the sessions occurred in the first 2 weeks of their first gynecologic rotation (Table 1). The fourth session occurred midway through the rotation (Table 2).
The next portion of the program involved surgical decision-making skills and robotic experience. Dissection was performed using chicken and turkey samples, after which the resident was ready to assist in a live surgery.
The live surgeries were performed by both fully affiliated and clinical faculty members. Each resident was expected to assist in a minimum of five robotic surgeries enabling that resident to incorporate initial knowledge and basic-skills training with actual performance while assisting in a live surgery. During this assistance, the residents had the opportunity to perform any portion of the surgery allowed by the primary surgeon, including a portion of the dissection and some suturing of the vaginal cuff. Third- and fourth-year residents (PGY 3 and PGY 4) were allowed to schedule patients from their own clinics for robotic-assisted gynecologic surgery after completing 4 weeks of their 8-week gynecologic surgery training and their surgical performance was supervised by a fully affiliated faculty member.
An evaluation was done after each surgery was performed. Conducted by an objective, affiliated faculty member, the resident was graded on his/her surgical performance. This surgical program was designed to produce residents who had performed as the primary surgeon of a robotic-assisted surgery at least five times throughout the completion of residency training and would have also assisted in approximately 50 other robotic cases. At the completion of the gynecology surgery rotation, a global evaluation was performed as required by the Accreditation Council for Graduate Medical Education (ACGME).
Results
Residents completed online daVinci robot training and received a certificate of completion for their training. In addition, they completed the basic-skills portion of the training and executed surgical procedures successfully (Tables 1–3).
Statistically significant.
A comparison was made among the four pod simulations: Whoville apparatus, ring jump, S-hook, and suturing. Repeat assessments showed a vast improvement between the two training attempts. The robotic-training program enabled residents to assist and perform surgery. Fourth-year residents assisted in sixty-six robotic surgeries and performed seventeen of these surgeries. In total, residents assisted in 103 and performed 25 robotic surgeries during the first year of the curriculum.
Discussion
Many residency programs are allowing residents who are interested to obtain robotic surgery exposure via assisting or performing portions of robotic surgery cases. While this may give residents familiarity with robotic-assisted surgery, it is not the most structured educational approach.
The concept of this program is to incorporate all necessary components of structured education into surgery: knowledge of the equipment and the type of surgery along with basic-skills training using simulation type models, combined with experience and the decision-making skills involved in live surgeries. The evaluation is vital in quantifying the residents' progress as well for determining their ability to perform robotic surgery. The basic components of surgery regarding dissection, knot tying, visualization, exposure of the surgical field, and awareness of the surrounding anatomy are extremely important for any surgical method; therefore, this program was designed to enhance the resident's education in robotic assisted surgery and also enhance their overall surgical education.
This program was designed to implement gynecologic robotic-assisted surgery into the residency program as formal training including skill-simulation training in actual gynecologic surgery with five aspects covered: (1) knowledge; (2) basic skills; (3) experience; (4) decision-making skills; and (5) and quality performance and evaluation (which is conducted during each step of the training process).
The evaluation results demonstrated that the authors' structured program offered ways to achieve positive surgical results (Fig. 1). Residents at every program year level were able to familiarize themselves with and perform successfully robotic-assisted surgery. Robotic-assisted gynecologic surgery has many advantages over basic laparoscopic surgery, and is not simply “a new product” but a minimally invasive method that has been utilized for several years.12,13
The authors observed, quantified, and compared the results of the robotic training. The results showed improvement across the different basic skill tasks in all resident year levels. Improvement was also seen from the midway point of skills training to completion. The ring jump task had the narrowest range of improvement. The most plausible explanation for this finding is that this activity involves an extra cognitive component and is not solely based on time but also on the number of rings left behind during the activity. Although the total times were relatively short, the additional cognitive aspect may have required and added some small amount of time. The S-hook activity showed a significant improvement from time 1 to time 2.
With respect to all activities, the upper-level residents (PGY3 and PGY4) demonstrated more skills and were able to complete the basic tasks as expected because they had more surgical experience in general. The residents showed improvement in familiarity with the daVinci robotic system and with simulated activities. During this time the residents also gained experience by assisting on various cases with fully affiliated and clinical faculty members. The upper-level residents were able to perform on approximately 5 cases as primary surgeons using robotic-assisted gynecologic surgery. As stated previously, residents performed or assisted in 25 and 130 cases, respectively. Although not looking at a primary outcome of this study, a review of the cases performed by residents included the following: no vaginal cuff dehiscence; blood loss less than 100 mL (in all cases); 1 sigmoid injury (stage IV endometriosis, recognized and repaired at surgery); and 1 readmission nonsurgical-related (for chronic obstructive pulmonary disease).
As expected, the upper-level residents (PGY3 and PGY4) showed the most “skill” in simulation training and developed increased comfort and familiarity with the tasks involved. The PGY1 and PGY2 year residents showed significant improvement midway through their training.
Robotic surgery, in general, has a limitation of the inability for haptic sensation. In the authors' educational program an attempt was made to teach “Visual Haptics,” which is the individual surgeon's ability to observe and focus on the surrounding tissues to note their reaction to and displacement by the manipulation and forces that the robot provides. Teaching Visual Haptics has proven to be an asset during training. The ability to be aware of the surrounding tissues is important for maintaining proper surgical technique in limited displacement of traction on surrounding tissues. This is important for homeostasis, proper dissection, and surgical healing.
One question that has been raised is: “Can residents with this training be qualified or considered competent in robotic surgery?” Surgical competency is a question postulated by hospitals nationally and, currently, there are not consistent recommendations published. At the authors' institution, a minimum of 5 cases performed with supervision is required to be considered competent in robotic surgery. This is followed with a requirement to participate in a combination (observed/performed) of 10 additional cases in 6 months to obtain robotic surgical privileges. Based on these requirements, the initial fourth-year class would not meet the author's hospital's current standards. It is anticipated that future residents may to be able to meet the above requirements with the continuation of the robotic-training curriculum.
Incorporation of robotic surgery in this manner has enabled the residents to participate in more surgical cases than they had before the facility acquired a daVinci robot. The residents still have adequate exposure and training to abdominal, vaginal, and other laparoscopic minimally invasive approaches.
Conclusions
The goal for this surgical education program was to incorporate gynecologic robotic-assisted surgery formally into the standard 4-year gynecology curriculum. In addition, the authors propose including robotic-assisted surgery into the required resident's case list of procedures. The >150 cases in which these residents performed or assisted in were surgical cases, in the previous 2 years. This opportunity to gain experience in robotic-assisted surgery was not available to these residents prior to implementation of the training curriculum. The authors believe their robotic-assisted gynecologic-surgery training program combines a solid educational approach with new surgical techniques. This educational program for residency training in robotic-assisted gynecologic surgery is a structured approach to expanding surgical education in minimally invasive techniques. Gynecologic surgery should improve patient care, patient satisfaction, and a patient's ability to resume normal activities sooner in the safest possible way by decreasing complications, blood loss, and healing time. As gynecologic educators, we have a duty to patients to train residents properly by including more advanced surgical techniques into surgical residency training.
Footnotes
Disclosure Statement
No potential financial conflicts exist.