
Abstract
Abstract
Introduction
There are no definitive or standard treatment options for high-grade cervical stenosis after conization. Two cases of recurrent cervical stenosis secondary to conization and effective management by using a Malecot nephrostomy drain are reported (C.R. Bard, Inc., Germany).
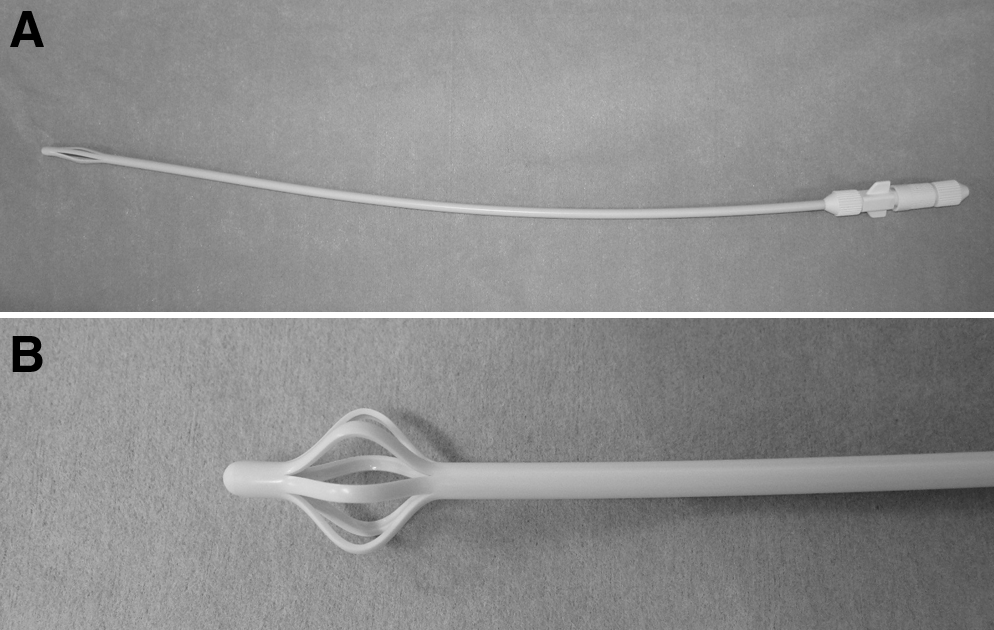
A Malecot catheter is usually used as a nephrostomy drainage catheter and ureteral stent. When the flexible stylet is withdrawn, the extendable wing is opened, thereby providing enhanced drainage and promoting the catheter stent retention (Fig. 1). The use of a Malecot catheter as a stent for recurrent cervical stenosis after conization has not been described previously.
(
Case 1
A 42-year-old unipara who had been treated by cervical conization for CIS and had had regular surveillance by the regional gynecologic oncology team, presented 4 years later with hematometra with menstrual cramps that occurred every period, and was transferred to Minoh City Hospital. She had previously had a cesarean section.
At initial presentation, the patient's uterine cervix was occluded. The external os of the uterine cervix was obliterated, in which uterine sounding was impossible even aftr she had been given a suppository painkiller. Cervical stenosis associated with hematometra was diagnosed with ultrasound (Fig. 2).

Transvaginal ultrasonogram of a hematometra in case 1, showing enlarged uterus with fluid collection.
After a discussion with the patient regarding several options, such as cervicoplasty, insertion of a stent, and hysterectomy, she underwent cervical dilatation and insertion of a drainage tube under anesthesia. The hematometra was evacuated after cervical dilatation to Hegar 10. A surgical drain was inserted into the uterus, of which 5 cm was in the uterine cavity, and then secured in the cervical canal with two resorbable sutures. Two weeks later, the catheter spontaneously slipped out of the uterus. Ultrasonogram showed no fluid accumulation in the uterus (Fig. 3). At the time of her expected next menstruation, however, she developed abdominal cramping without any bleeding. Under transvaginal ultrasound, the uterus was enlarged up to a length of 7.8 cm proximal to the stenosis (Fig. 4). The patient was diagnosed with recurrence of symptomatic cervical stenosis. Because she wished to have the minimum procedure instead of a hysterectomy, informed consent was given by the patient and it was decided to perform dilatation of the cervical canal and insertion of a silicone Malecot catheter. After the cervical canal was dilated to Hegar 6, a 14-Fr Malecot catheter was passed through into the uterine cavity and held in place. The patient was discharged the following day.

Ultrasound image showing no fluid accumulation after 2 weeks of drainage.

One month after removal of drainage with a surgical drain, transvaginal ultrasonography shows relapse of hematometra at the time of expected menstruation.
Seven months later, the catheter was replaced with a new one to avoid infection, and cervical cytology was performed. Histology revealed no evidence of atypical or malignant cells in cervix and endometrium. A subsequent examination was performed every 4 months. One year after the second placement, the Malecot catheter was removed.
At the time of her expected next menstruation after removal, the patient developed symptomatic cervical obstruction again. The Malecot catheter was the placed for the third time. Postoperatively, the patient has been examined every 4 months and the catheter has been replaced with a new one once a year. Since the third insertion of the Malecot catheter, she has been afebrile and symptom free for ∼2 years.
Case 2
A 36-year-old woman, gravida 2, para 2, was diagnosed with CIS by directed punch biopsies and underwent conization at a university hospital. She had previously had a cesarean section. She had been treated for epilepsy and depression with sedatives and antidepressants. Histology revealed microinvasive cervical cancer stage Ia1; 1 mm-invasion, negative margin. The patient was then followed regularly by use of serial cervical cytology smears. Two years after surgery, she developed severe abdominal cramping without any bleeding. She was diagnosed with cervical stenosis and hematometra. After the cervical dilatation, a urethral catheter was placed in the cervical canal for 1 year. After the removal of the catheter, the patient gradually began to experience dysmenorrhea but had a regular menstrual cycle. Three years later, sh developed symptomatic cervical stenosis again. She was transferred to Minoh City Hospital for her management.
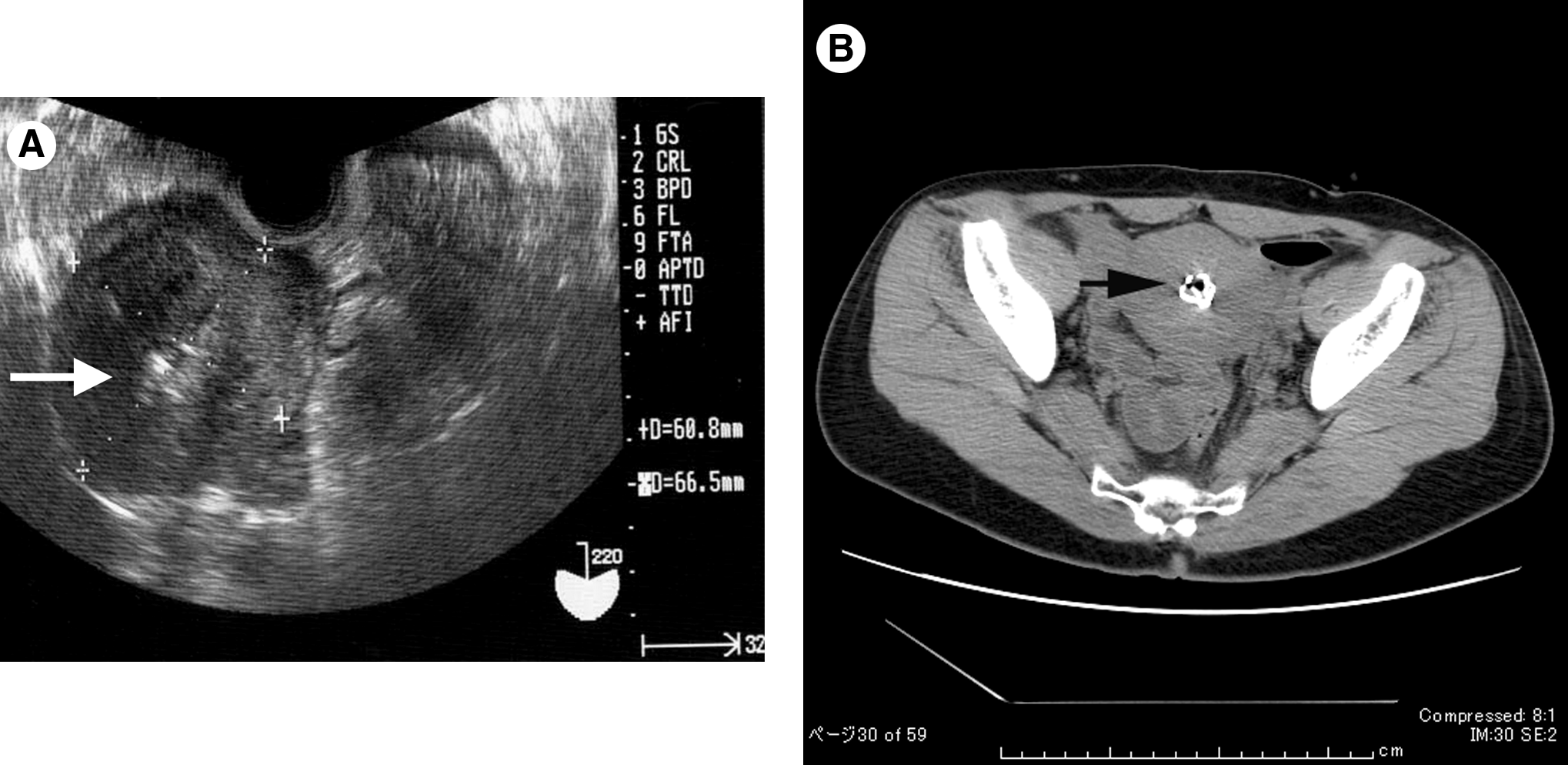
Pelvic examination revealed a totally occluded and shortened residual cervix. Transvaginal ultrasonic examination revealed fluid collected in the uterus and a shortened cervix (Fig. 5).

Transvaginal ultrasonography in case 2 at the first visit, showing hematometra and suspected location of obliterated external os (arrow).
A diagnosis of repeated cervical stenosis was made. After proper counseling and obtaining written informed consent, dilatation of the residual cervical canal and insertion of a Malecot catheter was the procedure chosen. With the patient under spinal anesthesia, the external os of the uterine cervix was fixed with a grasping forceps and dilated to Hegar 7. Cytologic specimen from the cervical wall was taken and the specimens were sent to pathology. A 14 Fr silicone Malecot catheter stent was inserted into the uterine cavity (Fig. 6). Histology demonstrated no recurrence of cervical disease. The localization of the stent was controlled by sonography and/or CT (Fig. 7). The catheter was cut short to leave the distal end protruding from the external os without emerging from the introitus. The following menstruation after replacement did not cause any pain or disorders.

Inserted Malecot catheter in the cervical canal.
Transvaginal ultrasonography
After 12 months, the stent was removed and a second manipulation using the same instrument was performed, with the patient under spinal anesthesia, without any complications. The stent has been replaced with a new Malecot catheter every year, resulting in long-term patency. Up to the time of this writing, there have not been any problems for 3 years.
Results
Placement of a Malecot catheter in the uterine cavity was performed for the 2 patients with recurrent cervical stenosis after conization. Relief of symptoms has been achieved in the patients. There was no evidence of recurrent cervical stenosis at follow-up in both of the patients.
Discussion
The incidence of symptomatic cervical stenosis secondary to cervical excision procedure resulting in hematometra is not a frequent complication. However, once it happens, it may cause a severe situation such as monthly abdominal cramping and infertility. The frequencies of cervical stenosis mentioned in the literature are 0–25%3,7 after laser conization and 1.3%–5.2%3,8,9 after loop excision. Baldauf et al. reported that the depth of surgical excision was associated with a high probability of cervical stenosis. 3 In some reports, the risk of postoperative cervical stenosis has been described to be increased when patients were older.10,11
Management of cervical stenosis after conization or electrosurgical procedures is not established.
The Malecot catheter, a nephrostomy tube, is distinguished by an extendable wing on the end of the catheter. After the stylet is withdrawn, the wings spread, resulting in stabilization of the catheter in place. Its distinctive shape can reduce the risk of slip and is ideally suited for the drainage of thick viscous fluids.
This catheter has been a useful instrument for several clinical conditions as well as for nephrostomy drainage. For example, Mason et al. reported that transperitoneal drainage with a suprapubic Malecot catheter under transperineal ultrasound guidance successfully treated a patient with septic shock secondary to prostatic abscess. 12 Another possible use for the Malecot catheter is evacuation of air. Recently, intrauterine air embolism associated with a rectovaginal fistula in a pregnant woman was successfully treated by continuously draining the vaginal air by using an intravaginal Malecot catheter. 13 The Malecot catheter was also reported to be used for fertility treatment. The insertion of a Malecot catheter in the uterine cervix was performed for these patients, who had histories of difficult intrauterine insemination (IUI) or embryo transfer (ET), to facilitate IUI or ET. Yanushpolsky et al. reported transcervical placement of the catheter for ∼10 days allowed easier access to the endometrial cavity during IUI or ET. 14
In the case presented in the current article, temporary insertion of a surgical drain or urinary catheter in the uterine cervix was initially successful; however, cyclical abdominal pain and reaccumulation of blood in the uterine cavity with amenorrhea occurred after removal of the catheter. The patient wished to pursue another option instead of having a hysterectomy. Therefore, a stent to provide a continuous route for distal passage of menstrual flow into the vagina needed to be identified for this patient and others. Because of the higher possibility of success and the lower risk to patients, the Malecot catheter was chosen. Both patients have had regular menstruatal cycles because long-term patency was achieved by using the Malecot catheter stent. This is the first report of the use of Malecot catheter for the management of symptomatic recurrent cervical stenosis secondary to conization.
It was initially difficult to identify the external os and to insert devices to obstruct the cervix, such as Hegar or catheter. Because of resistance at the first insertion, it was uncertain whether the catheter was successfully placed in the uterine cavity even under abdominal ultrasonic guidance. However, subsequent replacement of the catheter was much more straightforward, even though the opening was still barely detectable.
One limitation of this management is that although the catheter is cut short in the vagina, patients may feel discomfort from the tail edge rubbing against the vagina. Furthermore, the patient's partner could have the feeling of a foreign body during intercourse, and there have not been any reports regarding spontaneous fertility under this condition. Lastly, although this method can provide a route for menstrual blood out of the vagina monthly, there can be a potential risk of uterine infection by stable placement of the stent. Because there are few reports regarding long-term placement of any catheter in the uterus, oral antibiotics were administered prophylactically for <1 week when the catheter was placed. There have not been any associated long-term complications or pelvic infection.
Conclusions
In conclusion, Malecot catheter placement appears to be a valid alternative in the treatment of recurrent cervical stenosis after conization.
Footnotes
Disclosure Statement
No competing financial conflicts exist.